
A radiomics prognostic scoring system for predicting progression-free survival in patients with stage IV non-small cell lung cancer treated with platinum-based chemotherapy
2021-11-18 08:17:00LanHeZhenhuiLiXinChenYanqiHuangLixuYanChanghongLiangZaiyiLiu
Lan He ,Zhenhui Li ,Xin Chen ,Yanqi Huang ,Lixu Yan ,Changhong Liang ,Zaiyi Liu
1Department of Radiology,Guangdong Provincial People’s Hospital,Guangdong Academy of Medical Sciences,Guangzhou 510080,China;2Department of Radiology,the Third Affiliated Hospital of Kunming Medical University,Yunnan Cancer Hospital,Yunnan Cancer Center,Kunming 650118,China;3 Department of Radiology,Guangzhou First People’s Hospital,School of Medicine,South China University of Technology,Guangzhou 510120,China;4 The Second School of Clinical Medicine,Southern Medical University,Guangzhou 510515,China;5Department of Pathology,Guangdong Provincial People’s Hospital,Guangdong Academy of Medical Sciences,Guangzhou 510080,China
Abstract Objective:To develop and validate a radiomics prognostic scoring system (RPSS) for prediction of progressionfree survival (PFS) in patients with stage IV non-small cell lung cancer (NSCLC) treated with platinum-based chemotherapy.Methods:In this retrospective study,four independent cohorts of stage IV NSCLC patients treated with platinum-based chemotherapy were included for model construction and validation (Discovery:n=159;Internal validation:n=156;External validation:n=81,Mutation validation:n=64).First,a total of 1,182 three-dimensional radiomics features were extracted from pre-treatment computed tomography (CT) images of each patient.Then,a radiomics signature was constructed using the least absolute shrinkage and selection operator method (LASSO)penalized Cox regression analysis.Finally,an individualized prognostic scoring system incorporating radiomics signature and clinicopathologic risk factors was proposed for PFS prediction.Results:The established radiomics signature consisting of 16 features showed good discrimination for classifying patients with high-risk and low-risk progression to chemotherapy in all cohorts (All P<0.05).On the multivariable analysis,independent factors for PFS were radiomics signature,performance status (PS),and N stage,which were all selected into construction of RPSS.The RPSS showed significant prognostic performance for predicting PFS in discovery [C-index:0.772,95% confidence interval (95% CI):0.765-0.779],internal validation (C-index:0.738,95% CI:0.730-0.746),external validation (C-index:0.750,95% CI:0.734-0.765),and mutation validation (Cindex:0.739,95% CI:0.720-0.758).Decision curve analysis revealed that RPSS significantly outperformed the clinicopathologic-based model in terms of clinical usefulness (All P<0.05).Conclusions:This study established a radiomics prognostic scoring system as RPSS that can be conveniently used to achieve individualized prediction of PFS probability for stage IV NSCLC patients treated with platinumbased chemotherapy,which holds promise for guiding personalized pre-therapy of stage IV NSCLC.
Keywords:Non-small cell lung cancer;radiomics;prognostic scoring system;progression-free survival;platinum-based chemotherapy
Introduction
Lung cancer remains the most commonly diagnosed cancer,with high incidence and mortality rates in both males and females (1,2).Non-small cell lung cancer(NSCLC) accounts for 85% of all lung cancer cases.Nearly two-thirds of NSCLC patients have unresectable metastatic disease upon diagnosis (3).For patients without positive markers (e.g.,EGFR/ALK/ROS1),or patients with low programmed death ligand 1 (PD-L1) expression,first-line treatment of platinum-based chemotherapy is recommended for stage IV NSCLC according to the American Society of Clinical Oncology guideline (4,5).Even when a curative treatment approach is feasible,the survival outcomes among patients are various (6).Thus,a method for individually predicting the progression probability of patients can determine whether to continue,escalate,discontinue,or change a patient’s therapeutic schedule so as to improve therapeutic outcomes and potentially reduce therapeutic toxicity (7).However,how to assess the individual patient’s potential progression probability to platinum-based chemotherapy remains very challenging.
