过敏性紫癜性肾炎临床预后影响因素研究
2022-03-08 14:28:49王小艳杨俊武张蓬杰
右江医学 2022年1期
王小艳 杨俊武 张蓬杰
【摘要】 目的 探討过敏性紫癜性肾炎临床预后影响因素。
方法 研究纳入陕西省人民医院2010年1月~2016年5月收治的过敏性紫癜性肾炎患者共138例,根据肾组织活检结果分组,其中无新月体组50例,节段性新月体组18例,大新月体组70例;比较不同病理类型的肾脏功能良好率,多因素Cox回归模型分析过敏性紫癜性肾炎临床预后独立危险因素。
结果 各组不同组间年龄、24 h尿蛋白量、Scr、eGFR、新月体类型、合并内皮增生比例及系膜增生比例比较差异有统计学意义(P<0.05);各组随访肾脏功能良好率比较差异有统计学意义,且大新月体组随访肾脏功能良好率显著低于其他两组(均P<0.01);多因素Cox回归模型分析结果显示,基线eGFR水平、合并大新月体比例可能是过敏性紫癜性肾炎临床预后的独立影响因素(P<0.05)。
结论 过敏性紫癜性肾炎各病理类型之间临床特征存在明显差异,其临床预后可能受患者基线eGFR水平、合并大新月体比例影响。
【关键词】 肾炎;预后;影响因素;新月体;eGFR;紫癜
中图分类号:R692 文献标志码:A DOI:10.3969/j.issn.1003-1383.2022.01.012
Study on influencing factors of clinical prognosis of Henoch-Schonlein purpura nephritis
WANG Xiaoyan1a, YANG Junwu1b, ZHANG Pengjie2
(1a. Department of Nephrology, 1b. Department of Hepatobiliary, 1.Pucheng County Hospital, Weinan 715500, Shaanxi, China; 2. Kidney Disease Center of Shaanxi Provincial People's Hospital, Xi'an 710068, Shaanxi, China)
【Abstract】 Objective To investigate the influencing factors of clinical prognosis of Henoch-Schonlein purpura nephritis.
Methods 138 patients with Henoch-Schonlein purpura nephritis admitted to Shaanxi Provincial People's Hospital from January 2010 to May 2016 were enrolled in this study. All patients were grouped according to the results of renal biopsy, there were 50 cases in non crescentic group, 18 cases in segmental crescentic group and 70 cases in large crescentic group. The good rate of renal function of different pathological types was compared, and multivariate Cox regression model was used to analyze the independent risk factors of clinical prognosis of Henoch-Schonlein purpura nephritis.
Results There were statistically significant differences in sex, 24-hour urine protein, Scr, eGFR, the proportion of complicated endothelial hyperplasia and the proportion of immunosuppressant among groups (P<0.05). There was statistically significant difference in the good rate of renal function among the three groups, and the good rate of renal function in the large crescentic group was significantly lower than those of the other two groups (all P<0.01). Multivariate Cox regression model analysis showed that the baseline eGFR level, the proportion of patients complicated with greater crescents and the proportion of patients with mixed crescents were independent prognostic factors of Henoch-Schonlein purpura nephritis (P<0.05).
Conclusion There are significant differences in clinical characteristics of the pathological types of Henoch-Schonlein purpura nephritis, and its clinical prognosis may be affected by the baseline eGFR level and the proportion of complicated large crescents.
