
A Case of Pediatric Heart Failure Caused by Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery:Case Report and Literature Review
2021-05-12 06:14:58LeiZhangTieweiLvXiaoyanLiuChuanFengMinZhengJieTianandHuichaoSun
Lei Zhang ,Tiewei Lv ,Xiaoyan Liu ,Chuan Feng ,Min Zheng ,Jie Tian and Huichao Sun
1 Department of Cardiology,Children’ s Hospital of Chongqing Medical University,Ministry of Education Key Laboratory of Child Development and Disorders,Yuzhong District,Chongqing,China
2 China International Science and Technology Cooperation Base of Child,Development and Critical Disorders,Chongqing Key Laboratory of Pediatrics,Chongqing,China
Abstract A female patient aged 3 months and 10 days was admitted to the cardiology department because of symptoms of heart failure.According to the echocardiography results,the patient received a diagnosis of primary endocardial f broelastosis and was treated with γ-globulin,prednisone,digoxin,and diuretics.Coronary computed tomographic angiography and coronary angiography were performed as there was no improvement after 2 months of treatment.Finally,the patient received a diagnosis of anomalous origin of the left coronary artery from the pulmonary artery (ALCAP A).ALCAPA is a rare congenital heart defect that can cause severe heart failure during infancy,and is easily misdiagnosed clinically.In this report,we show the process of misdiagnosis of the case and consult the relevant literature,hoping to improve the understanding and early diagnosis of ALCAPA.
Keywords:heart failure;anomalous origin of a coronary artery;left coronary artery from the pulmonary artery;endocardial f broelastosis
lntroduction
Many cardiovascular diseases can cause heart failure in children,including congenital heart diseases,cardiomyopathies,arrhythmia,and myocarditis.Primary endocardial f broelastosis (EFE) is a common cardiomyopathy in childhood,characterized as hyperplasia of endocardial elastic f bers and diffuse thickening of the endocardium.EFE was classif ed as an unclassif ed cardiomyopathy by the World Health Organization and the International Society and Federation of Cardiology (now the World Heart Federation) in 1995.However,the latest statement on the classif cation and diagnosis of cardiomyopathy in children (American Heart Association,2019) does not mention primary EFE [1].However,primary EFE is a common cardiomyopathy in children,and its treatment strategies and prognosis are different from those of dilated cardiomyopathy;therefore,EFE cannot be completely classif ed as dilated cardiomyopathy.The cause of primary EFE is still unclear,but it is widely accepted that it may be related to viral infection and immune response disorder [2–8].
Currently,the main treatment of EFE is antiinf ammatory with glucocorticoid and γ -globulin besides the usual treatments for heart failure,including positive inotropic drugs,ACE inhibitors,β-blockers,and diuretics [9,10].The prognosis of primary EFE is better than that of dilated cardiomyopathy.Before the diagnosis of primary EFE is established,cardiac diseases that can cause similar pathological changes should be differentiated,such as other kinds of cardiomyopathies,coarctation of the aorta,and anomalous origin of a coronary artery.
Anomalous origins of a coronary artery are a group of rare congenital heart defects,including anomalous aortic origin of a coronary artery(AAOCA),anomalous origin of a coronary artery from the pulmonary artery (ACAPA),and coronary artery f stula.Among ACAPA,anomalous origin of the left coronary artery from the pulmonary artery(ALCAPA),also known as Bland-White-Garland syndrome,is relatively common and severe [11,12].Because of the nonspecif c clinical manifestation of ALCAPA and the limitations of color Doppler examination,it is diff cult to recognize it with echocardiography.The following case was misdiagnosed and treated as primary EFE initially.Because of poor response to treatment,the diagnosis was conf rmed as ALCAPA by coronary computed tomographic angiography (CT A) and coronary angiography.The left coronary artery with anomalous origin was transplanted to the aortic coronary sinus surgically and the normal coronary circulation was restored.The systolic function and the size of the heart gradually returned to normal.