To date,clinical and genetic factors have been extensively investigated to select patients who may benefit from specific chemotherapies (8).It is increasingly suggested that tailored individual chemotherapy,based on molecular biomarkers,represents a novel avenue for NSCLC treatment (9).However,these methods are invasive and limited by the fact that they are acquired at a single timepoint and from a single anatomical location(10,11).To address this topic,radiomics is an emerging field that involves throughput conversion of quantitative automated imaging features into mineable data (12-14).With its capability of simultaneous modelling of both multiple image phenotypic features and clinical factor effects,radiomics analyses aim to provide comprehensive quantification of tumor phenotypes,which can be incorporated into prediction and prognostic models (15-19).With advances in radiomics,tumor characterization is not just limited to anatomy,but it also reveals cellular and genomic level information that is quantifiable as an imaging phenotype (14).However,this type of radiomics prognostic scoring system (RPSS) for predicting disease progression probability to platinum-based chemotherapy of stage IV NSCLC is currently lacking (20).
Hence,in this study we aimed to establish an effective RPSS to individually predict the progression probability to platinum-based chemotherapy for stage IV NSCLC patients with the aim of providing valuable information for personalized medicine.
Materials and methods
Patients
This retrospective study had ethical approval,and the informed consent requirement was waived.In this multicohort study,we reviewed 159 patients with stage IV NSCLC treated with first-line platinum-based chemotherapy at Guangdong Provincial People’s Hospital between November 2007 and March 2012 as the discovery cohort,and 156 patients treated from April 2012 to June 2016 in the same institution as the internal validation cohort.Another independent cohort of 81 patients was included from November 2007 to June 2016 in the Yunnan Cancer Hospital as the external validation cohort for this study (Figure 1).

Figure 1 Study design flowchart.GDPH,Guangdong Provincial People’s Hospital;YCH,Yunnan Cancer Hospital;RPSS,Radiomics prognostic scoring system.
All patients were treated according to the American Society of Clinical Oncology guideline (5).The inclusion criteria were as follows:1) Patients who were histological or cytological confirmed NSCLC;2) Patients diagnosed with stage IV according to the TNM classification system of the American Joint Committee on Cancer (21);3)Patients who were not harboring EGFR-sensitizing mutations orALKgene rearrangements;4) Patients with low PD-L1 expression;5) Patients underwent at least 4 cycles of platinum-based chemotherapy as first-line treatment;6) Patients received no radiotherapy and anticancer therapy before chemotherapy;and 7) Patients underwent a full follow-up.Patients with a history of other malignancies or surgery resection were excluded from this study.For each patient,the clinical variables that might correlate with the prognostic outcomes were also recorded,including age,gender,stage at diagnosis,smoking status,performance status (PS),histological type,and the administered therapeutic regimen.
Furthermore,with the aim of extending the prognostic value of RPSS we established for predicting progressionfree survival (PFS),we included in the analysis a mutation validation cohort of stage IV NSCLC patients with EGFRsensitizing mutation who only received platinum-based chemotherapy as first-line treatment from November 2007 to June 2016 in Guangdong Provincial People’s Hospital.
Treatment procedure
All patients only received cisplatin or carboplatin based double chemotherapy as first-line treatment (5).The other administrated regimens included pemetrexed,gemcitabine,paclitaxel,and docetaxel.The details of drug treatment are provided inSupplementary materials.During treatment,routine blood tests were conducted,and the liver and renal functions were monitored.
Follow-up and assessment of PFS
Each patient was followed at 4-week intervals with a CT of the chest/abdomen,physical examination,and routine laboratory tests.Additional CT or magnetic resonance imaging was routinely performed if extrapulmonary metastasis was suspected.PFS was defined as the time interval between the date of initiation of chemotherapy and either disease progression or death,which was censored at the date of death from other cause or the date of the last follow-up visit for the progression-free patients.
CT image acquisition,interpretation,and radiomics feature extraction
All patients performed contrast-enhanced CT scans within 2 weeks before chemotherapy start.The details of CT image acquisition are described inSupplementary materials.Then,all acquired CT images were gathered for tumor segmentation and radiomics feature extraction. The primary tumors from each patient were manually segmented by an experienced radiologist,with more than 10 years of clinical experience in chest CT interpretation.If multiple disconnected tumor volumes were found,the largest by volume was chosen for features extraction.