【Key words】 nephritis; prognosis; influencing factors; crescent; eGFR; purpura
过敏性紫癜性肾炎患者肾小球新月体病变与临床症状严重程度有关,但其是否会影响肾脏功能良好率尚无明确定论[1~2]。目前IgA肾病肾脏病理分型标准已将新月体纳入其中,而IgA肾病与过敏性紫癜性肾炎在临床和病理特征方面较为接近,但新月体病变情况是否可用于过敏性紫癜性肾炎患者临床预后评估仍缺乏充足证据[3~5]。基于上述问题,本次研究通过纳入陕西省人民医院2010年1月~2016年5月收治的过敏性紫癜性肾炎患者共138例,根据肾组织活检结果分组,旨在探讨影响过敏性紫癜性肾炎临床预后的因素,现报道如下。
1 资料与方法
1.1 研究对象
本次研究纳入陕西省人民医院2010年1月~2016年5月收治的过敏性紫癜性肾炎患者共138例,根据肾组织活检结果分组,即无新月体组(50例)、节段性新月体组(18例)及大新月体组(70例)。纳入标准:①经肾活检病理诊断确诊[6];②有确切皮肤紫癜病史;③年龄≥14岁;④临床资料完整。排除标准:①肾活检肾小球数目<8个;②继发性肾小球肾炎;③肾穿刺禁忌证。研究方案设计符合《赫尔辛基宣言》要求,且患者或家属签署知情同意书。
1.2 方法
查阅病例收集患者性别、年龄、病史、临床症状、血压、24 h尿蛋白量、Scr及用药情况等资料;根据EPI-GFR公式计算eGFR。肾穿刺后获得组织标本送检病理,行光镜、免疫荧光及电镜检查[7]。
1.3 随访预后评估
随访截止时间为2020年6月;肾脏功能不良判定标准为随访2年内eGFR降低>基线值30%,或随访过程中Scr较基线值升高1倍,或进入终末期肾脏病,反之则为肾脏功能良好[8]。
1.4 统计学方法
选择SPSS 22.0软件处理数据;正态性评估采用Kolmogorov-Smirnov检验,其中符合正态分布计量资料以(±s)表示,多组间比较采用方差分析,两两比较采用t检验;不符合正态分布计量资料以[M(Q1,Q3)]表示,比较采用Mann-Whitney U检验;计数资料以%表示,比较采用χ2检验;肾脏功能良好率比较采用Kaplan-Meier法;多因素分析采用Cox回归模型分析;检验水准:α=0.05,双侧检验。
2 结 果
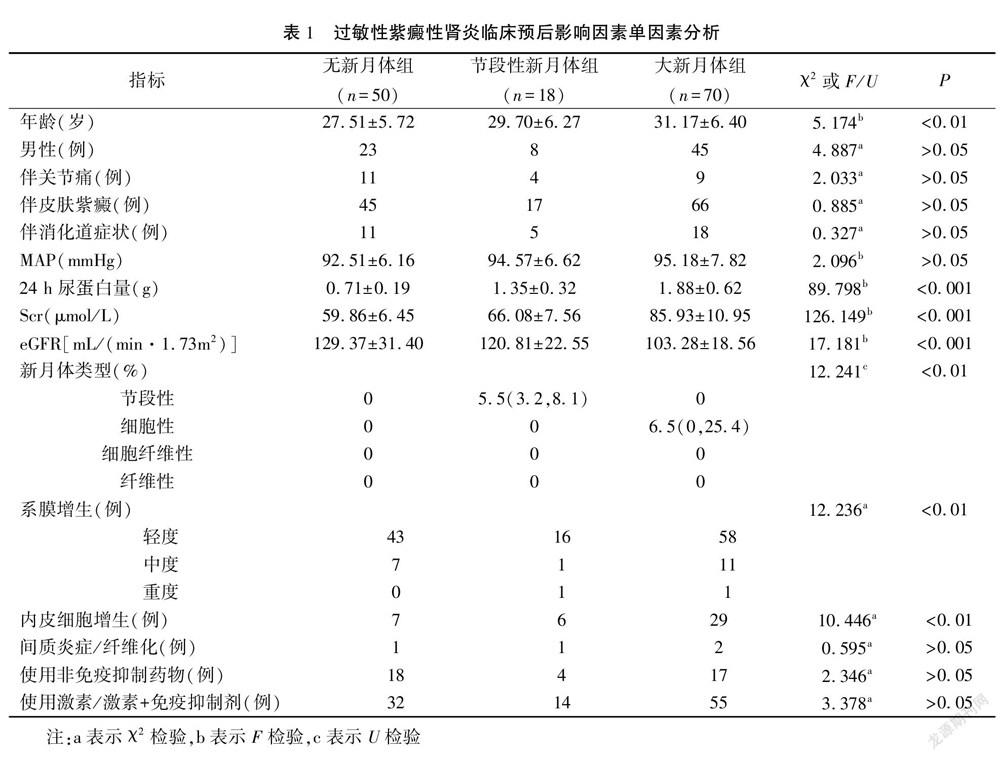
2.1 过敏性紫癜性肾炎临床预后影响因素单因素分析
不同组间年龄、24 h尿蛋白量、Scr、eGFR、新月体类型、合并内皮增生比例及系膜增生比例比较差异有统计学意义(P<0.05)。见表1。
2.2 不同组肾脏功能良好率比较
