
Subcostal artery bleeding after endoscopic combined intrarenal surgery: Signs and treatment
2022-03-25 06:40DvideCmpossoRoertoMenozziCrlMrtoAntonioFrttini
Asian Journal of Urology 2022年1期
Dvide Cmposso , Roerto Menozzi , Crl Mrto ,Antonio Frttini
a Urology Unit, Civil Hospital of Guastalla, Azienda USL-IRCCS di Reggio Emilia, Parma, Italy
b Interventional Neuroradiology Unit, University Hospital of Parma, Parma, Italy
c Department of Radiology, University Hospital of Parma, Parma, Italy
Percutaneous nephrolithotomy is the first option in renal stones >2 cm.One of the most serious complications of this procedure is postoperative bleeding [1].Various risk factors (multiple punctures, position, access size, stone volume, operative time, and non-papillary puncture)were considered in the literature with no clear conclusions [1-2].Despite the discordance about the risk factors, the etiology is clear.Bleeding can occur in the perioperative period, due to the injury of a renal segmental artery or vein or delayed due to the formation of arteriovenous fistula or pseudoaneurysm.All these injuries take place during the renal puncture and the track dilation.In most cases, the grade of bleeding after percutaneous nephrolithotomy is negligible and selflimiting, but in case of severe hemorrhage, angiography and super-selective angioembolization is the treatment of choice also for renal function preservation [3].Hypotension and hematuria are the most common presentations.We reported the case of a 55-year-old male, who underwent supine endoscopic combined intrarenal surgery for a right staghorn stone with X-ray guided lower pole papillary puncture access, below the 11th rib.The procedure was uneventful.A few hours after surgery, he developed loin throbbing pain and hypotension without hematuria.Abdomen ultrasound did not reveal kidney hematoma or hydronephrosis.Computed tomography (CT) scan showed an 8 cm retroperitoneal hematoma with active bleeding from the XI subcostal artery.The patient underwent blood transfusion and angioembolization of the XI subcostal artery.No further treatments were necessary.Subcostal vessels