
Case Control Study Obesity is associated with decreased risk of microscopic colitis in women
2022-02-15 08:19RobertSandlerTemitopeKekuJohnWoosleyDaleSandlerJosephGalankoAnnePeery
Robert S Sandler,Temitope 0 Keku,John T Woosley,Dale P Sandler,Joseph A Galanko,Anne F Peery
Robert S Sandler,Department of Medicine,University of North Carolina,Chapel Hill,NC 27514-7555,United States.rsandler@med.unc.edu
Temitope O Keku,Joseph A Galanko,Anne F Peery,Department of Medicine,University of North Carolina,Chapel Hill,NC 27514-7555,United States
John T Woosley,Department of Pathology,University of North Carolina,Chapel Hill,NC 27514,United States
Dale P Sandler,Department of Health and Human Services,National Institute of Environmental Health Sciences,Durham,NC 27709,United States
Abstract BACKGROUND Microscopic colitis is a leading cause of diarrhea in the older adults.There is limited information about risk factors.We hypothesized that obesity would be associated with microscopic colitis.AIM To examine the association between obesity and microscopic colitis in men and women undergoing colonoscopy.METHODS We conducted a case-control study at the University of North Carolina Hospitals.We identified and enrolled men and women referred for elective,outpatient colonoscopy for chronic diarrhea.We excluded patients with a past diagnosis of Crohn’s disease or ulcerative colitis.A research pathologist reviewed biopsies on every patient and classified them as microscopic colitis cases or non-microscopic colitis controls.Patients provided information on body weight,height and exposure to medications via structured interviews or Internet based forms.The analysis included 110 patients with microscopic colitis (cases) and 252 nonmicroscopic colitis controls.Multivariable analyses were performed using logistic regression to estimate odds ratios and 95% confidence intervals.RESULTS Cases were older and more likely than controls to be white race.Study subjects were well educated,but cases were better educated than controls.Cases with microscopic colitis had lower body mass index than controls and reported more weight loss after the onset of diarrhea.Compared to patients who were normal or under-weight,obese (BMI > 30 kg/m2) patients were substantially less likely to have microscopic colitis after adjusting for age and education,adjusted OR (aOR)0.35,95% confidence interval (CI) 0.18-0.66).When stratified by sex,the association was limited to obese women,aOR 0.21,95%CI:0.10-0.45.Patients with microscopic colitis were more likely to report weight loss after the onset of diarrhea.After stratifying by weight loss,there remained a strong inverse association between obesity and microscopic colitis,aOR 0.33,95%CI:0.10 -1.11 among the patients who did not lose weight.Ever use of birth control pills was associated with lower risk of microscopic colitis after adjusting for age,education and BMI,aOR 0.38,95%CI:0.17-0.84.CONCLUSION Compared to controls also seen for diarrhea,microscopic colitis cases were less likely to be obese.Mechanisms are unknown but could involve hormonal effects of obesity or the gut microbiome.
Key Words:Colitis;Microscopic/epidemiology;Humans;Diarrhea/epidemiology;Obesity
lNTRODUCTlON
Microscopic colitis is a chronic inflammatory disease of the colon characterized by a normal or near normal endoscopic appearance but abnormal pathology.It is increasingly recognized that endoscopically visible lesions can be recognized in nearly 40% of patients although they are non-specific[1].Histologically,there is a thickened collagen band (collagenous colitis) or an increase in intraepithelial lymphocytes(lymphocytic colitis)[1].Microscopic colitis was first described in 1976 by Lindstrom[2].The term microscopic colitis was used by Readet al[3] in a 1980 publication describing a series of patients with chronic diarrhea of unknown origin.While initially considered uncommon,population-based studies have shown a rising incidence that may have started to plateau[4-6].
