
Health Council of the Netherlands and evaluation of the fifth generation, 5G, for wireless communication and cancer risks
2021-08-02 05:42LennartHardell
Lennart Hardell
Lennart Hardell, The Environment and Cancer Research Foundation, Studievägen 35, Örebro SE-702 17, Sweden
Lennart Hardell, Department of Faculty of Medicine and Health, Örebro University, Örebro SE-701 82, Sweden (retired)
Abstract Currently the fifth generation, 5G, for wireless communication is about to be rolled out worldwide. Many persons are concerned about potential health risks from radiofrequency radiation. In September 2017, a letter was sent to the European Union asking for a moratorium on the deployment until scientific evaluation has been made on potential health risks (http://www.5Gappeal.eu).This appeal has had little success. The Health Council of the Netherlands released on September 2, 2020 their evaluation on 5G and health. It was largely based on a World Health Organization draft and report by the Swedish Radiation Safety Authority, both criticized for not being impartial. The guidelines by the International Commission on Non-Ionizing Radiation Protection were recommended to be used, although they have been considered to be insufficient to protect against health hazards (http://www.emfscientist.org). The Health Council Committee recommended not to use the 26 GHz frequency band until health risks have been studied. For lower frequencies, the International Commission on Non-Ionizing Radiation Protection guidelines were recommended. The conclusion that there is no reason to stop the use of lower frequencies for 5G is not justified by current evidence on cancer risks as commented in this article. A moratorium is urgently needed on the implementation of 5G for wireless communication.
Key Words: 5G; Cancer risk; Health Council Netherlands
INTRODUCTION
The fifth generation, 5G, for wireless communication is about to be rolled out worldwide in spite of health concerns. This has created debate among concerned people in many countries. In an appeal to the European Union (EU) in September 2017,currently endorsed by more than 400 scientists and medical doctors, a moratorium on the 5G deployment was required until proper scientific evaluation of negative consequences has been made (http://www.5Gappeal.eu). This has not had any impact on the progress of the deployment of 5G.
On September 2, 2020, the Health Council of the Netherlands released their evaluation of 5G and health (No. 2020/16/16e/16Ae). The Committee consists of 9 members, 2 scientific secretaries, 1 incidentally consulting expert, and 3 observers.(https://www.healthcouncil.nl/documents/advisory-reports/2020/09/02/5g-andhealth).
Of large concern as to impartiality is that one member of the Committee, Huss A, is a member of the International Commission on Non-Ionizing Radiation Protection(ICNIRP) since May 2020. ICNIRP is a private organization based in Germany that does not acknowledge health effects other than caused by heating from radiofrequency(RF) radiation. Thereby nonthermal biological effects are disregarded.
Furthermore, one of the two secretaries, van Rongen E, has been a long-time commission member of ICNIRP since 2010, chair 2016 to 2020, and vice chair since May 2020 (https://www.researchgate.net/profile/Eric_Rongen). A third former ICNIRP member, Sienkiewicz Z, participated as a consulting expert.
It should be added that Huss A receives research funding from a telecom industry sponsored Swiss Foundation, and she is also member of this foundation’s Scientific Committee (https://www.emf.ethz.ch/en/foundation/organisation). Further, van Rongen E is a long-time member of the industry organizations, the Institute of Electrical and Electronics Engineers and the International Committee on Electromagnetic Safety (IEEE/ICES).
These facts give concern of conflicts of interest in the Health Council Committee.Members of ICNIRP tend to adhere also in other settings to the ICNIRP no-risk paradigm regarding nonthermal RF radiation. This may also be the case in the Health Council report. In fact it should be noted that the Ethical Board at the Karolinska Institute in Stockholm, Sweden concluded already in 2008 that being a member of ICNIRP may be a conflict of interest that should be stated officially whenever a member from ICNIRP makes opinions on health risks from electromagnetic fields(EMFs) on behalf of another organization, as in this case (Karolinska Institute Diary No. 3753-2008-609). This verdict is related to Prof. Ahlbom A, ICNIRP Commission Member from 1996 until 2008, and is a general statement. Those involved in the current Health Council report with ICNIRP affiliation (present or former) omitted to state that conflict of interest.