Case
A female patient aged 3 months and 10 days was admitted to the Children ’ s Hospital of Chongqing Medical University (Chongqing,China) because of diff culties in feeding (long time to drink milk,interruption in the process of milk intake,and less milk intake) and profuse sweating for 1 month.There had been no edema,cyanosis,or pneumonia since birth.The mother caught a cold in the f rst trimester of pregnancy without medications.There was no family history of heart disease or sudden death.
Physical examination revealed a respiratory rate of 65 breaths per minute and a heart rate of 158 beats per minute.Pulse oximetry revealed oxygen saturation of 95%.The body weight was 5.5 kg.No edema or cyanosis was found.Cardiomegaly and hepatomegaly were prominent.The heart sound was low and blunt,without arrhythmia and murmur.The liver was swollen and 4 cm below the ribs,with a blunt margin.There was no edema in both legs.The routine blood examination showed a white blood cell count of 9.5 × 109/L (36% neutrophils,62%leukocytes) a red blood cell count of 4.8 × 1012/L,a hemoglobin level of 108 g/L,and a platelet count of 335 × 109/L.The procalcitonin level was less than 0.05 ng/L.The chest X-ray showed signif cant cardiomegaly and no obvious abnormalities in the lung f elds.
The patient showed symptoms of heart failure,including diff culties in feeding,profuse sweating,and low urine output,with an enlar ged heart and liver,so heart failure caused by cardiac disease was suspected f rstly.So we performed echocardiography and ECG f rst.
Echocardiography showed that all chambers were enlarged,especially the left ventricle.The left ventricular end-diastolic dimension was 36 mm.The motion of the interventricular septum and the posterior wall of the left ventricle was decreased.The endocardium of the left ventricle was thickened(2.6 mm).There were hyperplastic and hypertrophied myocardial trabeculations of the left ventricle,and a honeycomb space was found in the anterior septum and the apex of the heart (the ratio of the maximal thickness of the noncompacted layers to the maximal thickness of compacted layers was 1.06).There were mild mitral and tricuspid regur -gitations.The left ventricular ejection fraction was 37%,fraction shortening was 18%,and diastolic function was normal.No obvious abnormality of the coronary arteries was found during this scan.The ECG showed a Q wave in leads V5and V6,and ST-T segment changes in leads
Then cardiac MRI was performed to obtain fur -ther information on the myocardium.The results also showed prominent cardiomegaly and that the ventricular wall and endocardium of the left ventricle were thickened (Figure2).Noncompaction of the ventricular myocardium was not found by MRI.So the diagnosis of EFE was made.Then the patient was treated as having EFE with the usual therapeutic protocols,including γ-globulin,prednisone,digoxin,diuretics,and benazepril.
Two months after treatment,the clinical manifestations showed no positive changes,the thickness of the endocardium had not decreased,and systolic function of the left ventricle had not improved(Table1).So the diagnosis of primary EFE was suspected.As previous ECG showed a abnormal Q wave and ST -T segment depression,coronary CTA was performed.The results suggested there might be a left coronary artery–pulmonary artery f stula (Figure3),so coronary angiography was further performed.