无新月体组、节段性新月体组及大新月体组随访累积肾脏功能良好率分别为96.00%、100.00%、78.62%,三组随访肾脏功能良好率比较差异有统计学意义(log-rank=20.68,P<0.01);大新月体组随访肾脏功能良好率显著低于无新月体组、节段性新月体组(P<0.01)。
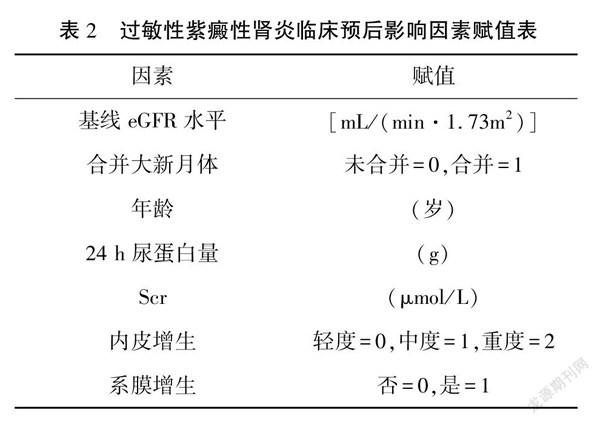
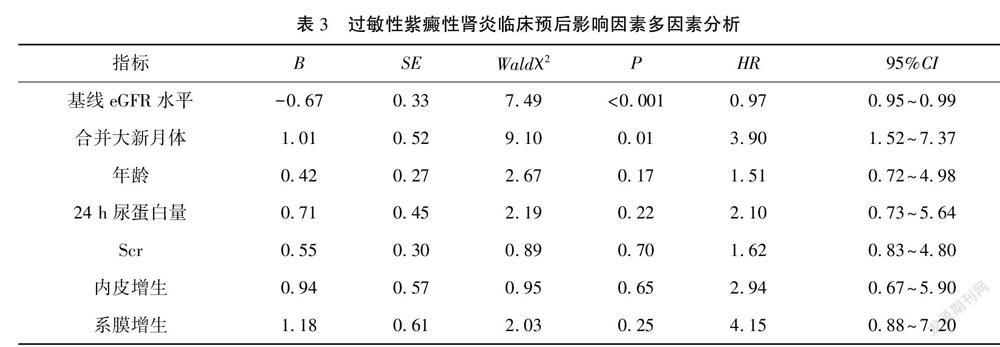
2.3 过敏性紫癜性肾炎临床预后影响因素多因素分析
纳入单因素分析有统计学意义指标进入Cox回归模型行多因素分析,结果显示基线eGFR水平、合并大新月体比例为过敏性紫癜性肾炎临床预后独立影响因素(P<0.05)。见表2、表3。
3 讨 论
目前与过敏性紫癜性肾炎病理特征相似的IgA肾病分型中已将新月体纳入[9~10]。已有研究显示[11~12],使用免疫抑制剂可影响新月体预测肾炎患者临床预后的价值。本次研究结果中,大新月体组患者使用免疫抑制剂比例显著高于其他两组,Kaplan-Meier法生存分析结果证实,无新月体组、节段性新月体组及大新月体组随访肾脏功能良好率分别为96.00%、100.00%、78.62%,三组随访肾脏功能良好率比较差异有统计学意义,大新月体组随访肾脏功能良好率低于无新月体组、节段性新月体组,即伴大新月体患者肾脏功能良好率更低,预后更差。Cox回归模型多因素分析结果显示,合并大新月體比例是过敏性紫癜性肾炎临床预后独立影响因素,进一步证实大新月体形成比例可独立影响过敏性紫癜性肾炎患者临床预后,合并大新月体比例越高则肾脏功能良好率越低,对于伴高比例大新月体形成患者临床应给予更为积极有效的治疗。此外基线eGFR水平是过敏性紫癜性肾炎临床预后独立影响因素,与既往研究结果相符[13~14]。
国外研究分析发现新月体形成可影响系统性红斑狼疮肾炎患者预后,结果证实单纯节段性新月体组患者具有最高抗双链DNA抗体阳性率和免疫荧光阳性程度,其中以C1q沉积最为明显,证实此类患者病情呈明显急性活动趋势[13,15~16]。另有报道提示伴节段性新月体IgA肾病患者往往存在急性病变,临床医师应更加重视[17~20]。本次研究结果中,节段性新月体组与无新月体组患者临床特征、肾脏功能良好率比较差异均无统计学意义;需要注意本次研究中节段性新月体组患者无不良预后事件发生,导致难以纳入风险模型进一步评估,需扩大样本量和延长随访时间明确临床意义。
本次研究亦存在一定不足:①属于单中心回顾性研究,纳入患者时间跨度相对较大,同时发生终点事件例数相对较少,所得结论存在偏倚可能;②本中心过敏性紫癜性肾炎患者免疫抑制剂使用比例较高,同时因纳入样本量较少,无法对免疫抑制剂用量和维持治疗方案进行亚组分析,所得结论仍有待后续研究进一步确证。