Recommendations by the Health Council of the Netherlands
The Committee has made four recommendations to the Parliament, cited in the following:(1) Because the lower frequency bands for 5G (up to 3.5 GHz) have already been used for telecommunication applications and Wi-Fi for years without resulting in any proven adverse health effects, the committee sees no reason to stop or restrict the use of these frequency bands. It does, however, recommend that the exposure should be monitored before, during and after the rollout of the 5G systems. This will make clear to what extent exposure to radiofrequency EMF changes as a result of the introduction of 5G, and any long-term health risks can then be estimated better. The World Health Organization (WHO) analysis can also be used in estimating the risks;(2) The committee recommends doing more research: epidemiological research into the relationship between exposure to the 5G frequencies used and the incidence of cancer, reduced male fertility, poor pregnancy outcomes and birth defects. An ongoing international study into the use of mobile telephones, in which the Netherlands is participating, can play a role in this: (a) experimental research into the health effects of exposure to EMFs in the 26 GHz frequency band; (b) scenario studies to get a picture of the exposure of individuals as a result of wireless communication systems (3G, 4G and 5G); (3) The committee recommends to not use the 26 GHz frequency band for 5G for as long as the potential health risks have not been investigated; and (4) Finally, the committee recommends using the latest guidelines from the ICNIRP as the basis for exposure policy in the Netherlands. Because it cannot be excluded that exposure under the latest ICNIRP standards also has the potential to affect health, the committee recommends taking a cautious approach and keep exposures as low as reasonably achievable.
Of these conclusions, number 3 is in agreement with an appeal to the EU asking for a moratorium on the roll-out of 5G until research has been done on potential health risks, although the appeal concerned all 5G frequencies (https://www.5gappeal.eu).The appeal has currently been signed by more than 400 international scientists and/or medical doctors.
The claim that “the lower frequency bands for 5G (up to 3.5 GHz) have already been used for telecommunications applications and Wi-Fi for years without resulting in any proven adverse health effects” is incorrect.
Evidence from research on cells, animals and humans shows that the frequencies used so far for telecommunications are harmful for humans and the environment. For overviews see[1-3].
There is no substantial research on health effects from the frequencies in the range between 3 and 4 GHz intended to be used for 5G as noted by the French authority ANSES in an expert report published in January 2020.
The Health Council Committee in Netherlands has mainly based its review on a 2014 draft report from the WHO and the reports from the Swedish Radiation Safety Authority (SSM). Huss A and van Rongen E have been coauthors of the Swedish SSM reports, and van Rongen E was furthermore a member of the WHO draft report’s core group of members, see Table 1.
The Committee recommends using the latest ICNIRP 2020 guidelines, which in turn relies on the 2014 draft report from the WHO, the reports from the SSM and the 2015 report from the Scientific Committee on Emerging and Newly Identified Health Risk(SCENIHR).
There seems to be an “ICNIRP cartel” of experts that dominate different expert evaluations,e.g.,ICNIRP, WHO, SSM, SCENIHR. This seems also to be the case in this Health Council report, see Table 1.