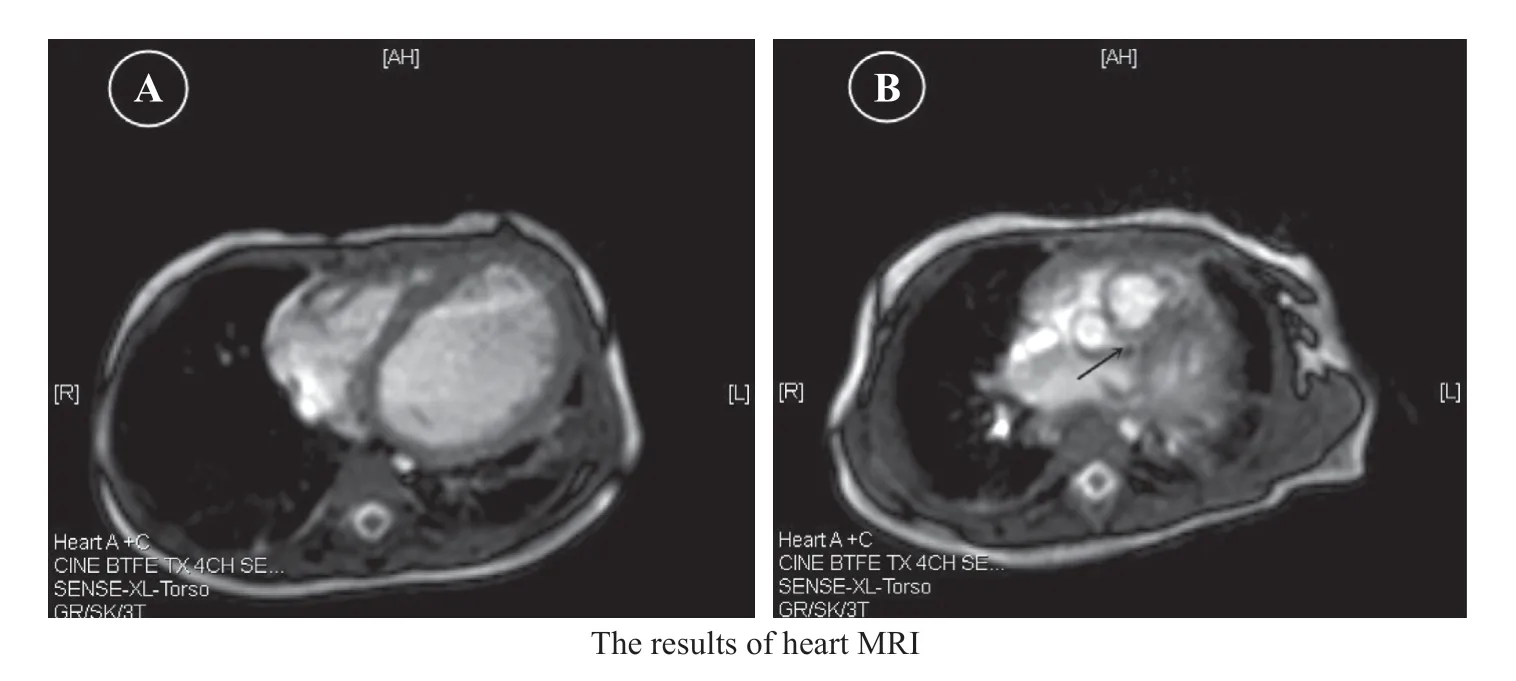
Figure2 (A) Cardiac MRI Showed Thickened Endocardium and no Noncompaction of the Ventricular Myocardium.(B) The Black Arrow Shows the Opening of the Left Coronary Artery.

Table1 ECG Results After Treatment.

Figure3 (A) Coronary Computed Tomographic Angiography Showed the Pulmonary Artery (PA),Indicating a Left Coronary Artery (LCA)–Pulmonary Artery Fistula.(B) The Left Coronary Artery and the Right Coronary Artery Originated From the Aorta.
During angiography of the aorta,it was found that the right coronary artery originated from the right coronary sinus and was visualized normally,while the left coronary artery was not visualized.A selective right coronary artery angiogram showed that the right coronary artery was dilated,the left coronary artery was visualized,there were abundant communicating branches between the left and right coronary arteries,and the pulmonary artery was visualized too (Figure4).So the diagnosis of ALCAPA was then conf rmed.