综上所述,过敏性紫癜性肾炎临床预后与患者基线eGFR水平、合并大新月体比例密切相关。
参 考 文 献
[1] LAU K K,SUZUKI H,NOVAK J,et al.Pathogenesis of Henoch-Schnlein Purpura nephritis[J].Pediatr Nephrol,2010,25(1):19-26.
[2] KIM C H,LIM B J,BAE Y S,et al.Using the Oxford classification of IgA nephropathy to predict long-term outcomes of Henoch-Schnlein Purpura nephritis in adults[J].Mod Pathol,2014,27(7):972-982.
[3] KOSKELA M,YLINEN E,UKONMAANAHO E M,et al.The ISKDC classification and a new semiquantitative classification for predicting outcomes of Henoch-Schnlein Purpura nephritis[J].Pediatr Nephrol,2017,32(7):1201-1209.
[4] 美國改善全球肾脏病预后组织.KDIGO慢性肾脏病评价及管理临床实践指南:2012版[M].王海燕,译.北京:人民卫生出版社,2014:125-126.
[5] SHRESTHA S,SUMINGAN N,TAN J,et al.Henoch-Schnlein Purpura with nephritis in adults:adverse prognostic indicators in a UK population[J].QJM,2006,99(4):253-265.
[6] PLUMB L A, ONI L, MARKS S D,et al.Paediatric anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis: an update on renal management[J].Pediatr Nephrol,2018,33(1):25-39.
[7] GEETHA D,SETHI S,DE VRIESE A S,et al.Interstitial immunostaining and renal outcomes in antineutrophil cytoplasmic antibody-associated glomerulonephritis[J].Am J Nephrol,2017,46(3):231-238.