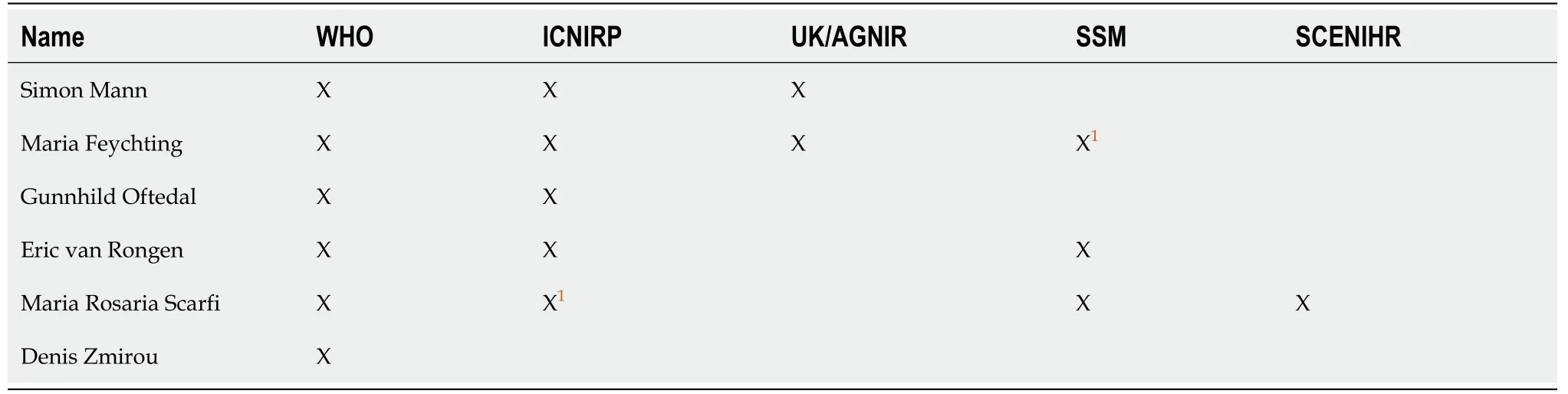
Table 1 Members of World Health Organization monograph core group and their involvement in other groups, see Hardell[16], 2017
As a general rule, scientists who are of the opposing opinion,i.e., that there are health risks associated with exposure to RF radiation, have never been invited to take part of these expert groups. Thus, the opinions expressed in these reports are not representative of the opinions in the scientific community on effects from EMFs(https://www.emfscientist.org).
It is pertinent to evaluate the current ICNIRP 2020 conclusions on cancer risks from RF radiation because the Health Council of the Netherlands recommends using the ICNIRP 2020 guidelines. The recommendation to “take a cautious approach and keep exposures as low as reasonably achievable” is certainly difficult to achieve on a market with expanding wireless communication and may be of no practical use. It is assumed that the ICNIRP 2020 guidelines will be used in most countries. Thus, the influence by ICNIRP and its members on reports that form the basis for guidelines by different organizations is necessary to elucidate.
The ICNIRP
In the following, the evaluation of increased cancer risks according to ICNIRP 2020 is discussed in more detail. It should be mentioned that ICNIRP relies only on thermal(heating) effects from RF radiation. Nonthermal effects are dismissed thereby neglecting a large amount of scientific evidence on harmful nonthermal effects, for instance DNA damage[4], oxidative stress[5] and cancer[2]. It should be noted that the International Agency for Research on Cancer (IARC) at the WHO evaluation from 2011 is not included in the report. IARC concluded that RF radiation in the frequency range30 kHz to 300 GHz is a possible human carcinogen, Group 2B after an evaluation by 30 international experts[6,7].
ICNIRP is a non-governmental organization based in Germany. It has obtained major influence worldwide on health risks from RF radiation through its recommended guidelines for limiting RF radiation exposure published in 1998, 2009 and 2020[8-10].
ICNIRP maintains the same attitude towards health effects from RF radiation as the IEEE and its standards setting Committee, the ICES. In fact, several members of ICNIRP are also members of these organizations, for instance van Rongen E, member of ICES since 2000. ICES is dominated by industry and military representatives[11].ICES within IEEE also sets limits for RF exposure, which are in line with the ICNIRP’s opinion that there are only immediate thermal effects, and no effects below those that cause immediate effects due to increased temperature.
