
Inexpensive and combined technique: Use of suction tracheal catheter and hydrogen peroxide for the evacuation of intravesical clots
2022-03-25 06:40FredAlainMontelongo-Rodríguez,CarlosDanielGuerra-Catañón,MarioVázquez-Herrera等
Asian Journal of Urology 2022年1期
Dear Editor,
Persistent hematuria could trigger urinary retention,leading the patient to the emergency department for abdominal pain, decreased urinary output, anemia, and azotemia [1,2].Conventional bladder clot evacuation requires a three-way catheter with continuous irrigation and aspiration with a syringe or Ellik evacuator[3].Sometimes a large and well-organized hematoma requires an open cystostomy [1,4].We want to introduce a combined method using hydrogen peroxide as well as suction technique with an endotracheal catheter to evacuate intravesical clots.
A 75-year-old patient diagnosed with locally advanced prostate cancer and a 65-year-old patient diagnosed with muscle-invasive bladder cancer were seen in the emergency department.Both presented with a history of gross hematuria (more than 100 red blood cells per high-power field [RBC/HPF]) with 5 days and 2 days of evolution,respectively, and acute suprapubic pain accompanied by urinary retention.Ultrasound demonstrated a large intravesical clot in both patients.The patient with prostate cancer had a clot volume of 120 cm3, and the patient with bladder cancer had a clot volume of 50 cm3.We decided to place a three-way catheter to carry out the continuous irrigation of the bladder as well as suction with a syringe in both patients.After not having success with the clot evacuation, patients were transferred to the operating room to realize cystoscopy with endoscopic evacuation of the bladder clots.A large and well-organized clot was observed in both patients, occupying almost the entire bladder.We decided first to carry out irrigation with 1.5 L of saline solution with 0.3%hydrogen peroxide.We decided to use an endotracheal 14 Fr suction catheter (Fig.1A)connected to the wall suction with a pressure of 200 mmHg through the cystoscope sheath (Fig.1B).We checked that there were no clots left on the bladder at the end of the procedure with a standard cystoscopy and verified the integrity of the bladder.We left a three-way Foley catheter with saline irrigation at the end of the procedure.We performed this method under the internal committee agreement and with written informed consents signed by both patients.Both patients were successfully managed by this combined technique.There were no complications during surgery or postoperative period.In 24 h, the urine was clear with the normal yellowish color,so we suspended the irrigation.Clot evacuation is a common situation faced by urologist.Sometimes a large and well-organized clot is difficult to break and evacuate by conventional methods.Given this situation, we decided to apply the theory proposed by Warlick et al.[2]; we irrigated the bladder with 1.5 L of 0.3% of hydrogen peroxide in normal saline.Hydrogen peroxide is medically used as an antiseptic solution for infections and wound irrigations [5].The role of hydrogen peroxide over the clot is not yet so wellunderstood; however, the inhibition of adenosine phosphate and oxidative effects of hydrogen peroxide are some of the theories proposed [6,7].In our experience, the way hydrogen peroxide may work is by contracting the clot as well as giving a more liquid consistency (Figs.2A and 2B).Another important effect that hydrogen peroxide cause is hemostasis due to the activation of the tissue factor,platelet aggregation regulating the contractility and function of the barrier of the endothelial cells and by stimulating the activation of the platelet-derived growth factor[6,8].Several articles demonstrated that there were no adverse effects with the use of hydrogen peroxide in the bladder [2,9,10].The concentration used in this study was the one proposed by Warlick et al.[2].There could be a big concern in what are the potential damages to the bladder mucosa; nevertheless, Xu et al.[9] mentioned that in cystoscopy performed 6 months posterior to the bladder irrigation with hydrogen peroxide no abnormalities were found.