To ensure the reproducibility and accuracy,80 patients were randomly selected for a reproducibility analysis using the inter-and intra-class correlation coefficients (ICCs).The details of ICCs for the reproducibility analysis of radiomics features extraction are described in theSupplementary materials.An ICC greater than 0.75 indicated a good agreement.
Finally,we programmed the radiomics analysis algorithms to automatically extract the radiomics features from manually segmented tumor region.All medical images were resampled to the same voxel of 1 mm3×1 mm3× 1 mm3by using cubic spline interpolation in our study.The voxel intensity within the region of interest was discretized to the same range of 64 intensity values.The details of the radiomics analysis algorithms are summarized inSupplementary materials.In total,1,182 quantitative radiomics features were extracted from each patient’s contrast-enhanced chest CT images,which included tumor intensity,texture features,wavelet features,and Gabor features.All features were compliant with the Image Biomarker Standardization Initiative (IBSI) (22).
Feature selection and radiomics signature construction
The radiomics features data were firstly normalized with zscore normalization (23),and were filtered based on their independence from other features,as determined by the Pearson’s correlation coefficient among the features (cutoff value of 0.9) (24).Then,the feature selection was done in the discovery cohort using the least absolute shrinkage and selection operator method (LASSO) penalized Cox proportional regression (25,26).Finally,the radiomics signature was built through the combination of selected features weighted by their respective coefficients.
All patients were stratified into high-risk and low-risk progression groups by the established signature,which was achieved by using time-dependent receiver operating characteristic (ROC) curves (27) based on Kaplan-Meier survival analyses and log-rank test (28).The significant difference in PFS was analyzed to investigate the clinical benefits across different progression subgroups by the Kaplan-Meier survival analysis and the Cox proportional hazards regression model.
Development and validation of RPSS
First,the established radiomics signature and potential clinicopathologic characteristics,including age,gender,smoking history,histological type,PS,T stage,N stage,the site and volume of metastases,and chemotherapy regimens,were involved in multivariable Cox regression analysis.Then,a final model selection was performed by the backward step-down selection process with Akaike information criterion (29). Subsequently,RPSS was calculated based on the result of multivariate analysis for individualized probability prediction of PFS. The performance of RPSS was measured by the concordance index (C-index),the integrated area under the ROC curve(iAUC),and the integrated Brier score (iBS) (30),and also was assessed by comparing the predicted versus observed survival probability using the calibration curve (31,32).In addition,the prognostic predictive power of the RPSS was further validated in the internal validation,external validation,and mutation validation cohort.
Clinical usefulness
To determine the clinical benefits of this radiomics signature,we established another clinicopathologic-based model with only clinicopathological characteristics.Then,comparisons between RPSS and clinicopathologic-based model were evaluated by C-index,iAUC,iBS,net reclassification improvement (NRI),and integrated discrimination improvement (IDI) (33,34).The larger Cindex which resulted in the positive value for NRI and IDI,the more accurate was the prognostic prediction for predicting PFS (35).For iAUC,the higher value indicated better performance;while for iBS,the lower value indicated better performance.Finally,a decision curve analysis was performed for determining the clinical usefulness of RPSS by quantifying the net benefits at different threshold probabilities (36-38).
Statistical analysis
The Kaplan-Meier method was used to calculate PFS,and the differences in PFS were compared using a log-rank test.The data were analyzed using R software (Version 3.2.3;R Foundation for Statistical Computing,Vienna,Austria),and the details of all R packages used in this study are described inSupplementary materials.The results are considered statistically significant at P<0.05 using a twotailed test.
Results
Characteristics of study population
The demographics and clinical characteristics of all patient cohorts are shown inTable 1.The median follow-up time was 5.73 [interquartile range (IQR):3.53-8.00] months in discovery cohort,5.47 (IQR:3.33-7.93) months in internal validation cohort,7.07 (IQR:4.03-12.02) months in external validation cohort,and 6.04 (IQR:3.49-8.83)months in mutation cohort,respectively.
