
Mediastinal Tuberculoma Mimicking Malignant Cardiac Tumor:A Case Report
2021-05-12 06:15:00YiqinDingWeiLiYnqiuLiuMinYeLingpingChengDonghongLiuHongLinndFengjunYo
Yiqin Ding ,Wei Li,Ynqiu LiuMin YeLingping Cheng,Donghong LiuHong Lin nd Fengjun Yo
1 Department of Ultrasound,The First Aff iliated Hospital,Sun Yat-sen University,Guangzhou,China
2 Department of Cardiology,Center for Translational Medicine,Institute of Precision Medicine,The First Aff iliated Hospital,Sun Yat-sen University,Guangzhou,China
Abstract Background:The clinical manifestations of cardiac masses are diverse and lack specif city.Here we report a cardiac mass detected by transthoracic echocardiography.Multimodality imaging and pathological f ndings after the operation conf rmed the mass as mediastinal tuberculoma.Case presentation:A 45-year-old male patient was admitted to our hospital reporting chest tightness,weight loss,and dyspnea for 3 months after exercise.Transthoracic echocardiography showed that there were a lar ge number of pericardial effusions and a soft tissue mass measuring 7.7 cm × 4.5 cm in the upper mediastinum,which oppressed the right pulmonary artery and accelerated the blood f ow of the left pulmonary artery.Contrast-enhanced ultrasonography showed degenerative inhomogeneous high enhancement of and an unclear boundary in the mass.Contrast-enhanced chest CT revealed punctate and patchy calcif cation in and uneven enhancement of the mass and the lymph nodes around the aortic arch.The mass was diagnosed as a malignant mediastinal tumor.Pathological analysis of the mass revealed chronic granulomatous tuberculosis.The symptoms abated signif cantly after antituberculosis treatment.The patient remained asymptomatic during follow-up.Conclusion:This report presents a rare case of mediastinal tuberculoma mimicking a malignant cardiac tumor.Multimodality imaging should be incorporated for differentiation of cardiac masses.
Keywords:Cardiac tumor;mediastinal tuberculoma;contrast-enhanced ultrasonography;Modality imaging
Background
The clinical manifestations of cardiac masses are diverse and lack specif city,which makes it diff cult for clinicians to detect and distinguish car -diac masses.Cardiac tumors are rare but can be associated with high morbidity and mortality [1].In recent years,more and more noninvasive imaging methods have been used for cardiac lesions.Twodimensional echocardiography is considered to be a guiding standard imaging examination for the evaluation of cardiac masses [2].Contrast-enhanced perfusion echocardiography has advantages in distinguishing masses from benign and malignant tumors.We report a case of a cardiac mass that was suspected to be a malignant cardiac tumor before the operation and was f nally diagnosed as car -diac tuberculoma by postoperative pathological examination.
Case Presentation
The 45-year-old male patient was admitted to our hospital reporting chest tightness,weight loss,and dyspnea for 3 months after exercise.The physical examination f ndings were normal on admission,and no precordial murmur was found in cardiac auscultation.The patient had lost 7.5 kg in the previous 6 months and reported not having a history of infections such as tuberculosis and hepatitis.The EKG was normal.No obvious abnormality was revealed by laboratory examinations.X-ray examination showed that the left lung had the appearance of ground glass,and the edge was clear.Transthoracic echocardiography (TTE) showed that there were a large number of pericardial ef fusions and a soft tissue mass measuring 7.7 cm × 4.5 cm in the upper mediastinum,which oppressed the right pulmonary artery and accelerated the blood f ow of the left pulmonary artery (Figure1A).The ejection fraction was 68%.
To distinguish the mass clearly,contrastenhanced ultrasonography (CEUS) was performed immediately.For the CEUS examination,the ultrasound system was switched to the contrast mode,with a mechanical index of 0.1–0.5.CEUS was performed with intravenous administration of 2.0 mL of SonoVue (Bracco,Milan,Italy).The contrast-specif c imaging mode was adjusted to ensure the balance of ultrasound intensity,penetration,and duration of the contrast agent.The mass showed degenerative inhomogeneous high enhancement,and the boundary was unclear(Figure1B).It was diagnosed as a malignant mediastinal tumor.Meanwhile,the patient underwent a contrast-enhanced chest CT scan.Punctate and patchy calcif cation could be seen in ill-def ned lesions (Figure2).Heterogeneous enhancement could be seen in the mass,and the lymph nodes around the aortic arch showed homogeneous enhancement.The CT results also suggested that it may be a malignant tumor.