As stated in an EU report[12], ICNIRP’s chairman, van Rongen E, was invited in 2016 to the industry organization ICES to comment and thereby influence the upcoming ICNIRP 2020 guidelines. The report concluded that it is “clear from ICES minutes that ICNIRP worked very closely with IEEE/ICES on the creation of the new RF safety guidelines that were published in March 2020. And this implies that large telecom-companies such as Motorola and others, as well as United States military, had a direct influence on the ICNIRP guidelines, which are still the basis for EU- policies in this domain.”
This adds to the evidence that van Rongen E, one of two secretaries of this Health Council, seems to have conflicts of interest.
In 2020, ICNIRP published new guidelines on health risks[10]. These updated guidelines were based on documents from the WHO, the SSM and the SCENIHR, as mentioned earlier, without any new thorough evaluation of its own.
Not one of these three reviews has been published after peer review in a scientific journal. In fact, substantial critique from the scientific community has been expressed against these reviews but has been ignored[13,14]. It should be noted that the most recent research is not covered in these older documents.
WHO
A draft of a monograph on health effects of EMF exposure was released by the WHO in 2014 but has never been published as a final version[15]. Public consultations were open until December 31, 2014.
It should be noted that the WHO in 2014 issued the following statement: “This is a draft document for public consultation. Please do not quote or cite”[15]. Nevertheless,this WHO draft from 2014, issued by a group dominated by ICNIRP members, among them van Rongen E, was used as a basis for the ICNIRP guidelines 2020 and this new report by the Health Council of the Netherlands. Five of six members of the WHO core group were members of ICNIRP, see Table 1[16]. The WHO group was nearly identical to ICNIRP.
The SCENIHR
The following quote is from the SCENIHR report 2015[17]: “Overall, the epidemiological studies on mobile phone RF EMF exposure do not show an increased risk of brain tumors. Furthermore, they do not indicate an increased risk for other cancers of the head and neck region…The results of cohort and incidence time trend studies do not support an increased risk for glioma while the possibility of an association with acoustic neuroma remains open.”
The SCENIHR report was criticized for its biased presentation and conclusions[13,14]. Like the WHO draft report and the Swedish reports by SSM, it was written by a group of experts with no representation from the many scientists that report increasing evidence of harmful effects below the ICNIRP guidelines and demand better protection against health risks (https://www.emfscientist.org). SCENIHR included scientists with financial ties to industry or membership in ICNIRP or IEEE.
The SSM
Between 2003 and 2019, the SSM group has published reports in English on its webpage, three cited by ICNIRP 2020[18-20]. In line with ICNIRP, the SSM reports have ignored harmful effects from nonthermal RF exposure. Since the first report in 2003 until today, around half of the group’s members have also been present or previous ICNIRP members. Both van Rongen E and Huss A have been part of this group of SSM experts. In consequence, the conclusions have generally been that there are no health risks below the limits recommended by themselves,i.e.in agreement with ICNIRP.
The 2018 annual report was the twelfth in this series and covered studies published from October 2015 up to and including March 2017. The conclusion was that “No new health risks have been identified”[20].
It should be noted that SSM in April 2020 published a new report from the SSM expert group that concluded: “The results of the research review give no reason to change any reference levels (ICNIRP’s) or recommendations in the field.” Of the ten members in the scientific group, five were present or past members of ICNIRP[21].
Current ICNIRP evaluation
van Rongen E, at that time chair of the ICNIRP Commission, claimed in a press release of the new ICNIRP 2020 guidelines that the 1998 version was “conservative in most cases” and “still provide adequate protection for current technologies.” He also argued that “The most important thing for people to remember is that 5G technologies will not be able to cause harm when these new guidelines are adhered to”[22]. Because there is still no published peer-reviewed research showing no health effects from the new 5G technology, not even from short-term exposure, that is a statement without scientific foundation.
Many incorrect statements were made in the ICNIRP 2020 article[10]. In the following, the section on cancer is commented. That section starts at page 41 in the ICNIRP 2020 article with “There is a large body of literature concerning cellular and molecular processes that are of particular relevance to cancer. This includes studies of cell proliferation, differentiation and apoptosis-related processes, proto-oncogene expression, genotoxicity, increased oxidative stress, and DNA strand breaks. Although there are reports of effects of radiofrequency EMFs on a number of these endpoints,there is no substantiated evidence of health-relevant effects.”