Microscopic colitis is now a frequent cause of chronic diarrhea,particularly in older adults.In some regions,the incidence of microscopic colitis exceeds Crohn’s disease and ulcerative colitis[7].Despite an increasing burden of disease,the etiology of microscopic colitis is not known.Prior studies implicated a range of medications including proton pump inhibitors (PPIs),nonsteroidal anti-inflammatory drugs(NSAIDs),statins,and beta blockers[8].Cigarette smoking has also been implicated[9,10].The condition has been reported to be more common in patients with a number of auto-immune diseases[11].
There is currently limited information that obesity might be inversely associated with microscopic colitis[12,13].We conducted a case-control study among a population of patients scheduled for colonoscopy due to chronic diarrhea in order to assess whether obesity and hormonal factors might be associated with microscopic colitis.
MATERlALS AND METHODS
Briefly,we identified male and female patients between April 1,2015 and December 22,2020 who were referred for outpatient colonoscopy for diarrhea.We excluded patients with a prior history of Crohn’s disease and ulcerative colitis.Potential participants were mailed information about the study in advance of their procedure.On the day of their exam,eligibility was verified by a research assistant who obtained informed consent for participation.To be eligible for the study,patients had to report a Bristol Stool Form type 5,6,or 7 (mushy,loose,watery) during the week prior to their colonoscopy regardless of the number of stools[14] .We recruited patients from each of the 3 endoscopy units at the University of North Carolina Chapel Hill.If the research assistant was not available for consent at the time of the procedure,the patient was later contacted to verify eligibility and obtain consent.We also queried the hospital pathology database every month and contacted patients with biopsy proven microscopic colitis who were not identified prior to their colonoscopy.This group included patients who were referred for colonoscopy for other reasons (generally screening) but reported diarrhea and had colon biopsies taken during the colonoscopy to assess for microscopic colitis.In sensitivity analyses,the patients identified retrospectively from pathology were excluded.
Patients with signs of gross inflammation on colonoscopy were excluded.Patients with subtle or isolated mucosal abnormalities were not excluded.Patients with nonlymphocytic colitis on biopsies were also excluded.A research pathologist (JTW) who was not aware of the clinical diagnosis reviewed the slides for all enrolled study subjects.Cases were patients with microscopic colitis on biopsy defined by increased number of intraepithelial lymphocytes.Additional features included increased lamina propria chronic inflammation,with minimal crypt distortion or active cryptitis.Collagenous colitis was defined by a thickened subepithelial collagen band.Slides were initially reviewed by a clinical pathologist.The slides were then re-read by the study pathologist.When there was a disagreement between the clinical pathologist and the research pathologist,the research pathologist re-read the slides.In addition,a 20% sample of slides were resubmitted to the research pathologist.After excluding indeterminate colitis,there was a 100% match between the initial and final reading by the research pathologist.Controls were patients with normal pathology.Patients with indeterminate microscopic colitis based on a sparse number of lymphocytes were excluded to avoid possible misclassification and because there were too few for separate analysis.
After the colonoscopy,all participants completed a 30 to 40-minute structured telephone interview or self-completed the same questionnaire using an internet-based form.The telephone interviewer verified eligibility,including the diarrhea criteria,for patients who were identified from pathology or who were missed in the endoscopy unit.Participants self-reported demographics,body weight,height,medical history including over-the-counter and prescription medications,reproductive history,bowel habits,and gastrointestinal symptoms.The reproductive history for women included questions about age at first menses,oral contraceptive use,gravidity,parity,and if postmenopausal,age at and type of menopause,and menopause hormone therapy use.All exogenous hormone questions included age at initiation,duration of use,and use in the last year,but not type of hormone or dose.BMI was calculated from selfreported weight in kilograms divided by height in meters squared (kg/m2).BMI was categorized using Centers for Disease Control criteria:BMI < 25 kg/m2(under-or healthy weight),BMI 25.0 < 30 kg/m2(overweight),BMI > 30 kg/m2(obese).