To identify the cause and make a diagnosis,the patient underwent subxiphoid pericardial window drainage and thoracoscopic mediastinal mass biopsy.Mass tissue and lymph node tissue were taken for pathological examination.The results showed that there were nodules composed of multifocal epithelioid cells in the lymph nodes,and cellulose necrosis could be seen in some of the nodules,which was consistent with chronic granulomatous inf ammation (Figure3).In addition,the pericardial effusion specimen was negative for acid-fast staining.The pericardial effusion showed a large number of lymph cells,but no tumor cell inf ltration.
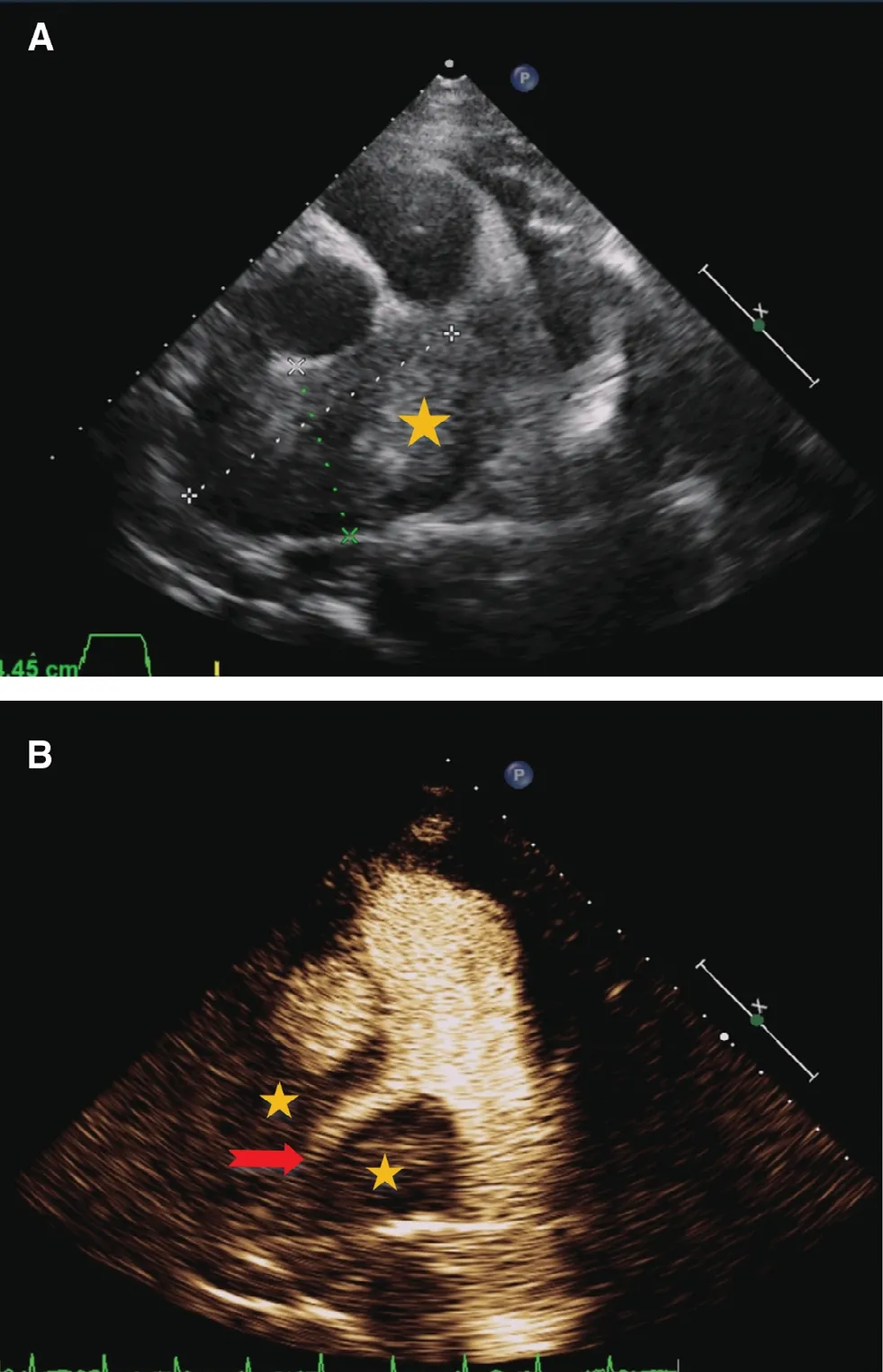
Figure1 Two-Dimensional Transthoracic Echocardiography and Contrast-Enhanced Ultrasonography.