Then coronary artery replantation was per -formed surgically (Takeuchi operation,reconnecting the left coronary artery of ectopic origin to the aorta).Treatment with digoxin,prednisone,and benazepril was stopped after sur gery.Follow-up by echocardiography showed that the left ventricular dimension and the thickness of the endocardium returned to normal 3 months after sur gery,and systolic function of the left ventricle returned to normal 6 months after sur gery (Table2).The ECG showed the Q wave and the ST -T segment changes disappeared 15 months after sur gery(Figure5).
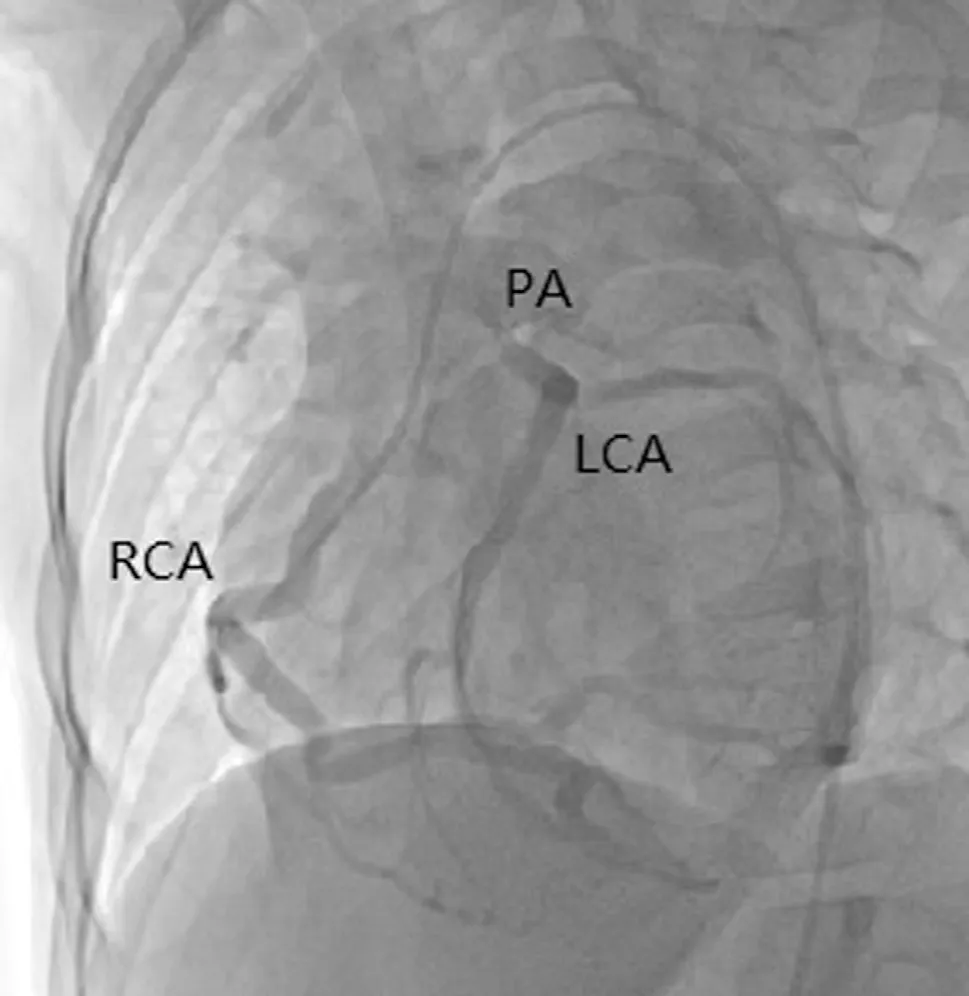
Figure4 Digital Subtraction Angiography.