Data analysis was conducted using Stata 17.0 (Stata Corp.College Station,TX).The analysis was reviewed by a biostatistician (JAG).Variables were examined one-by-one in bivariate analyses using chi square tests for categorical variables and Student t-tests for continuous variables.Multivariable logistic regression models were used to calculate adjusted odds ratios and 95% confidence intervals adjusted for age,educational status and BMI.Smoking was not included in models because smoking was not independently associated with microscopic after adjusting for education.We have previously examined the association between medications thought to be associated with microscopic colitis (PPI,statins,SSRI,NSAIDs)[15].There was no association in our study so those drugs were not included in models.Multivariable logistic models also included terms for reproductive factors including age at first live birth,number of live births and age of menarche.The model terms were informed by review of the relevant literature and directed acyclic graphs (DAGs)[16].For analyses of menopause,the reference group was the most common age of natural menopause,age 45-54.Missing data were not imputed.
The study was approved by the University of North Carolina Office of Human Research Ethics.All patients gave informed consent.
RESULTS
Patients were enrolled in the study between April 1,2015 and December 22,2020.Among the 1008 patients who were referred for colonoscopy for diarrhea,176 cancelled their colonoscopy,161 were ineligible,99 were missed in the endoscopy unit and not subsequently recruited,and 196 refused.After excluding indeterminate colitis(n=14),there were 362 who serve as the basis of this report.There were 110 microscopic colitis cases (including 34 identified from pathology reports) and 252 controls.Interviews were completed by phone by 84% of subjects and Internet for the remainder.
Table 1 shows characteristics of the study population.The cases were older than controls:case mean age 63.2 (standard deviation (SD) 12.7,interquartile range 53-73)vscontrol mean age 54.5 (SD 11.8,interquartile range 45-64).Cases were more likely than controls to be white (96.2%vs85.7%).As a group,the study subjects were very well educated,but cases were more likely to have a college degree or have attended graduate school,66.0%vs44.3%.Cases were less likely to be current smokers,11.3%vs21.0%.There was a strong correlation between smoking and education,with better educated patients substantially less likely to smoke (not shown).There was no difference between cases and controls for marital status,race,or smoking after adjustment.
As Saenko explained, when using deep learning, engineers must choose "between how much human-imposed, top-down design you put into something to make it more interpretable versus how much performance you lose as a result of that."
Overall,mean BMI was lower in cases (BMI 25.7 kg/m2(SD 6.4)) than controls (BMI 29.5 kg/m2(SD 7.2)).As shown in Table 2,the risk for microscopic colitis was lower for BMI 25-30 kg/m2(OR 0.71,95%CI:0.40-1.25) and BMI > 30 kg/m2(OR 0.31,95%CI:0.17-0.55) compared to under-or healthy weight (BMI < 25 kg/m2) as the reference.Similar results were seen in analyses adjusted for age and education.To determine whether the results were comparable for men and women,we stratified by sex.The results for women were similar to the overall results with lower risk for obese women.The results for men were null,but the number of men was small making estimates unstable with wide confidence intervals around risk estimates.Patients with microscopic colitis were more likely to report weight loss following the onset of diarrhea than controls:65.3% casesvs42.5% controls,p < 0.001.Because current BMI could be misclassified due to weight loss following the onset of diarrhea,we stratified on weight loss.The results were similar in the weight loss and the no weight loss strata.We conducted analyses separately for lymphocytic colitis and collagenous colitis and the results were similar to the overall.
All of the patients in our study had diarrhea.We asked patients if they had ever been told by a physician that they had irritable bowel syndrome (IBS).Not surprisingly the cases were less likely to have a history of IBS,odds ratio 0.40,95%CI:0.20 -0.78).When we stratified by IBS,patients in the highest BMI category were less likely to have microscopic colitis in the non-IBS stratum,aOR 0.38 (95%CI:0.18-0.79)an estimate similar to the overall estimate in cases and controls.We compared the BMI in patients with IBS stratified by microscopic colitis status.In the microscopic colitis cases,the mean BMI was not different in the IBS group (24.6 kg/m2(SD 7.2)) and the non-IBS group (25.7 kg/m2(SD 6.4),P=0.55).Similarly,the mean BMI was not different among the controls with IBS (30.3 kg/m2(SD 6.6)) compared to non-IBS controls (29.1 kg/m2(SD 7.2),P=-0.27)).
