
Expert consensus on the application of the magnetic anchoring and traction technique in thoracoscopic and laparoscopic surgery
2022-03-02 06:51JiGngBiYueWngYongZhngYiLvSientifiCommitteeoftheThirInterntionlConfereneofMgnetiSurgery
Ji-Gng Bi , , , Yue Wng , , , Yong Zhng ,, Yi Lv , , ,, Sientifi Committee of the Thir Interntionl Conferene of Mgneti Surgery
a Department of Hepatobiliary Surgery, Institute of Advanced Surgical Technology and Engineering, The First Affiliated Hospital of Xi’an Jiaotong University,Xi’an 710061, China
b National Local Joint Engineering Research Center for Precision Surgery & Regenerative Medicine, The First Affiliated Hospital of Xi’an Jiaotong University,Xi’an 710061, China
c Shaanxi Provincial Center for Regenerative Medicine and Surgical Engineering, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an 710061, China
d Department of Thoracic Surgery, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an 710061, China
Introduction
The mutual interference between surgical instruments in thoracoscopic and laparoscopic surgery and the effective exposure of the surgical field are important factors affecting surgical operability [1] . Magnetic anchoring and traction is one of the core techniques of magnetic surgery, which uses magnetic materials to generate force through indirect contact to achieve traction exposure of the target organs [2] ( Fig. 1 ). The magnetic anchoring and traction system comprises an internal and an external magnetic component. The external magnetic component is usually a permanent magnet, and the internal magnetic component includes an internal magnet and a tissue clip. This system requires fewer trocars, reduces surgical trauma, and improves surgical operability [3] . At present, the magnetic anchoring and traction technique has been applied in many fields including general surgery [ 3-10 ],gynecology [ 10 , 11 ], urology [ 12-14 ], and thoracic surgery [15] . We formed the following consensus on the indications, contraindications, surgical skills, notes, and complication management for the clinical application of the magnetic anchoring and traction technique.
Indications and contraindications
Indications
Currently, thoracic and laparoscopic surgery requires traction to ensure that the exposure of the surgical field is suitable for the application of the magnetic anchoring and traction technique, such as in laparoscopic cholecystectomy [ 3 , 5-8 ], appendectomy [ 9 , 11 ], ovarian cystectomy [11] , hysterectomy [10] , nephrectomy and prostatectomy [ 12-14 ], thoracoscopic lobectomy [15] ,and esophagectomy. Suitable diseases include: (A) benign cholecystitis, gallbladder polyps and other benign gallbladder lesions; (B)appendicitis; (C) benign gynecological diseases, including ovarian cysts, fibroids and ectopic pregnancy; (D) renal tumors, prostate cancer; (E) benign and malignant pulmonary nodules; (F) early and middle stage esophageal cancer, including squamous cell carcinoma, adenocarcinoma, etc.
Contraindications
(1) Serious dysfunctions of vital organs such as the heart, lung,kidney and brain, leading to the patients unable to tolerate the surgery, in which existing methods of thoracic and laparoscopic surgery are also contraindicated [3] .
(2) Excessive obesity and thickness of the chest and abdominal wall result in the magnetic anchoring force being unable to achieve effective traction [ 3 , 7 ]. However, the specific upper limit of body mass index (BMI) is uncertain. The maximum of BMI in the literature was 67.7 kg/m2[16] .
(3) Patients with magnetic implant in the body [3] . This would be a relative contraindication. For example, for patients with pacemaker, we are able to perform abdominal procedures (such as prostatectomy) because there is a sufficient distance to assure that the magnet would not impact on the pacemaker, so this is not a contraindication for abdominal surgery. But for thorascopic surgery, this may be a contraindication.
Application routine
Preoperative evaluation and preparation
(1) According to the factors such as the thickness of the thoraco-abdominal wall and the traction force required to pull the target organ, surgeons need to evaluate the range of magnetic force required for effective anchoring and pulling, and select the appropriate external and internal magnetic components [ 17 , 18 ].
(2) Preoperative instrument sterilization. In order to prevent corrosion of the magnetic instruments and weakening of the magnetic force, the method of strong corrosion and high temperature should not be used for the sterilization of magnetic instruments; rather, ethylene oxide or hydrogen peroxide plasma is recommended [ 19 , 20 ].