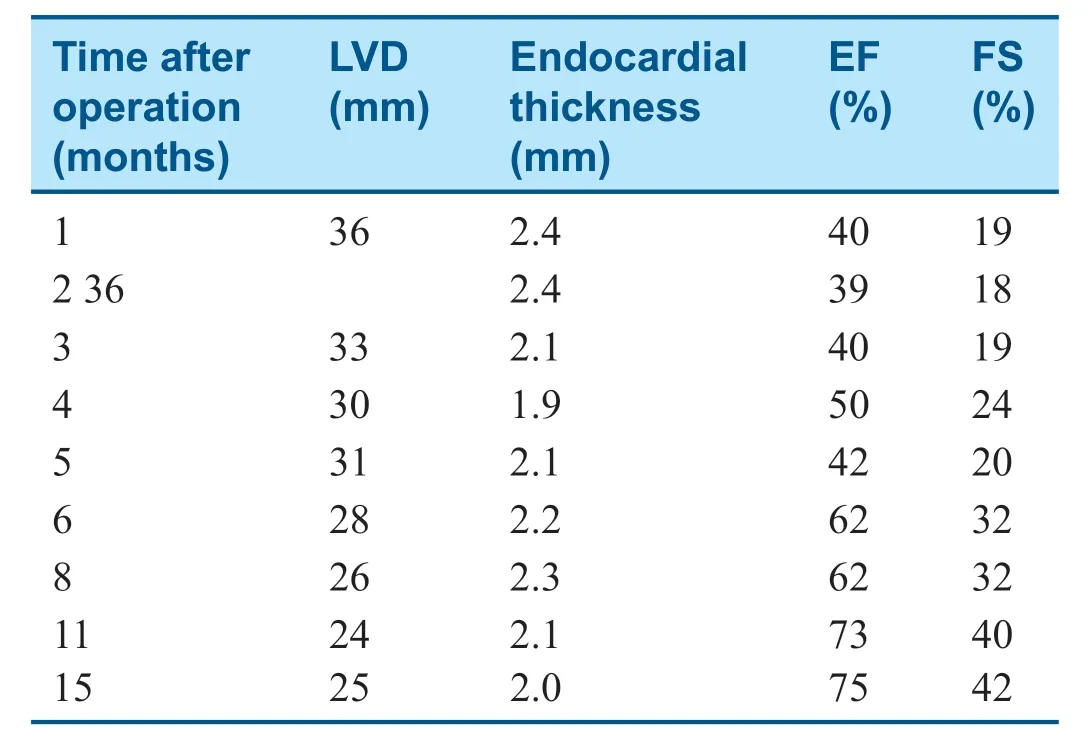
Table2 Follow-up Results After the Operation.
Discussion
The anomalous origin of a coronary artery is caused by the abnormal development of the embryonic coronary artery.According to the site of anomalous origin,these defects can be divided into AAOCA,ACAPA,and coronary artery f stula.For children with AAOCA,the coronary artery still originates from the aorta,so there can be no obvious clinical manifestations.However,when the opening site of the coronary artery is too high,this may lead to a decrease of diastolic coronary blood f ow,coronary ischemia,and left ventricular systolic dysfunction[11–13].
ACAPA includes ALCAPA,anomalous origin of the left anterior descending coronary artery from the pulmonary,anomalous origin of the left circumf ex coronary from the pulmonary artery,and anomalous origin of the right coronary artery from the pulmonary artery,and among these,ALCAPA is relatively common.However,ALCAPA is rare and represents 0.25%–0.5% of all congenital heart defects.Most ALCAPA patients will present with coronary artery steal,myocardial ischemia,mitral regur gitation,and left ventricular dysfunction.The severity of the clinical manifestations is associated with the presence of communicating branches between the right coronary artery and the left coronary artery.
If the communicating branches are abundant,the normal coronary artery can supply arterial blood to the area supplied by a coronary artery with anomalous origin through these branches.However,because of the low pressure in the pulmonary artery,the blood f ow in the coronary artery will enter the pulmonary artery,resulting in the phenomenon of“ coronary artery steal,” and leading to progressive myocardial ischemia and heart failure.Meanwhile,it may share similar presentations as left-to-right shunt congenital heart diseases.