Because the risk for microscopic colitis was lower in obese women than men(recognizing small numbers of men),we examined potential hormonal risk factors in women.Reproductive factors are shown in Table 3.The table shows crude odds ratios and odds ratios adjusted for age,education and BMI (model 1) and age,education,BMI,number of live births and age at menarche (model 2).Age at menarche,parity,number of live births and age at first live birth were not different in cases and controls.Use of oral contraceptive pills was inversely associated with microscopic colitis in crude (OR 0.41,95%CI:022-0.79),adjusted (aOR 0.38,95%CI:0.17-0.84),and multiplyadjusted analyses (aOR 0.20,95%CI:0.08-0.52).The results were the same when cases identified by pathology were excluded.The results were also similar for lymphocytic and collagenous colitis.

Table 1 Characteristics of the study population
Menopausal factors are shown in Table 4.The percent of women who were postmenopausal was higher in the cases in crude analyses,but that is because they were older.The difference was absent in the adjusted model.Cases were more likely to have ever-used menopausal hormone hormones in the crude analysis OR 2.79,95%CI:1.44-5.41).After adjusting for age,education and BMI the risk estimate was lower(aOR 1.63,95%CI:0.73-3.62).
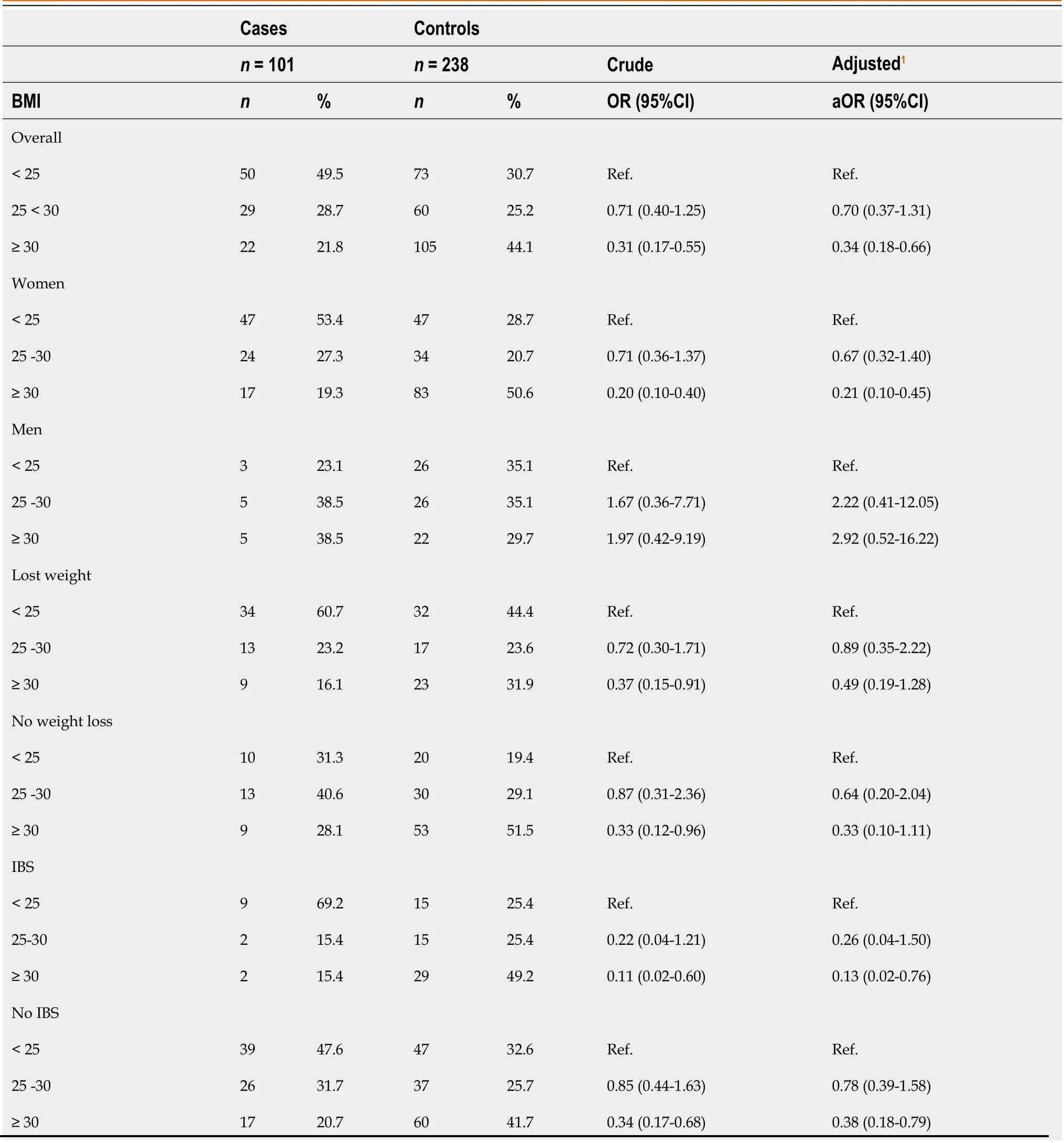
Table 2 Body mass index and risk of microscopic colitis
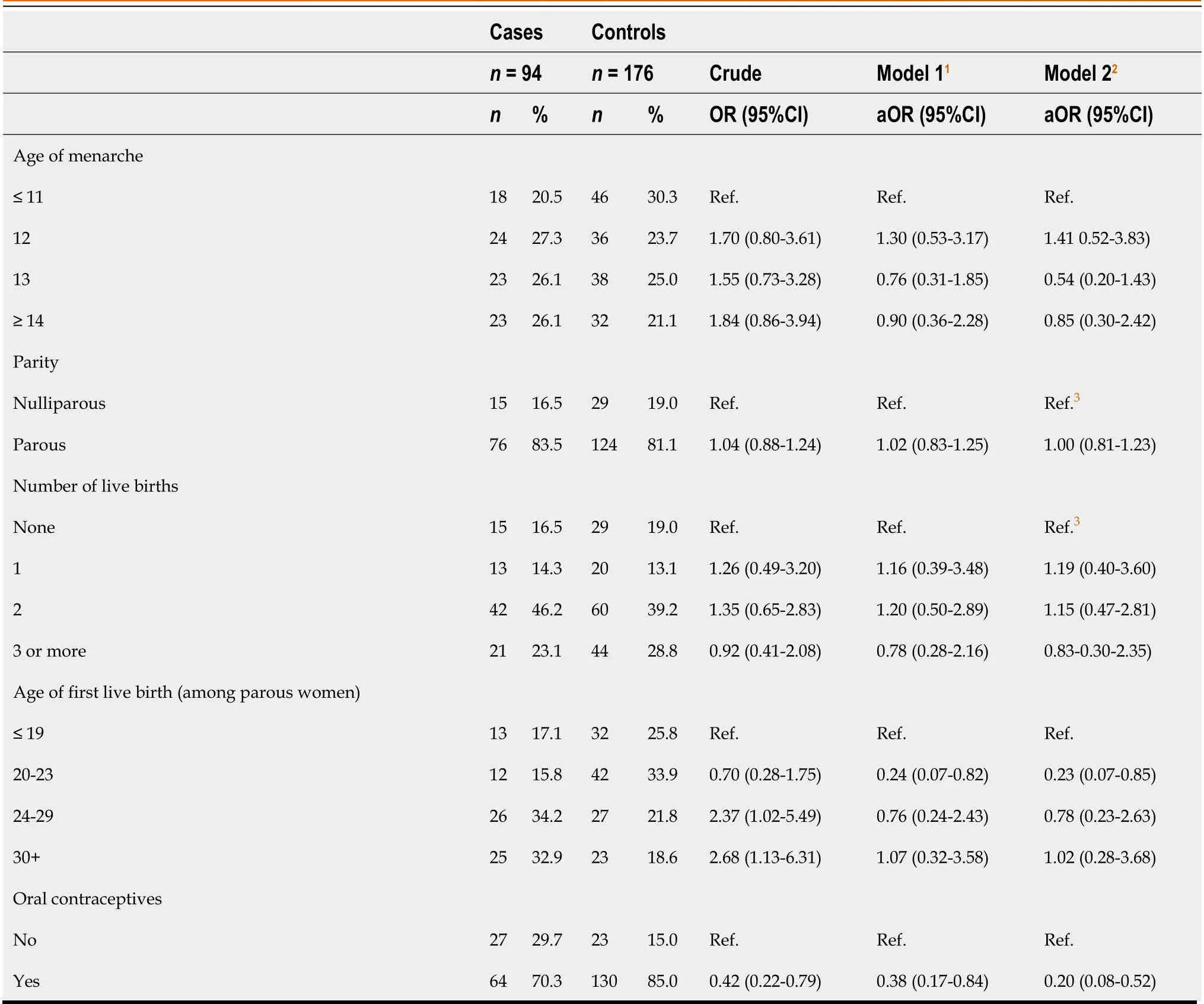
Table 3 Reproductive factors and risk of microscopic colitis in women

Table 4 Menopausal factors and risk of microscopic colitis in women