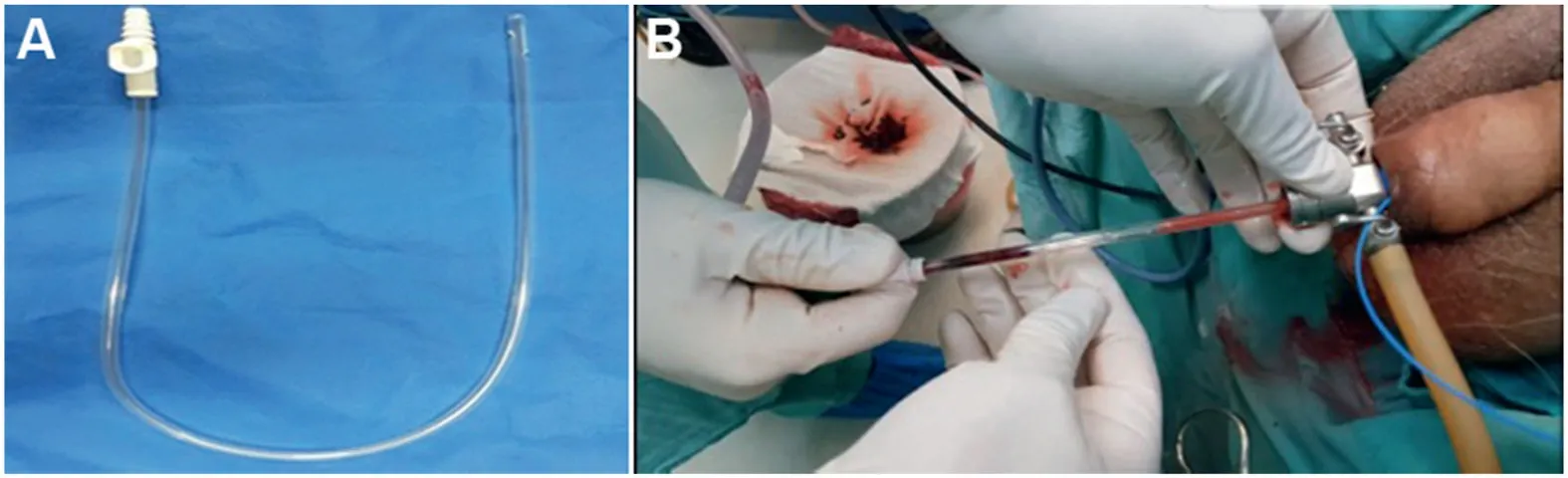
Figure 1 The placement of the three-way catheter and bladder flushing.(A) Endotracheal suction catheter with the suction vent; (B) Endotracheal suction catheter passing through the cystoscope sheath.
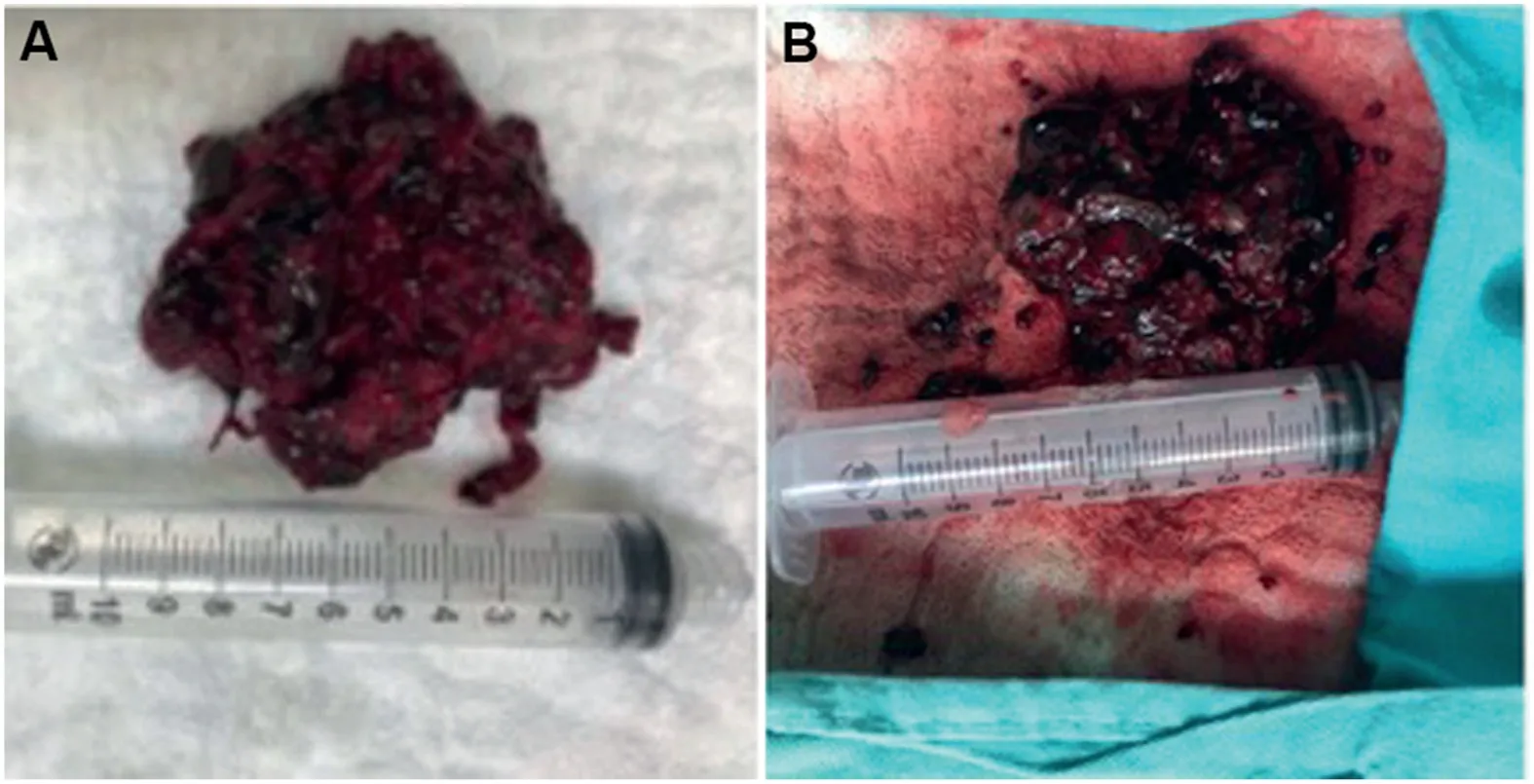
Figure 2 Treatment of clot with hydrogen peroxide.(A)Clot without hydrogen peroxide; (B) Clot after the application of hydrogen peroxide.
Goel and Dalela [3] applied suction to the bladder to evacuate the clots of 25 patients without having any complication with a suction bridge method.We believe this method is very efficient, however, not all hospitals have this equipment.Applying the knowledge used to make this bridge,we came up with the idea of using the endotracheal suction catheter used by anesthesiologists.This catheter has a French measure as the conventional Foley catheters;at the tip, it has openings so that the secretions could pass at the other side an air vent so that we can regulate suction.Another advantage is that this catheter has measures similar to Foley catheters and goes up to 18 Fr.Also, the endotracheal suction catheter has the same manageable consistency of a Foley catheter so we can reduce the bladder perforation risk.This study has certain limitations because there is no control group and it is a nonrandomized study.Also, this study is a single-center study including a small number of patients.
