
The role of preoperative dutasteride in reducing bleeding during transurethral resection of the prostate: A systematic review and meta-analysis of randomized controlled trials
2022-03-25 06:40:52YudhistiraPradnyanKlopingNiwandaYogiswaraYusufAzmi
Asian Journal of Urology 2022年1期
Yudhistira Pradnyan Kloping, Niwanda Yogiswara, Yusuf Azmi
Universitas Airlangga Fakultas Kedokteran Ringgold Standard Institution, Jawa Timur, Indonesia
KEYWORDS Dutasteride;Benign prostatic hyperplasia;Bleeding;Transurethral resection of the prostate
Abstract Objective: Bleeding is one of the most common complications of transurethral resection of the prostate(TURP).Several previous studies reported that administering dutasteride before surgery could reduce perioperative bleeding.We aimed to evaluate the efficacy of preoperative dutasteride treatment in benign prostatic hyperplasia patients undergoing TURP by performing a meta-analysis of relevant randomized controlled trials (RCTs). Methods: A comprehensive literature search was performed through the electronic databases including Medline, Cochrane Library, Google Scholar, and ClinicalTrial.gov in October 2020.RCTs evaluating the role of dutasteride for TURP were screened using the eligibility criteria and the quality of RCTs was assessed using the Cochrane Risk of Bias Tool.The heterogeneity was assessed using I2 statistic.The measured outcomes were hemoglobin (Hb) levels, perioperative blood loss, blood transfusion, microvessel density (MVD), and operation time.Data were pooled as mean difference (MD) and odds ratio (OR). Results: A total of 11 RCTs consisting of 627 samples from the treatment group and 615 samples from the placebo group were analyzed.Patients that received dutasteride had less reduction in Hb levels (MD-1.10, 95%confidence interval[CI] -1.39 to-0.81, p<0.00001).Dutasteride also significantly reduced the operation time(MD-1.79,95%CI-2.97 to-0.61,p=0.003)and transfusion rate after surgery(OR 0.34,95%CI 0.15 to 0.77,p=0.009)compared to the control group.However, the MVD (MD -3.60, 95% CI -8.04 to 0.84, p=0.11) and perioperative blood loss in dutasteride administration for less than 4 weeks (MD 46.90, 95% CI -144.60 to 238.41,p=0.63) and more than 4 weeks (MD -190.13, 95%CI-378.05 to -2.21, p=0.05) differences were insignificant.Conclusion: Preoperative administration of dutasteride is able to reduce bleeding during TURP,as indicated by less reduction in Hb level, lower transfusion rate, and less operation time.
1.Introduction
One of the most common urological diseases affecting the aging male population is benign prostatic hyperplasia (BPH)[1].The progressive nature of the disease, generating a prostatic growth rate of 2.0%-2.5% per year in older men,causes a substantial impact on the quality of life for numerous patients [2].In order to manage the disease, there are a plethora of options available to urologists ranging from pharmacological treatments to surgical interventions [3].BPH patients who do not respond to pharmacological modalities,often undergo transurethral resection of the prostate(TURP)as the gold standard surgical treatment [4].Despite the technical and instrumentation improvements to the method,it is still associated with a number of complications [5].Bleeding is one of the most prevalent and severe complications of TURP.Persistent bleeding may lead to serious lifethreatening complications such as postoperative blood clot retention and hypovolemic shock [6].These complications could prolong the patient’s length of stay as well as increasing the need for potential blood transfusion[7].Thus,being able to reduce the risk of bleeding is considered as a significant benefit for BPH surgery[8].Several methods have been suggested to reduce the amount of bleeding.Improving the operator’s skill and surgical technique as well as utilizing novel resection devices like laser-equipped or bipolar scopes have been shown to be beneficial in lessening the risk of complications[9].Non-surgical methods have also been studied,one of which is the use of preoperative 5-alpha reductase inhibitors(5-ARIs),which was claimed to exhibit favorable results [10,11].Finasteride and dutasteride are 5-ARIs administered to inhibit the conversion of testosterone(T)to dihydrotestosterone (DHT).Apart from the daily use as pharmacological treatments for BPH, they are also used to manage hematuria associated with the disease[12].This effect was achieved by reducing the growth of prostatic tissue and suppressing the androgen-controlled vascular endothelial growth factor(VEGF),which results in reduced angiogenesis and less prostatic bleeding[13-15].Even though the drug has displayed promising results for prostatic bleeding management in a clinical setting,only 4%of urology consultants in the UK use them as a routine preoperative treatment in reducing blood loss during TURP [16].This is because its role is still considered unclear [17].Previous meta-analyses conducted have demonstrated that preoperative finasteride administration could decrease hemoglobin (Hb) reduction and hematocrit levels, but the study failed to demonstrate the benefits of dutasteride to decrease total blood loss during TURP[18].However,only two studies evaluating dutasteride were included in the analysis to classify the perioperative blood loss [19,20].In this study, we performed an updated analysis involving the latest relevant available randomized controlled trials(RCTs)to evaluate the efficacy of preoperative dutasteride administration for reducing surgical blood loss in BPH patients.