DlSCUSSlON
We found a striking difference in the risk for microscopic colitis with BMI,with a strong inverse association with obesity in women.Women with microscopic colitis were substantially less likely to be obese.There was no apparent effect of BMI on risk for microscopic colitis in men,although the number of men in our study was small.Given the sex differences,we also looked for possible reproductive or hormonal associations.We found a strong inverse association of microscopic colitis with ever use of oral contraceptives.In contrast to most prior studies,we enrolled patients who were referred for colonoscopy for diarrhea.At the time of the referral,the status as a microscopic colitis case or control was not known.All participants had similar symptoms,access to care,colonoscopy and biopsies.
Although BMI is an important risk factor for a number of diseases,there is surprisingly little information on the association between BMI and microscopic colitis.In a study using population controls,Larsenet al[17] reported data on 135 microscopic colitis who were compared to 27960 participants in the Malmo Diet and Cancer Study.There was no difference between the groups with respect to BMI.Similar to our study,Pascuaet al[18] included 259 diarrhea controls in a small study with 26 microscopic colitis patients.There was no difference in BMI.Another small study was designed to examine the microbiome in 20 patients with microscopic colitis,20 age-and sexmatched healthy controls,and 20 patients with functional diarrhea according to Rome IV criteria[19].The BMI was 24.7 (SD 3.5) in microscopic colitis patients,28.2 (SD 6.9)in healthy controls,and 27.9 (5.5) in the patients with chronic diarrhea.No statistics were reported in the paper,but based on the sample size and the estimates,the difference was significant for healthy controls (P=0.05) and for diarrhea controls (P=0.03).Rothet al[20] identified microscopic colitis cases from pathology records from 2002 -2010 from the Skåne University Hospital,Malmö,with controls selected from a population-based study of breast cancer.The BMI in cases was 24.84 kg/m2and controls 24.88 kg/m2,P=0.451.The cases and controls were not recruited contemporaneously.
Cotteret al[13] sought to develop a scoring system to predict microscopic colitis among patients presenting with diarrhea.In a derivation cohort of 617 patients,BMI <30 kg/m2was associated with an increased risk of microscopic colitis,OR 2.15 (95%CI:1.19-3.88).Weight loss has been shown to be associated with MC in publications by the same authors[21,22],and it is not clear whether weight loss might have led to misclassification of BMI category.Liuet al[12] used the two Nurses’ Health Study cohorts to identify 244 cases of self-reported microscopic colitis with 4.2 million person-years of observation.Compared to the women in the lowest BMI category,BMI < 18.5 kg/m2,those with a BMI > 30 had an adjusted hazard ratio of 0.50 (95%CI:0.32-0.79).The p for trend was < 0.001.Weight gain since early adulthood was also associated with reduced risk of microscopic colitis.The results were seen in both Nurses cohorts.
