
The Relationship between Abnormal Circadian Blood Pressure Rhythm and Risk of Readmission in Patients with Heart Failure with Preserved Ejection Fraction
2021-05-12 06:14:54
1 Department of Cardiology,the First People’ s Hospital of Fuyang District in Hangzhou,Hangzhou,311400,China
2 Department of Cardiology,the Second Aff iliated Hospital of Chongqing Medical University,Chongqing,400010,China
Abstract Objective:Abnormal circadian blood pressure rhythm has been revealed to be associated with hypertensive tar get organ damage and cardiovascular events,but its association with readmission risk in patients with heart failure with preserved ejection fraction (HFpEF) remains unknown.We conducted a retrospective study to explore the relationship between circadian blood pressure rhythm and readmission risk in HFpEF patients.Methods:We retrospectively collected baseline and follow-up data on HFpEF patients who underwent ambulatory blood pressure monitoring (ABPM) from May 2015 to October 2019.Patient circadian blood pressure rhythms de fned by ABPM were grouped as dipper,nondipper,or riser patterns.Univariate and multivariate linear regression analyses were performed to assess the association between circadian blood pressure rhythm and readmission risk.Results:A total of 122 patients were enrolled in this study.The mean age and ejection fraction were 69.87 years and 61.44%,respectively,with mean the N-terminal pro-B-type natriuretic peptide (N-TproBNP) level being 1048.15 pg/mL.There were signif cant differences in the 24-hour systolic blood pressure (SBP),sleep SBP,and sleep diastolic blood pressure (DBP) among the three groups,where the 24-hour SBP,sleep SBP,and sleep DBP in the riser pattern group were markedly higher than in the dipper pattern group.Notably,serum NT-proBNP levels,the proportion of patients readmitted for heart failure and the mean number of admissions dif fered markedly among three groups.Instructively,multivariate linear regression analysis showed that the riser pattern was a signif cant and independent risk factor for increased serum NT-proBNP level ( β =9 29.16,95% conf dence interval 178.79–1679.53,P=0.016).In multivariate logistic regression analysis,the riser pattern was demonstrated to be a signi fcant risk factor for readmission (odds ratio 11.23,95% conf dence interval 2.01–62.67,P=0.006) in HFpEF patients.Conclusion:The riser blood pressure pattern is a potential risk factor for elevated serum NT-proBNP level and readmission in HFpEF patients.
Keywords:Heart failure with preserved ejection fraction;circadian blood pressure rhythm;ambulatory blood pressure monitoring;riser pattern;N-terminal pro-B-type natriuretic peptide;readmission
lntroduction
Heart failure,the most common reason for hospitalization in patients aged 65 years or older in high-income countries,is a clinical syndrome associated with substantial health care resource utilization,poor life quality,and premature death [1].Epidemiological studies have indicated that up to 50% of patients with heart failure have a preserved ejection fraction,and the proportion of af fected patients has increased over time [2,3].The rates of hospitalization and death in patients who have heart failure with preserved ejection fraction (HFpEF)approach those who have heart failure with reduced ejection fraction.Despite advancements in therapeutic strategies,rehospitalization remains a signif cant challenge in HFpEF,placing a considerable burden on health care systems [4].Furthermore,heart failure readmission carries prognostic implications,with longer hospital stays and worsening prognosis[5].Unraveling the treatable risk factors for readmission in patients with HFpEF may shed light on the development of novel therapeutic strategies.
Measurement of dynamic blood pressure changes over 24 hours by ambulatory blood pressure monitoring (ABPM) is used to reveal an individual ’ s circadian blood pressure rhythm.Recent studies have indicated that the ABPM parameters are more strongly associated with tar get organ damage and cardiovascular disease than are off ce or clinic blood pressure parameters [6].Abnormal circadian blood pressure rhythm has been revealed to be associated with hypertensive target organ damage and prognosis [7].In particular,the riser blood pressure pattern is a type of abnormal circadian blood pressure rhythm in which sleep blood pressure paradoxically exceeds awake blood pressure,and it has been demonstrated to be a risk factor for hypertensive tar get organ damage and cardiovascular events [7–10].However,the association between abnormal circadian blood pressure rhythm and risk of readmission in patients with HFpEF is still unknown.This study aimed to explore the relationship between the circadian blood pressure rhythm and the cardiac function and readmission risk in patients with HFpEF.
Methods
Study Population
This was a retrospective and observational study.We recruited patients who were admitted with a diagnosis of HFpEF (left ventricular ejection fraction of 50% or greater) [11] with New York Heart Association (NYHA) class III or class IV heart failure at the First People ’ s Hospital of Fuyang District in Hangzhou from May 2015 to May 2017.The eligibility criteria for inclusion were as follows:(1) patients underwent ABPM at the baseline;(2) suff cient clinical information,including ejection fraction and N-terminal pro-B-type natriuretic peptide (NT-proBNP) level,was available at baseline;(3) fatal and nonfatal outcomes were available for 18 months of follow-up.Patients with infective endocarditis,myocarditis,malignant tumors,severe liver disease,dementia,delirium,and other severe noncardiovascular diseases were excluded.Baseline ABPM data were collected after the stabilization of heart failure symptoms during the patients ’ f rst hospitalization.The study enrolled 122 patients with HFpEF of NYHA class III or class IV.The circadian blood pressure rhythm was determined on the basis of the results of ABPM,and the patients were divided into dipper pattern,nondipper pattern,and riser pattern groups accordingly.