2.Materials and methods
2.1.Search strategy
A comprehensive literature search was performed through the electronic databases including PubMed, Cochrane Library,Google Scholar,and ClinicalTrial.gov in October 2020 following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines as shown in Table 1.MeSH terms correlated with dutasteride and TURP were used to search relevant studies.The full search strategy was summarized in the supplementary material table S1.There were not any language or other restrictions during the search.The study search and selection were independently performed and cross-checked by two reviewers(Kloping YP and Yogiswara N).Any disagreements were resolved by a discussion between the reviewers.The number of screened and included literature was shown in Fig.1.

Table 1 Characteristics of included studies for meta-analysis.
2.2.Eligibility criteria
Studies were considered eligible if they met the following criteria:All accessible RCTs, evaluating subjects with BPH undergoing monopolar or bipolar TURP, who received preoperative dutasteride compared to placebo or no preoperative treatment.The evaluated outcomes should include: Perioperative blood loss, Hb level, microvessel density (MVD), operation time, or blood transfusion.We excluded studies that have inaccessible full texts, irrelevant outcomes, or subjects with bleeding disorders.
2.3.Data collection and statistical analysis
All studies were included based on the eligibility criteria and assessed manually for duplication.The quality assessment of the included study were undertaken using the Cochrane Risk of Bias Tool [21].The formula developed by Hozo et al.[22] was utilized to calculate the mean and standard deviation (SD) of the studies that displayed continuous outcome using median and range values.Heterogeneity of the studies was evaluated by I2statistic.The heterogeneity was considered to be significant if I2is morethan 50%.A fixed-effect model was selected for the analysis if the heterogeneity was observed to be insignificant.Otherwise,a random-effect model was selected.If p-value<0.05, we considered the difference as statistically significant.The meta-analysis was performed using statistical software RevMan 5.3 by Cochrane Collaboration, Oxford,United Kingdom.

Figure 1 PRISMA flowchart of the screening process and included studies.CENTRAL, the Cochrane Central Register of Controlled Trials.PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
2.4.Outcomes
The outcomes evaluated in this study were the change of estimated perioperative blood loss, Hb, MVD, blood transfusion, and operation time.Data were pooled as mean difference(MD)and odds ratio(OR)for continuous data and dichotomous data, respectively.
3.Results
A search flow diagram was presented in Fig.1.An initial 516 titles and abstracts were screened, of which 32 studies were accessed for full-text eligibility.In all, 11 were included for meta-analysis [19,20,23-31].Table 1 presented the summary of the included studies, while Fig.2 summarized the result of bias assessment.Almost all of the studies used the same dose(0.5 mg/day)of dutasteride and only one study used 5 mg/day dose.The duration of the treatment varied from 2 to 8 weeks.Most studies did not specify the type of TURP used in the trials.Only two studies reported using the monopolar and bipolar methods[23,27].Six studies reported prostate with an average volume of 56.1 mL.No study reported any significant difference in terms of postoperative length of stay.There is also no information regarding reoperation for bleeding control from the included studies.
3.1.Perioperative blood loss
Four studies evaluating 518 participants, which were allocated into treatment(n=259)and control groups(n=259),estimated the blood loss during TURP [19,20,23,29].The studies were further separated into subgroups based on the duration of the treatment, more or less than 4 weeks.A random-effect model of analysis was chosen because of significant heterogeneity in both subgroups.Pooled analysis in Fig.3 showed that there was marginal reduction between the group receiving treatment compared to placebo with respect to the perioperative blood loss in the subgroup which were given dutasteride for more than or equal to 4 weeks, but not for the group which were administered the drug for less than 4 weeks (MD -190.13, 95% confidence interval [CI] -378.05 to -2.21, p=0.05; MD 46.90, 95%CI -144.60 to 238.41, p=0.63, respectively) and the combined analysis of both groups (MD -81.94, 95% CI -223.62 to 59.73, p=0.26).