[8] TOMINAGA K,UCHIDA T,IMAKIIRE T,et al.Anti-neutrophil cytoplasmic antibody-associated glomerulonephritis with detection of myeloperoxidase and phospholipase A2 receptor in membranous nephropathy-lesions:report of two patients with microscopic polyangiitis[J].BMC Nephrol,2018,19(1):120.
[9] LI C,ZHOU M L,LIANG D D,et al.Treatment and clinicopathological characteristics of lupus nephritis with anti-neutrophil cytoplasmic antibody positivity:a case-control study[J].BMJ Open,2017,7(7):e015668.
[10] CAI F,HAN F,WANG H,et al.The crescentic implication of renal outcomes in proliferative lupus nephritis[J].J Rheumatol,2018,45(4):513-520.
[11] BRIX S R,NORIEGA M,HERDEN E M,et al.Organisation of lymphocytic infiltrates in ANCA-associated glomerulonephritis[J].Histopathology,2018,72(7):1093-1101.
[12] TRIMARCHI H,BARRATT J,CATTRAN D C,et al.Oxford classification of IgA nephropathy 2016:an update from the IgA nephropathy classification working group[J].Kidney Int,2017,91(5):1014-1021.
[13] GUO N H,FU X,ZI F M,et al.The potential therapeutic benefit of resveratrol on Th17/Treg imbalance in immune thrombocytopenic Purpura[J].Int Immunopharmacol,2019,73:181-192.
[14] ZHANG A,NING B,SUN N,et al.Indirubin increases CD4+CD25+Foxp3+regulatory T cells to prevent immune thrombocytopenia in mice[J].PLoS One,2015,10(11):e0142634.
[15] LI J Q,TIAN J M,FAN X R,et al.miR-106b-5p induces immune imbalance of Treg/Th17 in immune thrombocytopenic Purpura through NR4A3/Foxp3 pathway[J].Cell Cycle,2020,19(11):1265-1274.
[16] CHEN L,WANG X,YIN L,et al.Effects of dexamethasone and gamma globulin combined with prednisone on the therapeutic effect and immune function of Henoch-Schonlein Purpura nephritis in children[J].J Clin Lab Anal,2021,35(1):e23580.
[17] WU D,LIU Y,PANG N,et al.PD-1/PD-L1 pathway activation restores the imbalance of Th1/Th2 and treg/Th17 cells subtypes in immune thrombocytopenic Purpura patients[J].Medicine:Baltimore,2019,98(43):e17608.
[18] KATAOKA H,YASUDA S,FUKAYA S,et al.Decreased expression of Runx1 and lowered proportion of Foxp3+CD25+CD4+ regulatory T cells in systemic sclerosis[J].Mod Rheumatol,2015,25(1):90-95.
[19] IMAI T,NISHIYAMA K,UEKI K,et al.Involvement of activated cytotoxic T lymphocytes and natural killer cells in Henoch-Schnlein Purpura nephritis[J].Clin Transl Immunology,2020,9(11):e1212.
[20] LIAO W,LI M,WU H,et al.Down-regulation of MBD4 contributes to hypomethylation and overexpression of CD70 in CD4+ T cells in systemic lupus erythematosus[J].Clin Epigenetics,2017,9:104.
(收稿日期:2020-12-17 修回日期:2021-10-26)
(編辑:潘明志)
猜你喜欢
家庭医学(下半月)(2020年4期)2020-05-30 12:42:42
中外医疗(2016年15期)2016-12-01 04:25:52
中国乳业(2016年4期)2016-11-07 09:50:20
中国市场(2016年35期)2016-10-19 02:30:10
商(2016年27期)2016-10-17 07:09:07
商(2016年27期)2016-10-17 04:40:12
科技视界(2016年20期)2016-09-29 13:45:52
中国民族医药杂志(2016年4期)2016-05-09 07:41:00
中国卫生标准管理(2015年17期)2016-01-20 09:26:46
中国继续医学教育(2015年3期)2016-01-06 01:36:33