Regarding studies on cancer risks, no current evaluation is made. Several studies are not included, or references are not even given to the discussed studies. This is not easily understood by the reader that is not experienced in this area.
Regarding animal studies yielding a tumor promoting effect from RF radiation[23,24], ICNIRP states that “interpretation of these results and their applicability to human health (is) difficult, and, therefore, there is a need for further research to better understand these results.” In the next paragraph, the recent animal National Toxicology Program (NTP) studies[25,26] and Ramazzini Institute results[27] on animal carcinogenesis from RF radiation are disregarded stating that “no consistency was seen across these two studies” and “within the context of other animal and human carcinogenicity research (HCN 2014, 2016), their findings do not provide evidence that radiofrequency EMFs are carcinogenic.”
That is a remarkable statement with no risk by ICNIRP and is not based on what the science really showed. There is a pattern of increased cancer risk based on human epidemiology, animal research and experimental findings. The Hardell team concluded that “There is clear evidence that RF radiation causes cancer/tumor at multiple sites, primarily in the brain (glioma) and head (acoustic neuroma). There is also evidence of an increased risk of developing other tumor types. The results are similar in both the NTP studies and the Ramazzini Institute findings (Falcioniet al[27]). Based on the IARC preamble to the monographs, RF radiation should be classified as Group 1: The agent is carcinogenic to humans”[28].
In a note published by ICNIRP, it was claimed that the histopathological evaluation in the NTP study was not blinded as to exposure status[29]. This false accusation was rebutted by one of those responsible for the NTP study[30]. However, the rebuttal seems to have had no impact on the current ICNIRP evaluation[10].
Regarding the 13 country Interphone case-control study on glioma[31] and acoustic neuroma[32], ICNIRP concluded that the studies do “not provide evidence of an increased risk,” which is not correct. However, regarding glioma cumulative call-time of mobile phone ≥ 1640 h yielded odds ratio (OR) = 1.40, 95% confidence interval (CI)= 1.03-1.89. The risk increased over time for exposure and was highest in the most exposed parts of the brain. These findings were of biological relevance.
RF radiation dose was estimated in parts of Interphone as total cumulative specific energy (J/kg) absorbed at the tumor's estimated center taking into account multiple RF exposure determinants[33]. The risk increased with increasing total cumulative specific energy 7+ years before diagnosis, OR = 1.91, 95%CI = 1.05-3.47 (Pvalue = 0.01)in the highest quintile. Compared with glioma in other parts of the brain increased,ORs were found for tumors in the most exposed part of the brain in those with 10+years of mobile phone use, OR = 2.80, 95%CI = 1.13-6.94.
Grellet al[34] published similar results for the Interphone study. “We found a statistically significant association between the intracranial distribution of gliomas and the self-reported location of the phone…Taken together, our results suggest that ever using a mobile phone regularly is associated with glioma localization in the sense that more gliomas occurred closer to the ear on the side of the head where the mobile phone was reported to have been used the most.”
For glioma, when comparing those in the highest quartile of use (> 558 lifetime hours) to those who were not regular users, the OR was 2.0, 95%CI = 1.2-3.4 in the Canadian part of Interphone[35]. After adjustment for selection and recall biases, a somewhat higher OR was found, 2.2, 95%CI = 1.3-4.1.
The Interphone study gave for acoustic neuroma statistically significant increased risk. Thus, ipsilateral cumulative mobile phone use > 1640 h gave OR = 2.33, 95%CI =1.23-4.40[32].