3.2.Hb level
Six studies(775 samples)from both treatment(n=387)and control (n=388) groups reported the Hb level alteration before and after the procedure [25-27,29-31].Pooled analysis showed a significant lower reduction of Hb level in group receiving dutasteride as compared with control (MD-1.10, 95% CI -1.39 to -0.81, p<0.00001).Fig.4 showed that the random-effect model was selected because we found significant heterogeneity among the study (I2=74%).
3.3.MVD
Four studies assessed the changes of MVD which included 573 patients distributed into treatment (n=288) and control groups (n=285) [20,24,27,29].Pooled MD values were estimated using random-effect model due to significant heterogeneity among the trials (I2=98%), resulting in an insignificant difference (MD -3.60; 95% CI -8.04 to 0.84,p=0.11) as shown in Fig.5.
3.4.Transfusion rate
Six studies including 720 participants which were allocated into the treatment (n=366) and control (n=354) group described the number of blood transfusions after TURP[19,20,24-26,29].A fixed-effect model was selected due to insignificant heterogeneity among the trials (I2=0%).Pooled analysis showed that there was a significant reduction in the group receiving treatment compared to placebo in terms of transfusion rate (OR 0.34, 95% CI 0.15 to 0.77,p=0.009), as shown in Fig.6.
3.5.Operation time
Nine studies which include 1086 participants from both treatment (n=545) and control (n=541) groups reportedthe operation time.A fixed-effects model was selected due to low heterogeneity among the trials(I2=42%).The pooled estimate in Fig.7 demonstrated that there was a significant reduction in the group receiving treatment as compared with placebo group in terms of operation time (MD -1.79,95% CI -2.97 to -0.61, p=0.003).

Figure 2 Cochrane risk of bias assessment of the included randomized controlled trials.
4.Discussion
This study reviewed 11 RCTs focusing on the preoperative effect of dutasteride administration in reducing blood loss during TURP.The addition of new studies that have not been analyzed in previous systematic reviews provides interesting new insights to the topic.The pathogenesis of BPH involves the promotion of proliferation and survival of prostatic cells by DHT which has a high affinity to the androgen receptor [32].5-ARI drugs are utilized due to their capability of inhibiting the production of DHT [33].The decision to focus on dutasteride as the intervention in this study is due to the fact that dutasteride is more potent than finasteride in terms of 5-ARI.Finasteride is a monoinhibitor of 5-alpha reductase type 2 at a therapeutic dose, whereas dutasteride is a dual inhibitor of both 5-alpha reductase type 1 and type 2.Dutasteride is 45 and 2.5 times more potent at inhibiting 5-alpha reductase type 1 and type 2 respectively compared to finasteride [34,35].The results of this systematic review are interesting when compared to the previous review conducted by Zhu et al.[18] that found no significant difference of blood loss, Hb level changes, number of required blood transfusions, and operative time between dutasteride and placebo administration.Based on the meta-analysis results of this review,we discovered several blood loss parameters to be significantly different between dutasteride and placebo, while several parameters are shown to be insignificant.
4.1.Perioperative blood loss
Based on the underlying action of dutasteride of inhibiting the angiogenic growth factors to decrease prostate glandvascularization,several studies reported that the drug can be used to reduce blood loss during the operation [20,29].However, there are studies that reported little to no significant difference in perioperative blood loss in patients administered with dutasteride compared to a placebo[19,20,23].Past studies suggested that the duration of treatment seems to be responsible for blood loss results differences among studies.Evidence has shown that dutasteride administration requires 1-2 weeks to achieve maximum serum DHT suppression, which then decreases androgen-controlled growth factors responsible for angiogenesis [29,36].Kravchick et al.[25] suggested that prostate vascularity in the periurethral area was reduced after 6 weeks of dutasteride administration.Bansal and Arora [29] also suggested that in their study, a 4-week prior of dutasteride administration may reduce operative blood loss.Contrary to the previous studies, Hahn et al.[19] reported insignificant difference between the dutasteride and placebo groups in their clinical trial.Similar findings are suggested by Tuncel et al.[20] who claimed that dutasteride administration was not superior to placebo for perioperative bleeding during TURP.By analyzing the results from eligible studies, we found no significant differences of perioperative blood loss between the treated and placebo groups of the included studies as shown by the subgroup treated less than 4 weeks, more than or equal to 4 weeks, and the combined analysis of both groups.Evaluating blood loss based solely on the gross perioperative blood loss during a TURP procedure is potentially inaccurate as the blood volume tends to mix with the irrigation fluid.Therefore, other objective parameters for indicating blood loss are necessary to be evaluated.