Treatment was started daily with an antituber -culosis regimen of isoniazid (300 mg),rifampin(450 mg),pyrazinamide (750 mg),and ethambutol (750 mg) after the operation.The symptoms abated signif cantly,and the patient was discharged 3 weeks later.In a telephone follow-up,the patient reported that there was no longer chest tightness and dyspnea.
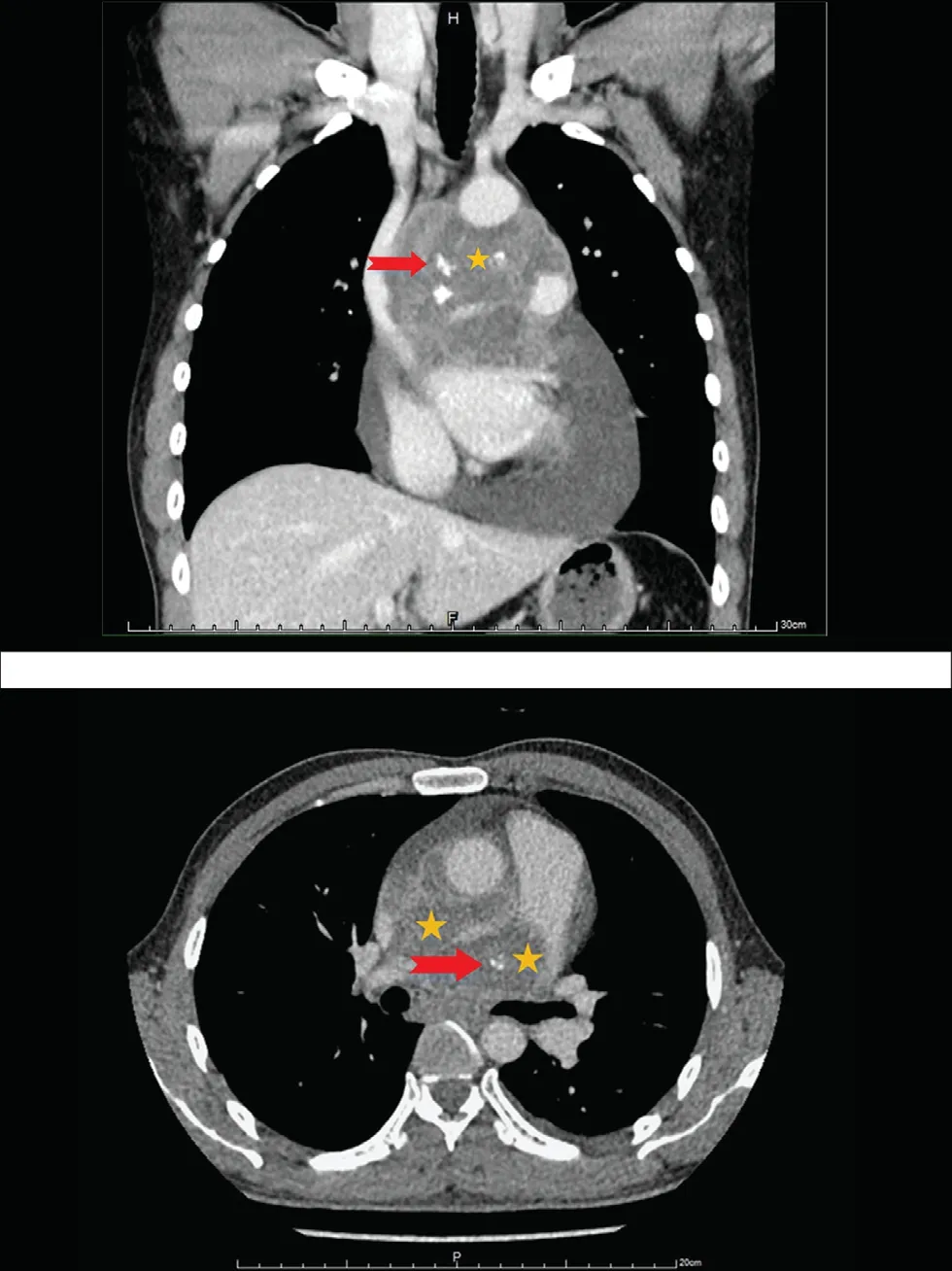
Figure2 Eggshell Calcif cation of the Mass on Contrastenhanced Chest CT Scan at Presentation.
Discussion
The main manifestations in this case were large pericardial effusion and the upper mediastinum mass with heterogeneous enhancement on CEUS and CT.The initial diagnosis was considered to be a malignant tumor;thoracoscopic biopsy conf rmed it was a granuloma.