Without communicating branches,blood f ow in the abnormal coronary artery will come from the pulmonary artery,with low perfusion pressure and low oxygen saturation.Severe coronary ischemia and heart failure will develop early in the neonatal period.Most untreated patients will die during the f rst year of life [1 4–17].It is recommended that ALCAPA patients under go sur gical treatment as soon as possible after diagnosis,which is the only way to cure the disease.
Because of the low incidence of ALCAPA and the limitations of two-dimensional echocardiography of the coronary artery,it is diff cult to recognize ALCAPA early in children and it is often misdiagnosed.In this case,heart failure and cardiac enlargement during infancy were the main clinical features.Thickening of the endocardium (>2.5 mm) without other structural abnormalities as observed by echocardiography met the diagnostic criteria for EFE.Subsequent follow-up revealed that the left coronary artery regarded as normal that originated from the aorta during echocardiography was just an illusion on a two-dimensional plane.After coronary CT A and coronary angiography,ALCAPA was conf rmed.
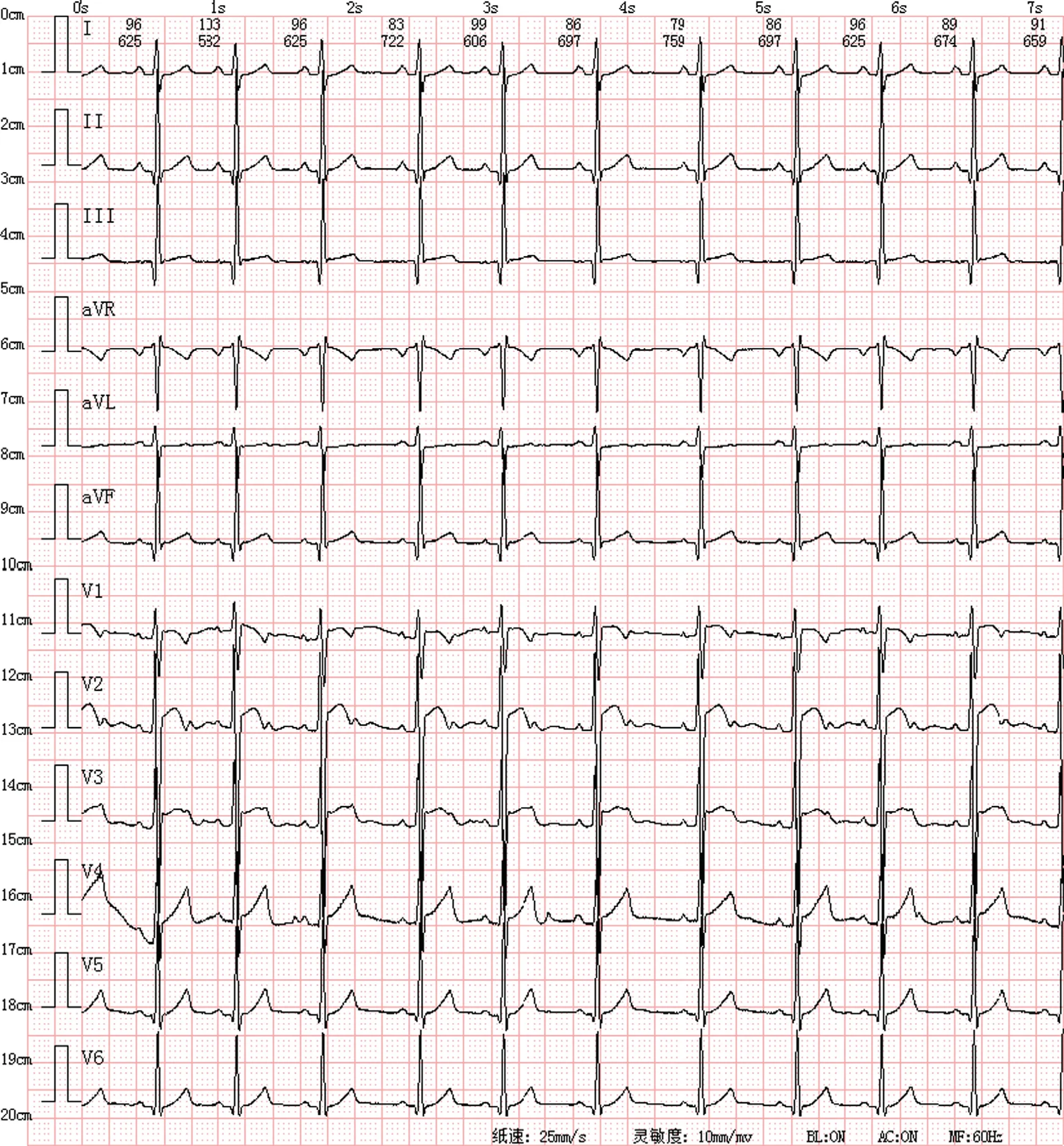
Figure5 The ECG of the Patient 15 Months After the Operation.
Through a literature review,we found several cases of ALCAPA misdiagnosed as EFE [18,19],indicating that misdiagnosis occurs frequently as ALCAPA may also cause thickening of the endocardium.Therefore,it is recommended that primary EFE should be dif ferentiated from ALCAPA.Coronary CTA and coronary angiography should be performed in the following situations:(1) abnormal Q waves with ST-T segment changes in leads I,aVL,and V4–6V,especially an abnormal Q wave and T wave inversion in aVL;(2) one coronary artery dilated without obvious reason,especially when the opening of the other coronary artery and the aortic sinus are not clearly displayed;(3) abundant communicating branches between the left coronary artery and the right coronary artery are found;(4) myocardial ischemia is indicated.Coronary angiography is the gold standard to diagnose ALCAPA.