Figure 3 Forest plot of preoperative dutasteride effect on blood loss during transurethral resection of the prostate.SD,standard deviation; IV, inverse variance; CI, confidence interval.

Figure 4 Forest plot of preoperative dutasteride effect on hemoglobin change.SD, standard deviation;IV,inverse variance; CI,confidence interval.

Figure 5 Forest plot of preoperative dutasteride effect on microvessel density.SD,standard deviation;IV,inverse variance;CI,confidence interval.
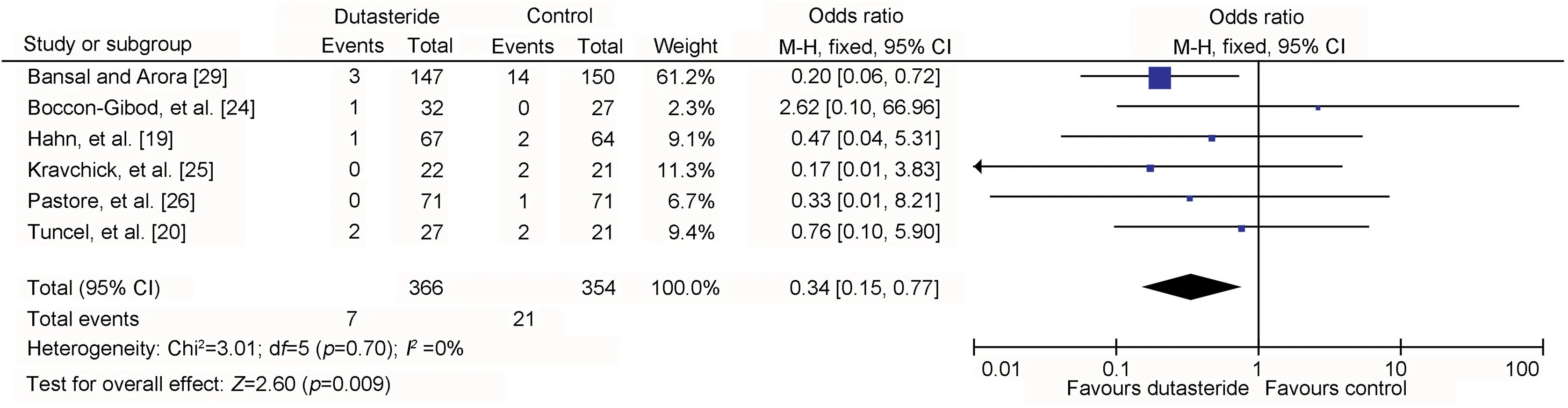
Figure 6 Forest plot of preoperative dutasteride effect on transfusion rate.M-H, Mantel-Haenszel; CI, confidence interval.
4.2.Hb level change
Acute hemorrhage during TURP would cause a direct loss of red blood cells loss.One of the established methods tomeasure this loss is by evaluating the patient’s Hb level[37].Noteworthy results were presented in the study conducted by Rahman et al.[31],in which there are significant postoperative Hb and hematocrit differences between the dutasteride and placebo groups.Bansal and Arora [29] reported higher fall of Hb level of the placebo group compared to the dutasteride group.Similar findings were also reported by Kim et al.[38] and Pastore et al.[26].In this review,we discovered that the decrease of Hb level in the treatment group was significantly lower than the control group based on the analyzed studies(MD-1.10,95%CI-1.39 to -0.81, p<0.0001).In this review, all studies that reported significant Hb change were conducted more than or equal to 4 weeks, indicating that this minimum duration is sufficient to reduce bleeding.Most studies reported significant Hb change reduction regardless of prostate volume.However, Busetto et al.[27] found that dutasteride could only reduce bleeding in large prostate volume (≥50 mL).This result suggests that prostate volume should be considered before administering dutasteride.

Figure 7 Forest plot of preoperative dutasteride effect on operation time.SD, standard deviation; IV, inverse variance; CI,confidence interval.