Regarding the Hardell team studies, ICNIRP writes: “a set of case-control studies from the Hardell group in Sweden report significantly increased risks of both acoustic neuroma and malignant brain tumors already after less than five years since the start of mobile phone use, and at quite low levels of cumulative call time.” The studies are not carefully evaluated by ICNIRP and no references are given. On the contrary,overall there was no statistically increased risk in the shortest latency period > 1-5 years for glioma or acoustic neuroma[36,37]. Somewhat higher risk was seen for ipsilateral exposure; a promotor effect cannot be excluded in addition to initiation of cancer[36]. Also in the Hardell team studies the risk increased with latency and cumulative use and was highest in the most exposed areas of the brain that would be expected for carcinogenesis. Concepts of both promotion, initiation and biological relevance for RF radiation carcinogenesis must be considered when discussing results in different studies. That is obviously not the case for ICNIRP.
In addition, ICNIRP claims that the Hardell team results may be caused by recall bias. For meningioma, no statistically significant increased risk was found in the same study. Using meningioma cases as “controls” (the comparison entity) still yielded statistically significant increased risk for glioma and mobile phone use[36]. Similar results were found for acoustic neuroma using meningioma cases as the comparison group[37]. These results clearly show that the increased risks for glioma and acoustic neuroma were not caused by recall bias,i.e.cases tending to overestimate exposure.That would have applied to all cases regardless of tumor type.
ICNIRP omitted the CERENAT study by Coureauet al[38]. The study strengthened the evidence of increased risk for glioma associated with mobile phone use. Life-long cumulative duration ≥ 896 h gave OR = 2.89, 95%CI = 1.41-5.93 for glioma. Number of calls ≥ 18360 gave OR = 2.10, 95%CI = 1.03-4.31. Higher risks were obtained for the highest exposed area, the temporal brain lobe, as well as occupational and urban mobile phone use.
In spite of serious methodological limitations, the Danish cohort study on mobile phone use was included, adding to the ICNIRP no-risk conclusion. This study, partly funded by Danish telecom operators, first published in 2001[39] and updated in 2011[40], reported no increased risks of tumors in the central nervous system. It was based on 420095 mobile phone private subscribers. This group’s incidence of brain tumors was compared to the incidence within the rest of the Danish population (control group). However, there are several methodological limits in the study such as inclusion only of mobile phone private subscribers in Denmark between 1982 and 1995 in the exposure group. The most exposed group, corporate users, and subscription in 1996 or later were excluded. Use of cordless/DECT phones was disregarded although shown to be a risk factor for brain and head tumors[36,37].
The study has been called “The most severely biased study among all studies published so far”[41]. Certainly, there were severe methodological flaws. The Danish cohort study was regarded by IARC in the 2011 evaluation[7] to be uninformative regarding cancer risks due to serious exposure misclassification. However, it was included by SCENIHR[17], WHO[15], SSM (2013)[42], and ICNIRP[10] as evidence of no risk. The statement by SSM 2013[42] that “The Danish cohort studies make an important contribution to the total assessment in the field” is not correct. The shortcomings in the study should have been known to the SSM expert panel as discussed in a peer-reviewed article[43] concluding that “After reviewing the four publications on the Danish cohort study, one might rightly wonder whether this cohort was initially set up to show no increased risk.”
The ICNIRP 2020[10] reference levels for RF radiation are based on time averaged exposure over 6 min or 30 min. However, pulses from different RF radiation sources may give much higher peak radiation from short time pulses than the power density average. Using time averaging in reference values may thus underestimate the risk. In addition, ICNIRP 2020 suggests higher guidelines for local exposure. According to the article, the reference level,e.g.,> 2 to 6 GHz local exposure, is suggested to increase to 40 W/m2time averaged over 6 min. This is contrary to the increasing scientific evidence on detrimental effects on human health and the environment from RF radiation. Previously 10 W/m2was used as reference level time averaged 6 min exposure[8,9]. Now the reference level for whole body exposure, time averaged 30 min, is suggested to be 10 W/m2.