Cardiac or mediastinal masses are still a challenging problem in TTE [3].Two-dimensional echocardiography is still considered a f rst-line diagnostic method for evaluating cardiac masses,and it is reported that the sensitivity of TTE is 93% and the sensitivity of transesophageal echocardiography is 97% [2].T he diff culty of distinguishing thrombosis and benign and malignant tumors can be reduced by CEUS.The superiority of CEUS lies in observing the perfusion of mass by the degree and kind of enhancement,which can dif ferentiate the neovascularization of malignancy from the avascularity of thrombus and the sparse vascularity of a benign tumor.CEUS can play an instrumental role in the conf rmation of the diagnosis,the delineation of the anatomic extent of the mass,and the evaluation of involvement of other structures that may assist in def ning the nature of the mass and the surgical decision.In addition,some researchers have found that dipyridamole stress quantitative realtime perfusion echocardiography is helpful for distinguishing between benign and malignant tumors[3],which may provide initial guidance for us to use new quantitative techniques such as parametric imaging in the future to better determine the characteristics of tumors [3].
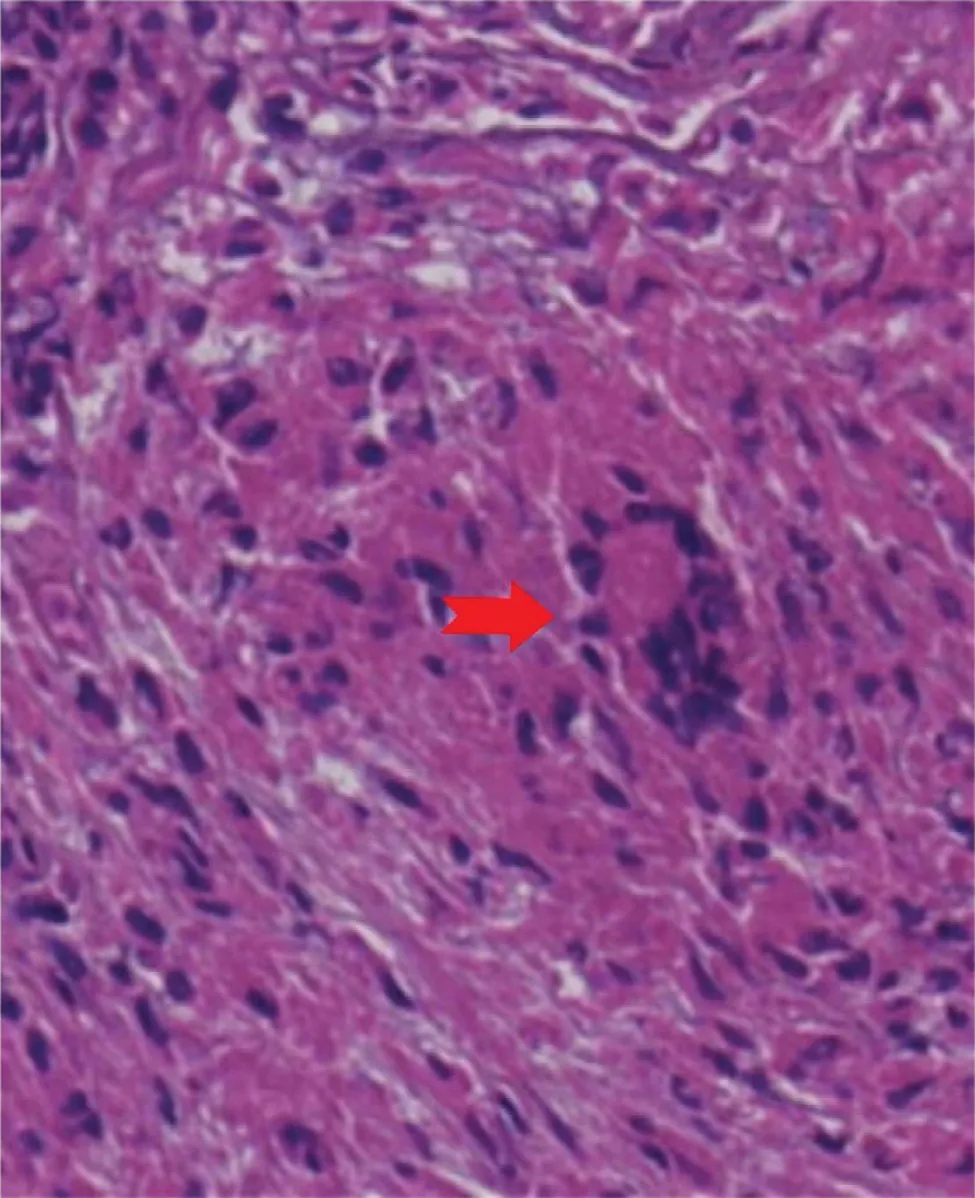
Figure3 Photomicrograph of the Tissue Biopsy Sample Showing a Langhans-Type Giant Cell (with nuclei arranged in a ring at the periphery) Surrounded by Epithelial Cells and Lymphocytes.