We were the first group that combined methods to manage a well-organized bladder clot.We believe that the suction method is very useful and combined with the oxidizing process of the hydrogen peroxide potentiates,even more,the suction method.Our novel and reproducible idea has the advantage that is a material commonly found in hospitals.A prospective study should be done to validate our combined method.
Author contributions
Study design: Fred Alain Montelongo-Rodrı´guez.
Data acquisition: Fred Alain Montelongo-Rodrı´guez, Mario Va´zquez-Herrera, Carlos Daniel Guerra-Castan˜o´n.
Data analysis: Fred Alain Montelongo-Rodrı´guez, Mario Va´zquez-Herrera, Carlos Daniel Guerra-Castan˜o´n.
Drafting of manuscript: Fred Alain Montelongo-Rodrı´guez.
Critical revision of the manuscript: Adria´n Gutie´rrez-Gonza´lez, Lauro Salvador Go´mez-Guerra.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2022年1期
Asian Journal of Urology2022年1期
- Asian Journal of Urology的其它文章
- Chromophobe renal cell carcinoma: Novel molecular insights and clinicopathologic updates
- The role of preoperative dutasteride in reducing bleeding during transurethral resection of the prostate: A systematic review and meta-analysis of randomized controlled trials
- Efficacy and safety of desmopressin on frequency and urgency in female patients with overactive bladder and nocturia,current clinical features and outcomes: A systematic review
- The impact of the coronavirus disease 2019 pandemic on elective urological procedures in Australia
- Efficacy of a combination of dutasteride,tadalafil,and solifenacin in the treatment of previously unsuccessful patients
- Associations between IL-1RN variable number of tandem repeat, IL-1β(-511)and IL-1β (+3954) gene polymorphisms and urolithiasis in Uighur children of China