Radiomics analysis profiling of PFS
Based on the reproducibility and the accuracy of radiomics features extraction,we found that the intra-and interobserver reproducibility of features extraction was satisfactory.The inter-observer ICCs calculated ranged from 0.751 to 0.957 based on Reader 1’s and Reader 2’s first extraction features,and the intra-observer ICCs calculated ranged from 0.763 to 0.911 based on Reader 1’stwice feature extractions.A total of 1,182 radiomics features were extracted from the pre-treatment CT images of each patient.After filtering by correlation analysis,100 radiomics features were used for the subsequent analysis(Supplementary Figure S1).Then,16 key features with nonzero coefficients in the LASSO Cox regression model were selected (Supplementary Figure S2). The radiomics signature was constructed based on the regression analysis with a corresponding value calculated for each patient(Supplementary materials).The cut-off value of radiomics signature was -0.734,which was generated by a timedependent ROC curve (Supplementary Figure S3),and used for dividing patients into high-risk and low-risk progression groups.The Kaplan-Meier curves clearly showed different prognostic strata in PFS between the high-risk and low-risk progression subgroups in all cohorts,with a high statistical significance (log-rank P<0.01 in all cases,Figure 2).Lower value of radiomics signature was associated with improved PFS in discovery (HR:5.829,95% CI:3.532-9.618),internal validation (HR:3.701,95%CI:2.262-6.054),external validation (HR:3.077,95% CI:1.617-5.857),and mutation validation cohort (HR:3.050,95% CI:1.390-6.693).The PFS and disease progression rate in the high-risk progression and low-risk progression group in all cohort are listed inTable 2.
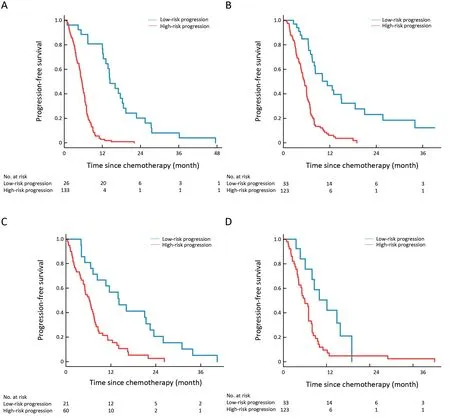
Figure 2 Kaplan-Meier survival curves for PFS in (A) discovery cohort (P<0.001,HR:5.829,95% CI:3.532-9.618);(B) internal validation cohort (P<0.001,HR:3.701,95% CI:2.262-6.054);(C) external validation cohort (P=0.001,HR:3.077,95% CI:1.617-5.857);and (D)mutation validation cohort (P=0.008,HR:3.050,95% CI:1.390-6.693) according to radiomics signature to classify stage IV NSCLC patients with high-risk and low-risk progression treated by platinum-based chemotherapy.PFS,progression-free survival;HR,hazard ratio;95% CI,95% confidence interval;NSCLC,non-small cell lung cancer.

Table 1 Demographic and pathological characteristics of all patient cohorts
RPSS for predicting of PFS
The multivariate analysis demonstrated that PS,N stage,and radiomics signature were independent risk factors for prediction of PFS (Table 3).RPSS was computed per patient according to the multivariate analyses,using a linear combination of selected independent risk factors weighted by their respective coefficients (Table 3).The C-index of RPSS for prediction of PFS were 0.772 (95% CI:0.765-0.779) in discovery,0.738 (95% CI:0.730-0.746) in internal validation,0.750 (95% CI:0.734-0.765) in external validation,and 0.739 (95% CI:0.720-0.758) in mutation validation.The iAUC was 0.760 in discovery,0.700 in internal validation,0.741 in external validation,and 0.705 in mutation validation cohort.AUC at 1-year PFS was 0.956 (95% CI:0.914-0.998) in discovery,0.825(95% CI:0.725-0.925) in internal validation,0.819 (95%CI:0.715-0.923) in external validation,and 0.818 (95% CI:0.649-0.986) in mutation validation cohort.And the iBS was 0.038 in discovery,0.072 in internal validation,0.070 in external validation,and 0.054 in mutation validation cohort.The calibration plot for the probability of survivalat the 10-month or 1-year PFS showed an optimal agreement between the prediction by RPSS and the actual observation (P<0.05,Figure 3).