The controls in our study had diarrhea.If the diarrhea controls had a condition associated with obesity,that could potentially explain the findings.Many of the diarrhea patients who did not have microscopic colitis probably had irritable bowel syndrome.In a stratified analysis,the inverse association with obesity was particularly strong in the IBS strata (both cases and controls had a history of IBS).It is not clear that patients with IBS are more likely to be obese.A comprehensive review has not shown BMI differences in patients with irritable bowel syndrome[24].In our study the controls with IBS did not have a higher BMI than the controls without IBS.
The mechanism by which increased body weight might be inversely associated with microscopic colitis in our study and others is uncertain.Men are at substantially reduced risk of microscopic colitis than women[4].Perhaps the reduced risk is due to a protective effect of androgens.Obesity has been associated with increased levels of androgens[25,26].Obesity has been linked with change in the gut microbiome[27]which has,in turn,been linked with microscopic colitis[19,28,29].The gut microbiota can metabolize androgens and estrogens[30].
Despite the marked sex discrepancy in microscopic colitis,the literature on reproductive and hormonal factors is very limited.Burkeet alused data from the Nurses’ Health Study cohorts[31].Similar to our results,the authors found no association with age of menarche,parity,age of first live birth or age of menopause.They found an increased risk for postmenopausal hormones.Verhaeghet al[32]reported that hormonal factors were not associated with microscopic colitis in multivariable analysis,although number of cases might not have been large enough to detect small differences between populations.
We found that ever-use of oral contraceptive pills was associated with a reduced risk of microscopic colitis in crude and adjusted analyses.In contrast to our study,Burkeet al[31] reported that ever-use of oral contraceptives was associated with an increased risk of microscopic colitis based on data from the two Nurses’ Health Study cohorts.There was a large difference in oral contraceptive use in the two cohorts -45%in the Nurses’ Health Study (NHS) and 85% in Nurses’ Health Study II (NHSII).Oral contraceptive use was not queried after 1984 in NHS (almost 40 years ago),or after 2009 in NHSII.The elevated risk was only statistically significant in the earlier cohort.There has been a temporal change in the hormone concentration of oral contraceptive pills,and the different results between our study and the Nurses’ cohort study might be due to different times of enrollment.OCPs generally contain a mix of estrogen(usually estradiol) and a progestin.The estrogen dose has decreased from over 100 μg when first introduced in the 1960 to 20-30 μg or less now.Progestin-only contraceptives are also now available.These changes mean studies may not be comparable if they were performed at different times.
The mechanism behind the observed associations of menopausal hormones and oral contraceptives with microscopic colitis are unknown although there are some possibilities to consider.Estrogen and progesterone receptors are expressed in the gut,and sex steroids have been shown to influence colonic transit time,chloride secretion and intestinal permeability[33].Autoimmune diseases are more common in women than men,possibly due to hormonal factors[34].Hormonal contraceptives have effects on the immune system and have been linked with a number of different autoimmune diseases[35].Microscopic colitis has been regarded as an autoimmune disease,perhaps because of similarities to celiac disease[36].In a genome-wide association study using the UK Biobank,there was an association with single nucleotide polymorphisms on the MHC 8.1 haplotype,supporting an immune component to the pathogenesis of microscopic colitis[37].We did not find autoimmune disease was over-represented in our microscopic colitis cases (unpublished data).The gut microbiome is involved in the metabolism,excretion and circulation of sex hormones[30].The effect of menopausal hormones and oral contraceptives on microscopic colitis could be mediated by gut microbes.Gut microbes could metabolize sex steroids or exogenous steroids and alter the gut environment.
Our study had some important strengths.The patients were drawn from the same referral area and had similar access to and receipt of care.All of the patients had diarrhea.Other studies have used community[38],population[39],or disease controls[40].A single experienced gastrointestinal pathologist reviewed all of the slides to classify patients as microscopic colitis cases or normal controls.The study included men and women.Detailed information was obtained from study participants using structured interviews.