The evidence for cancer
Several meta-analyses have during the last years reached the conclusions that all together the available evidence shows increased risk of cancer from mobile phone use[2]. One additional method is to use Sir Bradford Hill’s viewpoints from 1965 on association or causation written at the height of the tobacco and lung cancer controversy[44]. In an article published in 2017, these viewpoints were used to evaluate RF radiation carcinogenesis based on epidemiology and laboratory studies[45]. It was concluded that based on these Hill “criteria” RF radiation should be regarded as a human carcinogen causing glioma. Since then the evidence has strengthened.
As discussed above, studies have shown an association between glioma and acoustic neuroma and mobile phone use especially in: (1) people with longest latency(time from first use until tumor diagnosis); (2) people with highest cumulative use of mobile phones; (3) people who had used mobile phones on the same side of the head as that on which their tumor developed; and (4) in people whose tumor was in the temporal lobe of the brain,i.e.the highest exposed lobe during use of the handheld wireless phone.
In addition, the Hardell team studies from Sweden found similar results for use of cordless phones. Thus, based on these findings that are of biological relevance and supported by the Hill viewpoints, a causal interpretation is possible. Thus, RF radiation should be classified as a human carcinogen, Group 1 according to the IARC criteria[45,46]. However, only IARC can make that classification.
DISCUSSION
In order to achieve sustainable development, policies must be based on the precautionary principle. No doubt there are threats of serious or irreversible damage by exposure to RF radiation, not the least the increased risk for glioblastoma with short survival for those affected[47]. Lack of full scientific certainty, as proposed by certain public health organizations, should not be used as a reason for postponing measures to prevent environmental degradation. Thus, a moratorium on the deployment of 5G and considerable reduction of RF radiation from existing systems is urgently needed.In short, “The precautionary principle provides justification for public policy actions in situations of scientific complexity, uncertainty and ignorance, where there may be a need to act in order to avoid, or reduce, potentially serious or irreversible threats to health or the environment, using appropriate strengths of scientific evidence, and taking into account the likely pros and cons of proportionate actions and inactions”[48].
In contrast to that as a general rule, ICNIRP, WHO, SSM, and SCENIHR have for many years dismissed available studies showing harmful effects from nonthermal RF radiation exposure and have based their conclusions mainly on studies showing no effects. Thereby results showing health hazards are criticized or not even cited in contrast to studies showing no risks that are accepted as evidence of no risk in spite of severe methodological problems. Many of the statements by these agencies are misleading and not correct. They are easily rebutted by reading the relevant publications. In fact, an Italian court ruling linked mobile phone use to tumors already in 2012. Also, later court rulings in Italy have come to the same conclusion.
These ICNIRP cartel dominated expert groups consequently reach similar conclusions that there are no health effects below ICNIRP guidelines. Scientists with opinions that there is increasing evidence of health risks below the ICNIRP guidelines,e.g.,as expressed in the EMF Scientists Appeal, are not invited to expert groups at the WHO, the EU (SCENIHR), the SSM, or ICNIRP. Table 1 clearly illustrates that few persons constitute different groups aimed at preventing hazards and risks to the health and the environment. The ICNIRP view is thereby influencing these expert reports, which also formed the basis for this Health Council report in the Netherlands.
There is growing scientific evidence on health risks from the RF radiation emitted by existing telecommunications systems prior to 5G. In addition, 5G will lead to an increase of radiation, including new techniques, which leads to the conclusion that hazardous exposure will increase. However, it is unacceptable that there is scanty research being performed on the risks or hazards from the new 5G technology and the new frequencies that will be used. This means an experiment on human health and the environment that should not be accepted. Thus informed consent would be needed from each involuntary exposed person. The exposure guidelines in ICNIRP 2020[10]constitute a hazard to public health and the environment because evidence is abundant on harmful effects including DNA damage, oxidative stress, and cancer.