Table 2 PFS and disease progression rate in high-risk progression and low-risk progression group

Table 3 Multivariate Cox regression analysis of models in discovery cohort
Comparison of predictive accuracy for PFS between RPSS and clinicopathologic-based model
As shown inTable 3,hazard ratios of the radiomics signature in the RPSS for survival were higher than that for other factors (PS and N stage).By removing signature from RPSS,a clinicopathologic-based model,with only the clinicopathologic characteristics (PS and N stage),was constructed.The predictive power for prognosis of PFS between RPSS and clinicopathologic-based model was compared.The C-index values for PFS prediction by clinicopathologic-based model were 0.686 (95% CI:0.678-0.694) in discovery,0.649 (95% CI:0.639-0.659) in internal validation,0.519 (95% CI:0.502-0.536) in external validation,and 0.674 (95% CI:0.655-0.693) in mutation validation cohort,respectively,which were significantly lower than the C-index by RPSS (All P<0.01).The iAUC was 0.616 in discovery,0.638 in internal validation,0.544 in external validation,and 0.659 in mutation validation cohort,which were significantly lower than the iAUC by RPSS.And the iBS was 0.055 in discovery,0.084 in internal validation,0.101 in external validation,and 0.056 in mutation validation cohort,which were significantly higher than the iBS by RPSS (of note:for iAUC and C-index,the higher the better,while for iBS,the lower the better) (Figure 4,5).Consequently,these results suggested that the RPSS was a more accurate and useful tool for the prediction of PFS regarding NRI of 0.732(95% CI:0.497-0.834) in discovery,0.480 (95% CI:0.203-0.676) in internal validation,0.463 (95% CI:0.131-0.674) in external validation,and 0.287 (95% CI:0.232-0.759) in mutation validation cohort (All P<0.05),and IDI of 0.335 (95% CI:0.210-0.459) in discovery,0.113(95% CI:0.036-0.184) in internal validation,0.263 (95%CI:0.076-0.397) in external validation,and 0.119 (95% CI:0.002-0.248) in mutation validation cohort (All P<0.05).
Clinical usefulness of RPSS
RPSS displayed as a nomogram is shown inFigure 6A,which used as an easy-to-use tool for probability scoring of 10-month and 1-year PFS.The decision curve analysis for RPSS provided a range of risk thresholds that yielded a positive net benefit compared with the clinicopathologicbased model,which is shown inFigure 6B.The RPSS provided the largest overall net benefit for predicting PFS compared with the clinicopathologic-based model.
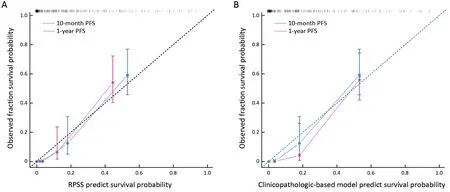
Figure 3 Calibration curves of RPSS and clinicopathologic-based model in terms of agreement between predicted and observed 1-year PFS and 10-month PFS.Calibration curve for RPSS (A) and clinicopathologic-based model (B) to predict survival probability.RPSS,radiomics prognostic scoring system;PFS,progression-free survival.

Figure 4 Prognostic value of RPSS and clinicopathologic-based model in terms of iAUC.(A) Discovery cohort;(B) internal validation cohort;(C) external validation cohort;and (D) mutation validation cohort.The higher value of iAUC indicated the better prognostic performance of clinical model.RPSS,radiomics prognostic scoring system;iAUC,integrated area under the curve.