injury is a very rare event.One case was reported in the literature, with hematuria through the nephrostomy tube [4].As in the previously reported case,we did not find any clear causes, nor could we suggest any additional preventive measures.With hemorrhagic complications,an early diagnosis is important to avoid misdiagnosis and mistreatment.In our case, the absence of hematuria and subcapsular or perinephric hematoma, with the selfreported loin throbbing pain (secondary to the dissection of the retroperitoneal space) are signs of extra-renal bleeding.These features should be considered for timely diagnosis.CT scan and angioembolization of arterial bleeding are the correct managements (Figs.1 and 2).
Author contributions
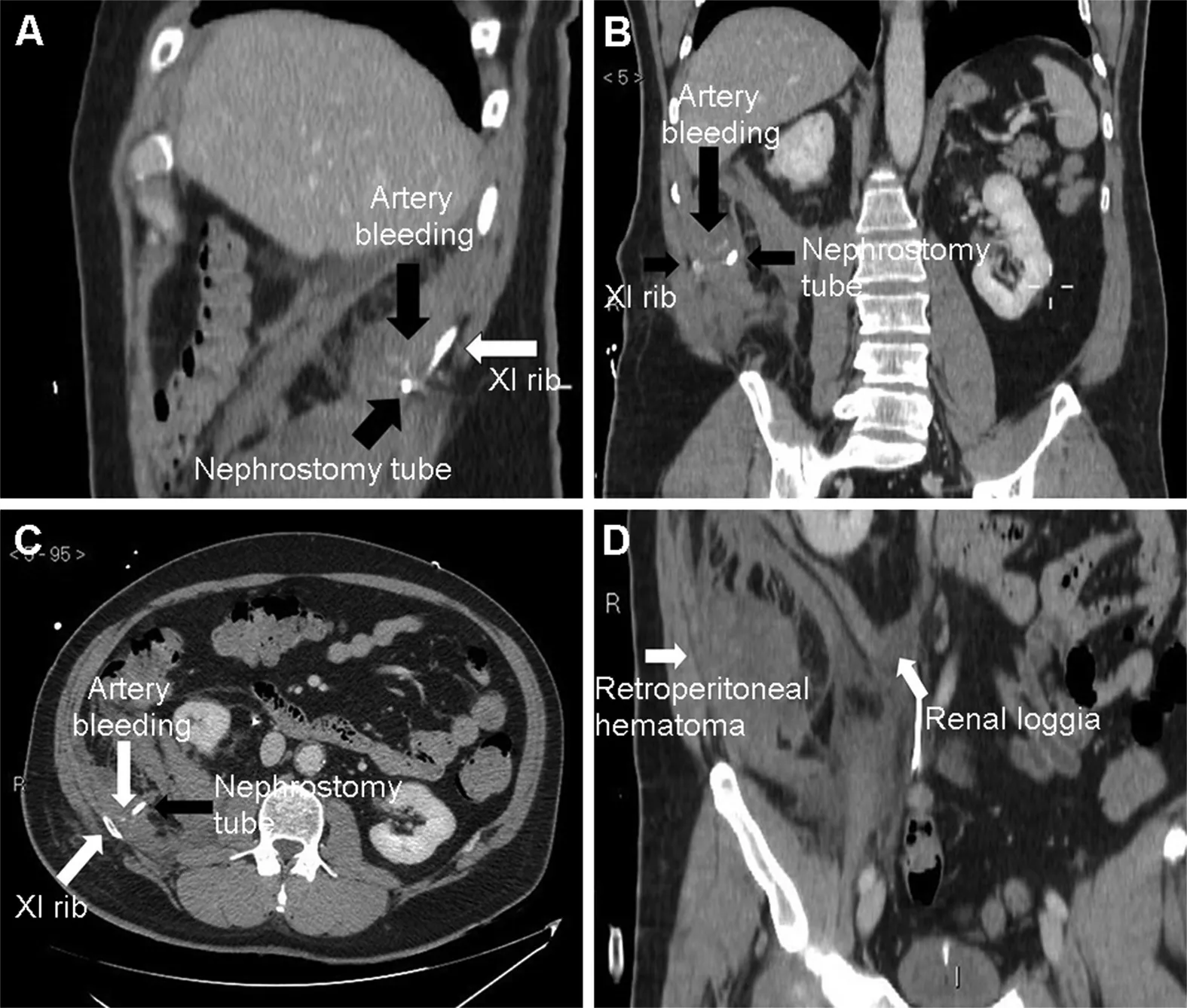
Figure 1 Computed tomography images.(A-C) Computed tomography scan revealed subcostal artery bleeding with a retroperitoneal hematoma;(D)The perirenal space was intact.

Figure 2 Angiographic exam.(A) Angiographic confirmation of subcostal artery bleeding; (B) Result after embolization using microcoils.
Drafting of manuscript: Davide Campobasso.
Critical revision of the manuscript: Roberto Menozzi,Antonio Frattin.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2022年1期
Asian Journal of Urology2022年1期
- Asian Journal of Urology的其它文章
- Chromophobe renal cell carcinoma: Novel molecular insights and clinicopathologic updates
- The role of preoperative dutasteride in reducing bleeding during transurethral resection of the prostate: A systematic review and meta-analysis of randomized controlled trials
- Efficacy and safety of desmopressin on frequency and urgency in female patients with overactive bladder and nocturia,current clinical features and outcomes: A systematic review
- The impact of the coronavirus disease 2019 pandemic on elective urological procedures in Australia
- Efficacy of a combination of dutasteride,tadalafil,and solifenacin in the treatment of previously unsuccessful patients
- Associations between IL-1RN variable number of tandem repeat, IL-1β(-511)and IL-1β (+3954) gene polymorphisms and urolithiasis in Uighur children of China