The Health Council Committee argues that “epidemiological research into the relation between exposure to the 5G frequencies used and the incidence of cancer,reduced male fertility, poor pregnancy outcomes and birth defects” should be performed after the roll-out of the 5G and its increase in radiation. However, the same Committee in the same report claims that “The committee has however classified relations as “possible” for cancer, male fertility, pregnancy outcomes and birth defects.”
Further the Committee states that “The conclusions from those earlier reports are also relevant for 5G as far as the frequency bands around 700, 1400, 1800 and 2100 MHz are concerned. The committee sees no reason to limit or stop the use of the lower frequency bands for 5G. Frequencies near 700 MHz and 3.5 GHz have been in use for current telecommunication systems or other applications such as Wi-Fi for years,without any demonstrable health damage as a result.”
Thus, this report states that 5G at the lower frequencies has no “demonstrable health damage, although relations (are), “possible” for cancer, male fertility, pregnancy outcomes and birth defects”.
The least to say is that the Committee is not transparent regarding health risks; they are “possible” but for the roll-out of 5G they are not “demonstrable.” Research on health hazards must be done before exposure, not after, something that is suggested for the higher frequencies. “The committee recommends not to use the 26 GHz frequency band for 5G for as long as the potential health risks have not been investigated.”
For implementation of 5G, regardless of frequency, ethics in medicine should be applied. In medicine the patient must be informed about the risks but also benefits in experimental studies and give written consent for the participation. That should also apply to the deployment of 5G. However, it has not been done so far. The participation is forced upon everybody, which is of course unacceptable from a human rights perspective.
CONCLUSION
In conclusion regarding cancer, current scientific evidence clearly demonstrates an increased risk for glioma and acoustic neuroma for use of mobile and/or cordless phones. In this review other tumor types and health endpoints are not discussed. The increased risk for brain and head tumors is based on human cancer epidemiology studies and is supported by similar tumor types found in animal studies. In fact, these animal studies confirmed the earlier results in case-control studies on increased tumor risk for use of wireless phones (both mobile and cordless phones). Mechanistic aspects on carcinogenesis come from laboratory findings on,e.g.,the increase of reactive oxygen species[5] and DNA damage[4].
The current evaluation by the Health Council of the Netherlands is based on a WHO draft and SSM report. It also recommends using ICNIRP guidelines, considered to be insufficient to protect against health hazards, such as cancer, by the majority of the scientists in this field (https://www.emfscientist.org). The report does not represent a thorough, balanced, objective, and up-to-date evaluation of cancer risks and other hazardous effects from RF radiation. It is also strikingly contradictory as it concludes that serious health effects such as cancer and birth defects are “possible.” Yet it has no objection to the roll-out of 5G and recommends that later studies are performed to study health outcomes such as cancer and birth defects. Thus, no lessons are learned from existing observations on increased cancer risks[49].
The conclusion by the Commission that there is no reason to stop the use of lower frequencies for 5G up to 3.5 GHz because of no “proven adverse health effects,”merely reflects the biased conclusions by ICNIRP dominated groups. Thus that conclusion must be dismissed, and new guidelines for previous and new frequencies must be established considering the new technology, the different propagation pattern for 5G, and increased RF radiation.
A moratorium is urgently required on the implementation of 5G for wireless communication[13]. Ultimately, wired solutions are preferred.
 World Journal of Clinical Oncology2021年6期
World Journal of Clinical Oncology2021年6期
- World Journal of Clinical Oncology的其它文章
- Breast cancer: Muscarinic receptors as new targets for tumor therapy
- Review of 10 years of research on breast cancer patients: Focus on indoleamine 2,3-dioxygenase
- Imaging diagnosis of bronchogenic carcinoma (the forgotten disease) during times of COVID-19 pandemic: Current and future perspectives
- Chemotherapy-induced neurotoxicity in the treatment of gynecological cancers: State of art and an innovative approach for prevention
- Impact of community-based exercise program participation on aerobic capacity in women with and without breast cancer
- Phytochemically rich dietary components and the risk of colorectal cancer: A systematic review and meta-analysis of observational studies