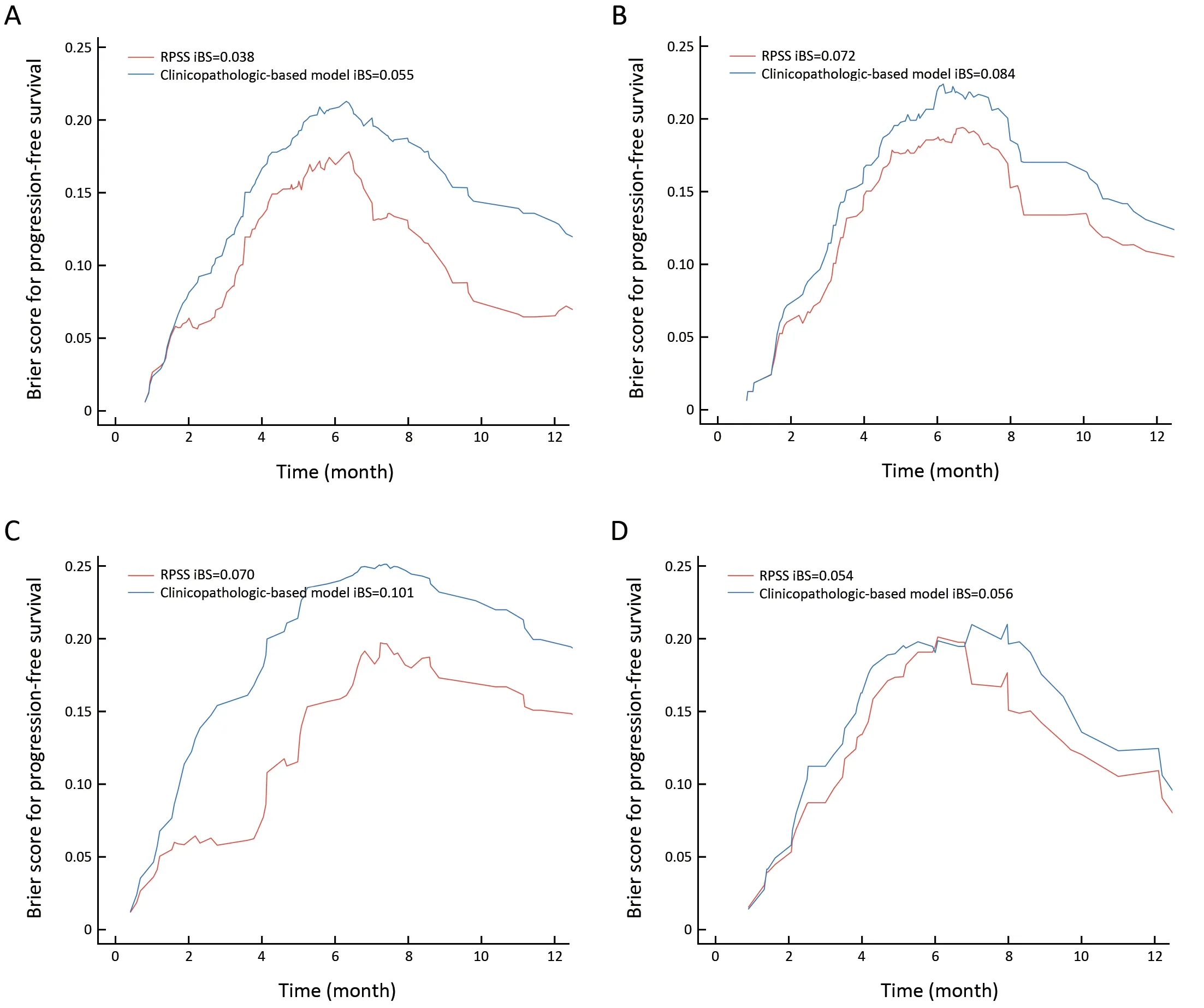
Figure 5 Prognostic value of RPSS and clinicopathologic-based model in terms of iBS.(A) Discovery cohort;(B) internal validation cohort;(C) external validation cohort;and (D) mutation validation cohort.The lower value of iBS indicated the better prognostic performance of clinical model.RPSS,radiomics prognostic scoring system;iBS,integrated Brier score.