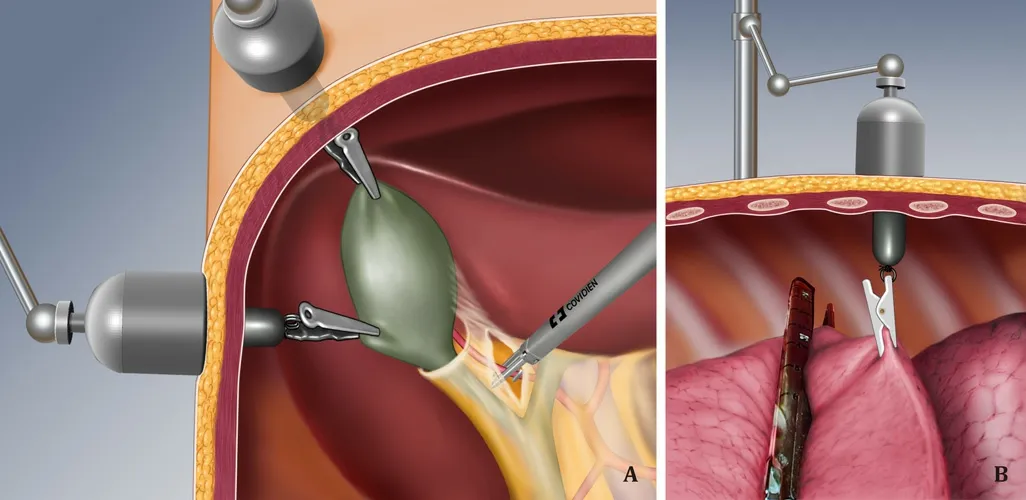
Fig. 1. Schematic diagram of magnetic anchoring and traction technique (This is an adaptation of the original idea of Dr. Guillermo Dominguez, the author of the Imanlap project [ 4 , 5 ]). A : Magnetic anchoring gallbladder traction; B : magnetic anchoring lung lobe traction.
Surgical steps
(1) Inserting the internal magnetic component into the thoracic or abdominal cavity: the titanium alloy non-magnetic holder is used to insert the internal magnetic component into the thoracic or abdominal cavity through the trocar [21] .
3.2.1 教师梳理教学目标,综合设计引用案例 选取恰当的案例,从课堂开始引入主题,引导学生从对案例产生兴趣转移到对教学内容产生兴趣,同步设计递进问题引导学生思考,全面发挥案例的导引与主线作用,实现教学目标。
(2) Clamping the tissue: the titanium alloy non-magnetic clamp is used to open the tissue clamp and clamp the target organ [4] .
(3) Anchoring: the inner magnetic component is placed inside the thoracic or abdominal wall using a holder, and the outer magnetic component is moved to the corresponding position of the thoracic or abdominal wall outside the body to achieve mutual attraction of the internal and external magnetic components [3] .
(4) Adjusting the exposure: the external magnetic component is moved, and by changing the position and direction of the built-in tissue clip, the target organ is pulled to expose the surgical field [3] . If using a single internal magnetic component for tissue exposure is not ideal, multiple components are used.
(5) Taking out the internal magnetic component: after the operation, the holder is used to remove the inner magnetic component through the stamp [22] .
Application notes
(1) Internal magnetic component: in order to avoid interference between magnetically anchored surgical instruments and other ferromagnetic surgical instruments, soft magnetic materials are used such as pure iron, permalloy (iron-nickel alloy), iron-cobalt alloy,and silicon steel to shield internal magnet, so that the magnetic leakage of magnetic anchoring instruments can be reduced [22] ,or a soft internal magnet can be used.
(2) Non-magnetic surgical instruments: instruments made from diamagnetic materials, such as titanium alloys, are preferable [ 23 , 24 ].
(3) Maintain the stable coupling of the internal and external magnetic components: try to avoid frequent separation [25] .
(4) When the magnetic anchoring cannot achieve effective traction, the surgical plan should be immediately adjusted [4] .
Complication managements
(2) Tissue laceration: target organ tissue laceration can occur when the traction force is too strong [14] . Choose tough tissue to clamp; the clamped tissue should not be too small.