Reviewing the whole case,taking into account the results of routine tests and the patient ’ s chief concern and the reported history of no tuberculosis,we did not consider the possibility of tuberculosis at f rst.CEUS showed a mass with degenerative heterogeneous enhancement and an unclear boundary that indicated a hypervascular and irregular projecting mass.We made the preliminary diagnosis of a malignant tumor.CT scan showed punctate and patchy calcif cation,an unclear boundary,and uneven enhancement,which increased the possibility of diagnosis of tuberculosis.Combined with these examinations,subxiphoid pericardial window drainage and thoracoscopic mediastinal mass biopsy were performed.The pathological f ndings indicated tuberculosis.
Tuberculoma,seen as well-de fned nodules located mainly in the right upper lobes,may appear after primary tuberculosis or reactivation.Calcif cation occurs in about 20–30% of cases [4].CT provides the best visualization of the calcif cations and characteristics of the nodules,as well as the lymph gland.CT is also useful for showing the ef fect on the mediastinal cardiovascular structures and tracheobronchial trees.Tuberculous effusions are very rich in proteins and often show f brin strands and septa on ultrasonography [4].On CEUS examination,tuberculoma can show heterogeneous enhancement because of the pathological characteristic by which tuberculoma usually exhibits different stages of inf ammatory exudation,caseous necrosis,and calcif cation simultaneously,and the lymph glands can show rim enhancement because of medullary necrosis.The radiological presentations of tuber -culosis shows some variations,but each modality excels in providing different information.Radiology also plays a vital role in the treatment and follow-up of tuberculosis patients.When a localized mediastinal soft tissue is detected,multimodality imaging combined with the clinical history will increase the degree of diagnostic certainty.
The clinical presentation of tuberculosis has changed to having less classical presentation and increased incidence of extrapulmonary forms [5].The differential diagnosis of masses of the anterior mediastinum and the middle mediastinum includes thymomas,lymphomas,thyroid masses,vascular masses,and lymph node enlargement due to metastases or granulomatous disease [6],Whereas the diagnosis of cardiac tuberculosis was almost exclusively made at autopsy previously,advances in imaging techniques provide an opportunity for earlier diagnosis.These advanced imaging techniques may contribute to an optimal morphological description,assessment of hemodynamic signif cance and surveillance using these advanced imaging techniques [6].
In addition to the imaging f ndings,the differential diagnosis of tuberculoma and tumor in this case can also focus on pericardial ef fusion.Ultrasoundguided pericardiocentesis is helpful for def nite diagnosis.The pericardial f uid is bloodstained in 80% of cases of tuberculous pericarditis.In the study by Mayosi et al.[4],tuberculous pericarditis presented clinically in three forms:namely,pericardial effusion,constrictive pericarditis,and a combination of effusion and constriction.
Conclusion
Although this case was initially not diagnosed by echocardiography and CT because of the variability of tuberculosis,TTE is still considered the f rstline imaging modality for the assessment of cardiac masses.CEUS can conf rm the presence of a car -diac or mediastinal mass and provide information on perfusion,which is used to complement TTE with improved detection of benign or malignant masses.Multimodality imaging plays a pivotal role in the evaluation of cardiac masses.
 Cardiovascular Innovations and Applications2021年2期
Cardiovascular Innovations and Applications2021年2期
- Cardiovascular Innovations and Applications的其它文章
- Myocardial Fibrosis in the Pathogenesis,Diagnosis,and Treatment of Hypertrophic Cardiomyopathy
- Using Three-Dimensional Lorenz Scatter Plots to Detect Patients with Atrioventricular Node Double Path Caused by lnterpolated Ventricular Premature Systoles:A Case Study
- A Case of Pediatric Heart Failure Caused by Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery:Case Report and Literature Review
- Comparison of Diagnostic Effects of T2-Weighted lmaging,DWl,SWl,and DTl in Acute Cerebral lnfarction
- The Relationship between Abnormal Circadian Blood Pressure Rhythm and Risk of Readmission in Patients with Heart Failure with Preserved Ejection Fraction
- Calcium-Sensing Receptor of lmmune Cells and Diseases