Figure 6 Clinical usefulness of RPSS.(A) Proposed nomogram to estimate the risk of disease progression for stage IV NSCLC treated with platinum-based chemotherapy.An individual patient’s value is located on each variable axis,and a line is drawn upward to determine the number of points received for each variable value.The sum of these numbers is located on the Total Points axis,and a line is drawn downward to the survival axes to determine the likelihood of 10-month and 1-year PFS;(B) Decision curve analysis for comparison of the proposed RPSS (red line) and the clinicopathologic-based model (blue line) in terms of clinical usefulness.The y-axis measures the net benefit.The net benefit was calculated by subtracting the proportion of all patients who are false positive from the proportion who are true positive,and weighting by the relative harm of forgoing treatment compared with the negative consequences of an unnecessary treatment.Accordingly,the proposed RPSS had the higher net benefit compared with the clinicopathologic-based model for prediction of PFS in stage IV NSCLC patients treated with platinum-based chemotherapy.RPSS,radiomics prognostic scoring system;NSCLC,non-small cell lung cancer.
Discussion
Although target therapy and immunotherapy have been recently developed to treat lung cancer,platinum-based chemotherapy is still first-line treatment for most stage IV NSCLC patients without gene mutations or for those with low PD-L1 expression (4,5).Disease progression is the common reason to stop first-line cytotoxic chemotherapy according to the American Society of Clinical Oncology guideline (4).First-line cytotoxic chemotherapy should be stopped at disease progression or after four cycles in patients whose disease is stable but not responding to treatment.Because NSCLC is remarkably heterogeneous,with regard to survival of the individual patients (6),the rarity of the biomarkers as a clinical entity means that any attempts to create predictive models to give an indication of prognosis are extremely challenging.In the present study,we developed a noninvasive approach as RPSS to solve this problem.This scoring system aimed to estimate the probability of PFS based on a multivariate Cox proportional hazards model that included a radiomics signature and two clinical variables (PS and N stage).Based on three independent validation cohorts,RPSS was validated as a reliable tool to predict disease progression in these patients,and was superior to the clinicopathologicbased model,with only clinicopathological characteristics(PS and N stage).Furthermore,deriving of decision curve analysis and displaying as a nomogram for RPSS enhanced its practical utility.
A large number of studies have tried to identify genetic variations or clinical factors that can be used to individually predict the outcomes of platinum-based chemotherapy (7).However,due to their inherent limitations,which are achieved invasively or inconsistently,it is impractical to noninvasively conduct the prediction with univariate genetic or clinical factors.We thus extracted 1,182 image features from the pre-therapy CT images,and then reduced these to 16 potential predictors for integration into a radiomics signature by using LASSO Cox regression.All radiomics features selected for construction of radiomics signature were compliant with Image Biomarker Standardization Initiative (IBSI) (22).Our study showed that the established radiomics signature,which can potentially capture biologic properties like intra-and intertumor heterogeneities (39),can successfully stratify patients into high-risk and low-risk progression and demonstrate that approximately 70%-80% of the patients were predicted as high-risk progression of chemotherapy.Our results showed that higher value of radiomics signature was associated with higher risk of disease progression for stage IV NSCLC patients treated with platinum-based chemotherapy (All P<0.05).Through the multivariate analysis,we identified that PS and N stage were independent prognostic factors.These findings were in high concordance with previous studies for stage IV NSCLC patients treated with platinum-based chemotherapy (7,40).Additionally,we found that there were significant differences in T stage between the discovery cohort and validation cohorts.The possible reasons for the inconsistency might be that the eligible patients were enrolled from different periods,which is a stronger approach for the validation of RPSS (32).Therefore,consistent with a previous study on the prediction of EGFR-TKI treatment outcome in stage IV NSCLC (15),T stage was not suitable to be included as an independent factor into the final model in this study.
Even though overall survival (OS) is as the gold standard endpoint in clinical trials of chemotherapy for lung cancer,some of the disadvantages of this endpoint are the need for long-term follow-up and larger number of patients.Serial studies had found a high level of evidence that PFS can be considered a surrogate endpoint for OS in advanced NSCLC treated with chemotherapy (41).Disease progression also is the common reason to stop first-line cytotoxic chemotherapy according to the American Society of Clinical Oncology guideline (4,5).Thus,we kept PFS as the primary endpoint for this study.Furthermore,we have validated this radiomics signature we established for OS prediction on discovery and internal validation cohorts.The results showed that radiomics signature also successfully achieved patient stratification with respect to OS on discovery and internal validation cohorts,and remained as an independent predictor adjusted for clinicopathological parameters (All P<0.05,Supplementary materials).