(3) Tissue crush injury: when multiple internal magnetic components are used simultaneously, the internal magnetic components may attract and collide with each other, resulting in crushed tissues [11] . Soft magnetic materials are recommended for the inner magnetic component; even if it detaches, there will be no tissue clamped between the components. There is also the possibility of tissue clipping between the internal magnetic component and ferromagnetic surgical instruments, and damaged tissue should be repaired.
Summary and outlook
The technique of magnetic anchoring and traction is a minimally invasive technique and needs further improvement. The application of this technique not only reduces surgical trauma because fewer trocars are required, but also alleviates the interference between surgical instruments, and improves the exposure of the surgical field and the surgical operability. At present, the magnetic anchoring traction technique has been successfully applied in many thoracoscopic and laparoscopic procedures. With continuously deepening understanding of the magnetic anchoring traction technique and improvement of the magnetic anchoring traction device, this technique will be used more widely.
Members of Scientific Committee of the Third International Conference of Magnetic Surgery (Sorted alphabetically by last name)
Luca Bertolaccini , IEO European Institute of Oncology IRCCS, Milan, Italy; Luigi Bonavina, University of Milan, Istituto di Ricovero e Cura a Carattere Scientifico Policlin San Donato,Italy; Jeffrey Cadeddu, University of Texas Southwestern Medical Center, United States; Paolo Dario, The Biorobotics Institute,Sant’Anna School of Advanced Studies, Italy; Michele Diana , Institut de chirurgie guidée par l’image (IHU) de Strasbourg, Strasbourg,France; Guillermo Dominguez , Fundacio‘n Hospitalaria, Buenos Aires, Argentina; Tim H Fass, University College Cork, Ireland;Bing Hu, West China Hospital, Sichuan University, China; Matthew Kroh , Digestive Disease Institute at Cleveland Clinic Abu Dhabi,USA; Jian-Hui Li, Shaanxi Provincial People’s Hospital, China; Arianna Menciassi , Scuola Superiore Sant’Anna, Italy; Padraig Cantillon Murphy, University College Cork, Ireland; Bradley J Nelson , Institute of Robotics and Intelligent Systems, ETH Zurich,Switzerland; Homero Rivas, Mohammed Bin Rashid University of Medicine and Health Sciences in Dubai, UAE; Ryan L Steinberg ,University of Texas Southwestern Medical Center, USA; Pietro Valdastri, University of Leeds, UK; Rong-Qian Wu, The First Affiliated Hospital of Xi’an Jiaotong University, China; Xiao-Peng Yan, The First Affiliated Hospital of Xi’an Jiaotong University, China ; Vitalii Zablotskii, Institute of Physics of the Academy of Sciences of the Czech Republic, Czech.
Acknowledgments
None.
CRediT authorship contribution statement
Ji-Gang Bai : Data curation, Formal analysis, Writing - original draft. Yue Wang : Methodology, Writing - original draft. Yong Zhang : Conceptualization, Writing - review & editing. Yi Lv : Conceptualization, Supervision, Writing - review & editing.
Funding
None.
Ethical approval
Not needed.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
猜你喜欢
小学教学研究(2022年21期)2022-07-28
当代党员(2022年9期)2022-05-20
家庭影院技术(2021年3期)2021-05-21
家庭影院技术(2021年1期)2021-03-19
家庭影院技术(2021年1期)2021-03-19
当代陕西(2019年15期)2019-09-02
中国计算机报(2017年44期)2017-12-11
广西教育·B版(2016年8期)2016-11-01
中学生数理化·高二版(2016年4期)2016-05-14
新高考·高二数学(2014年7期)2014-09-18
 Hepatobiliary & Pancreatic Diseases International2022年1期
Hepatobiliary & Pancreatic Diseases International2022年1期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Primary pancreatic lymphoma diagnosed by endoscopic ultrasound-guided fine needle biopsy
- A stable and reliable animal model for hepatocellular carcinoma with portal vein tumor thrombus
- Diverse and precision therapies open new horizons for patients with advanced pancreatic ductal adenocarcinoma
- SNHG16 promotes hepatocellular carcinoma development via activating ECM receptor interaction pathway
- Predictors of recurrent bile duct stone after clearance by endoscopic retrograde cholangiopancreatography: A case-control study
- Call for action: Increased healthcare utilization with growing use of percutaneous cholecystectomy tube over initial cholecystectomy in cirrhotics