4.2.1.MVD change
The proliferation of prostatic stromal cells is hypothesized to be promoting angiogenesis.As the histologic indicator of angiogenesis, MVD was used in several studies to evaluate blood loss [39].The increase of vascularity in the prostatic urethra and its closed proximity to mucosa are attributed as the causes of prostatic bleeding during TURP by several studies [40].Certain previous studies suggested that dutasteride is able to alleviate perioperative bleeding by reducing MVD in the hypertrophic tissue of the prostate[41].Studies by Boccon-Gibod et al.[24] and Tuncel et al.[20] both reported that the MVD of the treated group was similar to the placebo group.These findings are similar to the results in this review, in which there was no any significant MVD difference between the treatment and placebo.Canda et al.[42] explained that 5-ARIs reduced hemorrhage in BPH by reducing hyperplasia, which increases the stability of the vessel wall as opposed to decreasing vascularity of the tissue.
4.3.Transfusion rate
Transfusion is necessary in cases where there is major blood loss during the procedure.Thus, assessing the rate of transfusion in a patient is a suitable indicator for estimating blood loss [43].Evaluating the transfusion rate of the studies analyzed in this review, there is a significant difference between the treatment and placebo group (OR 0.34, 95% CI 0.15 to 0.77, p=0.009).Bansal and Arora [29]reported significantly less blood transfusion required for the treatment group compared to the placebo group.This is supported by Hagerty et al.[10] who suggested that patients being administered 5-ARIs would require less blood transfusion based on their study findings.Even though the findings indicated a reduction in blood transfusion requirements, most studies reported no significant reduction in hospital length of stay [19,26,29].
4.4.Operation time
In several operative procedures, the duration of operation is suggested to be correlated with perioperative blood loss[44].Therefore, in studies evaluating the role of dutasteride in reducing blood loss during TURP, the duration of operation was also usually evaluated.The trial conducted by Rahman et al.[31] exhibited results in favor of dutasteride regarding operation time.Bansal and Arora [29] also supported these findings, as indicated by the comparable results between the dutasteride and placebo groups in their study.In this review,we found a significant operation time reduction between the treatment and the placebo group of the analysed studies (MD -1.79; 95% CI -2.97 to -0.61;p=0.003).
4.5.Research limitations and future considerations
The results of the RCTs in general show promising results of dutasteride for reducing perioperative blood loss based on several outcomes.There is a possibility that dutasteride could be implemented as one of the drugs to be considered by urologists when attempting to reduce blood loss during TURP.Unfortunately, during the course of the study, the full-text versions of several literature were not accessible.Secondly, data regarding postoperative outcomes, including hospital length of stay and reoperation rate were limited.Future clinical trials and reviews regarding the topic should take into account additional factors, such as prostate volume, reoperation rate, and hospital length of stay since they are importantclinical aspects for urologists without access to laser technology.
5.Conclusion
Preoperative administration of dutasteride is able to reduce bleeding during TURP indicated by less reduction in Hb levels, lower transfusion rate, and less operation time.
Author contributions
Study concept and design: Yudhitira Pradnyan Kloping,Niwanda Yogiswara.
Data acquisition: Yudhitira Pradnyan Kloping, Niwanda Yogiswara, Yusuf Azmi.
Data analysis: Yudhitira Pradnyan Kloping, Niwanda Yogiswara, Yusuf Azmi.
Drafting of manuscript: Yudhitira Pradnyan Kloping,Niwanda Yogiswara, Yusuf Azmi.
Critical revision of the manuscript: Yudhitira Pradnyan Kloping, Niwanda Yogiswara.
Supervision: Yudhistira Pradnyan Kloping.
Conflicts of interest
The authors declare no conflict of interest.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ajur.2021.05.011.
 Asian Journal of Urology2022年1期
Asian Journal of Urology2022年1期
- Asian Journal of Urology的其它文章
- Atypical small acinar proliferation and its significance in pathological reports in modern urological times
- Subcostal artery bleeding after endoscopic combined intrarenal surgery: Signs and treatment
- Inexpensive and combined technique: Use of suction tracheal catheter and hydrogen peroxide for the evacuation of intravesical clots
- Concurrent laparoscopic management of giant adrenal myelolipoma and contralateral renal cell carcinoma
- Management and evaluation of bladder paragangliomas
- Current insights on haemorrhagic complications in percutaneous nephrolithotomy