Here,we also investigate whether the prognostic value of RPSS for predicting PFS could be extended in the mutation validation cohort of stage IV NSCLC patients with gene mutation who only received platinum-based chemotherapy as the first-line treatment.Surprisingly,we found that the RPSS also displayed a good discrimination in predicting PFS in mutation validation cohort (Cindex=0.739;iAUC=0.705;and AUC at 1-year PFS=0.818).This came to the robustness and effectiveness of our proposed RPSS for prognostic prediction.Thus,our established RPSS showed a good accuracy for prediction of PFS in all stage IV NSCLC patients treated with platinumbased chemotherapy.
To further investigate that how much extra clinical benefits we can obtain for individualized prediction on PFS by incorporating the radiomics signature,we also developed and compared a clinicopathologic-based model incorporated clinicopathologic characteristics (PS and N stage) without signature.Finally,results showed that RPSS showed better discrimination performance than the clinicopathologic-based model in all cohorts (C-index,RPSSvs.clinicopathologic-based model,discovery cohort:0.772vs.0.686;internal validation cohort:0.738vs.0.649;external validation cohort:0.750vs.0.519;mutation validation cohort:0.739vs.0.674;all comparisons P<0.05).And the decision curve analysis proved that RPSS offered significant improvement for individualized PFS prediction comparing with clinicopathologic-based model.
Although the RPSS we established demonstrated good levels of accuracy for the prediction of PFS,there are some limitations to our study.That is,the prognostic factors we used were restricted to the pre-therapy CT image phenotypic features and common clinical variables,and some potential molecular or immune biomarkers,such as excision repair complementing group 1 (ERCC1) protein(42),were not included as variables in the model analysis.The refinement of RPSS,with the identification of additional clinical,pathological or molecular predictors,will permit the optimization of this model.However,results of immunohistochemically staining are often inconsistent,assays for many biological or molecular markers are not widely available,and it may be difficult to standardize such results across the clinical practice.
Another limitation was that the primary tumors’ features were extracted in our study.For IV carcinoma,the metastases might be more important than primary tumor to predict the chemotherapy response.However,stage IV NSCLC patients might have more than one tumor including the metastases,which might affect the uniformity of extracted radiomics features.Most of radiomics studies built radiomics models based on primary tumor to predict the development of distant metastases from NSCLC (43).Lack of radiomics studies had shown the reproducibility of extracted radiomics features from the metastases tumor.Thus,we selected the primary tumors of each eligible patient for features extraction.If multiple disconnected tumor volumes were found,the largest by volume was chosen for features extraction.Further investigations are warranted to explore the potential usefulness of radiomics features extracted from metastases tumor for the prediction of chemotherapy response in patients with stage IV NSCLC.To the best of our knowledge,our study provided the first prognostic scoring system integrating both pretherapy image biomarkers and clinical factors for stage IV NSCLC patients treated with platinum-based chemotherapy.
Conclusions
We developed and externally validated a RPSS that was conveniently used to achieve an individualized prediction of PFS probability for stage IV NSCLC patients treated with platinum-based chemotherapy,which holds the promise of guiding the personalized pre-therapy of stage IV NSCLC.
Acknowledgements
This study was supported by the National Key Research and Development Plan of China (No.2017YFC1309100);the National Science Fund for Distinguished Young Scholars (No.81925023);and the National Natural Scientific Foundation of China (No.81771912,81901910,82072090,and 82001986).
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2021年5期
Chinese Journal of Cancer Research2021年5期
- Chinese Journal of Cancer Research的其它文章
- Lung cancer risk in never-smokers:An overview of environmental and genetic factors
- Chidamide combined with cyclophosphamide,doxorubicin,vincristine and prednisone in previously untreated patients with peripheral T-cell lymphoma
- Better prognostic determination of cT3 rectal cancer through measurement of distance to mesorectal fascia:A multicenter study
- Single patient classifier as a prognostic biomarker in pT1N1 gastric cancer:Results from two large Korean cohorts
- Coexisting opportunities and challenges:In which scenarios can minimal/measurable residual disease play a role in advancednon-small cell lung cancer?
- Integrating pathomics with radiomics and genomics for cancer prognosis:A brief review