A limitation of the study was the small size,particularly for men.Microscopic colitis is an uncommon disease and most reports in the literature are hampered by small numbers.Many of the patients referred for colonoscopy were either not eligible,cancelled their appointments or refused to participate.Nonresponse,along with the selected nature of the study population,may affect generalizability but should not lead to bias.Exposures were determined by self-report which is common in case-control studies.Recall of past exposures may be inaccurate,but we would not expect the recall for cases and controls to be differential as all of the patients were enrolled in the study because of diarrhea..Cases were older than controls.We adjusted for age in all models and we performed sensitivity analyses with similar results.Lymphocytic colitis and collagenous colitis are considered to be histologic subtypes of the same disease[41] We combined the two entities to improve study power.In exploratory analyses we found similar results when we examine each type separately.The study was conducted in a developed country.Geographic variations in the incidence of microscopic colitis have been reported but there have been a limited number of direct comparative studies[1].There are few studies from developing countries[42].
Microscopic colitis,first described in 1976,is a relatively new disease.With any new disease there is the presumption that an environmental factor,as opposed to a genetic factor,is responsible.Obesity has increased in the US since the 1980[43].The incidence of microscopic colitis has also been increasing in the US [44].The fact that we and others have found lower risk of microscopic colitis with obesity suggests that obesity must interact with some other factor such as the microbiome to mediate risk.Given the difference in distribution in microscopic colitis by sex,exogenous hormones in the form of birth control pills and postmenopausal hormones are naturally of interest.In this study we found that postmenopausal hormones were modestly associated with a increased the risk of microscopic colitis and oral contraceptives with decreased risk.
As the population ages,the number of patients with microscopic colitis is likely to increase.Identifying factors associated with risk for microscopic colitis is an important first step developing hypotheses about etiology.
CONCLUSlON
Compared to controls also seen for diarrhea,microscopic colitis cases were less likely to be obese.Mechanisms are unknown but could involve hormonal effects of obesity or the gut microbiome.
ARTlCLE HlGHLlGHTS
Research background
There is limited information about risk factors for microscopic colitis,a leading cause of chronic waterv diarrhea.
Research motivation
We hypothesized that obesity might be associated with microscopic colitis.
Research objectives
To compare patients with microscopic colitis to patients with chronic diarrhea to learn more about associations with obesity and hormones.
Research methods
We conducted a case-control study among patients who were referred to a single academic medical center for chronic diarrhea.The biopsies were reviewed by a research pathologist and classified as microscopic colitis cases or diarrhea controls.We used logistic regression to estimate odds ratios and 95% confidence intervals.
Research results
Cases with microscopic colitis had a lower body mass index than controls in adjusted models.Although patients with microscopic colitis reported that they lost more weight following the onset of diarrhea,the associations with BMI persisted in analyses stratified by weight loss.Oral contraceptives were inversely associated with microscopic colitis.
Research conclusions
Microscopic colitis cases were less likely to be obese than diarrhea controls.While the mechanism behind the association is not known,it could involve hormonal effects of obesity or the gut microbiome.
Research perspectives
Additional research is needed to understand the association between obesity and microscopic colitis.
 World Journal of Gastroenterology2022年2期
World Journal of Gastroenterology2022年2期
- World Journal of Gastroenterology的其它文章
- Nanotheranostics:A powerful next-generation solution to tackle hepatocellular carcinoma
- Multiple subcellular localizations and functions of protein kinase Cδ in liver cancer
- Observational Study ldentification of functional tumor necrosis factor-alpha promoter variants associated with Helicobacter pylori infection in the Sudanese population:Computational approach
- Prospective Study Outreach onsite treatment with a simplified pangenotypic directacting anti-viral regimen for hepatitis C virus microelimination in a prison
- Therapeutic endoscopy for the treatment of post-bariatric surgery complications
- Update on the applications and limitations of alpha-fetoprotein for hepatocellular carcinoma