Acknowledgments
We thank Dr.Qijian Yi and Mi Li for their help with coronary angiography.
Ethics Statement
The patient gave his written informed consent to publish his case (including publication of images).
Conf ilcts of lnterest
The authors declare that they have no conf icts of interest.
Funding Sources
The project was funded by the Natural Science Foundation of Chongqing Science and Technology Commission (cstc2019jcyj-msxmX0866).
Author Contributions
Huichao Sun,Lei Zhang,Tiewei Lv,and Jie Tian wrote the manuscript.Huichao Sun,Lei Zhang,and Tiewei Lv edited the manuscript.Huichao Sun,Tiewei Lv,Xiaoyan Liu,and Jie Tian revised the manuscript.Huichao Sun,Xiaoyan Liu,Min Zheng,and Chuan Feng collected the data.Huichao Sun,Lei Zhang,Tiewei Lv,Xiaoyan Liu,and Jie Tian analyzed the data.All authors read and approved the manuscript.
 Cardiovascular Innovations and Applications2021年2期
Cardiovascular Innovations and Applications2021年2期
- Cardiovascular Innovations and Applications的其它文章
- Myocardial Fibrosis in the Pathogenesis,Diagnosis,and Treatment of Hypertrophic Cardiomyopathy
- Using Three-Dimensional Lorenz Scatter Plots to Detect Patients with Atrioventricular Node Double Path Caused by lnterpolated Ventricular Premature Systoles:A Case Study
- Mediastinal Tuberculoma Mimicking Malignant Cardiac Tumor:A Case Report
- Comparison of Diagnostic Effects of T2-Weighted lmaging,DWl,SWl,and DTl in Acute Cerebral lnfarction
- The Relationship between Abnormal Circadian Blood Pressure Rhythm and Risk of Readmission in Patients with Heart Failure with Preserved Ejection Fraction
- Calcium-Sensing Receptor of lmmune Cells and Diseases