For each patient,baseline characteristics,including age,sex,body mass index (BMI),NYHA class,medical history,laboratory and echocardiographic data,and medications on admission were collected.The study was approved by the Ethics Committee of the First People ’ s Hospital of Fuyang District in Hangzhou,and informed consent was obtained from all patients according to the Declaration of Helsinki’ s Ethical Principles for Medical Research Involving Human Subjects.
Def initions
Heart failure readmission was def ned as one or more admissions due to heart failure during 18 months of follow-up after dischar ge of the patients from their f rst hospitalization,and the primary end point was heart failure readmission occurrence.The NT-proBNP levels were def ned as the baseline level.The glomerular f ltration rate was estimated with the Japanese Society of Nephrology equation as follows:estimated glomerular f ltration rate (eGFR)(mL/min/1.73 m2)=194 ×C− 1.094 ×A− 0.287 (× 0.739 for women),whereCis the serum creatine concentration andAis the age [12].BMI was calculated as weight (in kilograms) divided by height (in meters)squared.A history of hypertension was def ned by blood pressure of 140/90 mmHg or greater,on the basis of medical records,and on the basis of use of antihypertensive medications.A history of diabetes mellitus was def ned by a fasting glucose level of 126 mg/dL or greater,on the basis of medical records,and on the basis of the use of antidiabetic medications.
Ambulatory Blood Pressure Monitoring
When the patients ’ heart failure symptoms were stabilized,a single session of noninvasive ABPM was performed by an automatic system with electric cuff inf ation (model 90127,Spacelabs Healthcare,Snoqualmie,WA,USA),and measurements were obtained every 20 minutes during the awake time and every 30 minutes during the sleep time.A minimum of 20 valid awake readings and six valid sleep readings were recorded to def ne the awake blood pressure and the sleep blood pressure,but all par -ticipants had more valid readings.Individuals were instructed to rest or sleep during nighttime and maintain usual daytime activities.
The nocturnal blood pressure fall (%) was calculated as the dif ference between the awake systolic blood pressure (SBP) and the sleep SBP divided by the awake SBP.Then we classif ed patients into three patterns by the circadian blood pressure rhythm:dipper pattern if the nocturnal blood pressure fall was greater than 10%,nondipper pattern if it was between 0% and 10%,and riser pattern if it was less than 0%.As the number of patients with extreme dippers (nocturnal blood pressure fall greater than 20%) was small (n=4) in this study,patients with extreme dippers were classif ed as the dipper pattern group in the present study.A nonriser pattern,which includes a dipper pattern and a nondipper pattern,was def ned when sleep SBP was lower than awake SBP.
Biochemical Analyses and Echocardiography
Venous blood samples were collected after patients had fasted overnight for determination of blood glucose and serum creatinine levels.Serum NT-proBNP levels were measured by a two-site sandwich electrochemiluminescence immunoassay(Elecsys proBNP II,Roche Diagnostics,Mannheim,Germany) with a Modular Analytics Evo analyzer with an E170 module (Roche).
Transthoracic two-dimensional echocardiography(LOGIQ 7,GE Healthcare,Chicago,IL,USA) was performed in all patients.The left ventricular enddiastolic dimension were measured in the M-mode,and the left ventricular ejection fraction was calculated by the Teichholz method.
Statistical Analysis
Continuous variables conforming to the normal distribution were described as means with standard deviations,and the one-way ANOVA test was used for comparison between groups.The categorical variables were presented as numbers and percentages and compared with the Pearson chi-square test.Multivariate linear regression models were used to assess the inf uence of circadian blood pressure rhythm on the serum NT-proBNP level,with adjustment for age,sex,BMI,history of hypertension,24-hour SBP,sleep SBP,sleep diastolic blood pressure (DBP),use of β blockers,and eGFR.To evaluate the predictive value of circadian blood pressure rhythm for heart failure readmission,we developed a series of logistic regression models,incorporating different circadian blood pressure rhythm indices in the presence or absence of clinical factors,including age,sex,BMI,history of hypertension,24-hour SBP,sleep SBP,sleep DBP,use of β blockers,NT-proBNP,and eGFR.P <0.05 was considered signif cant.All statistical analyses were performed with SPSS Statistics,version 22.0 (IBM,Armonk,NY,USA).
Results
Baseline Characteristics in Patients with HFpEF
The mean (± standard deviation) age of all patients with HFpEF was 69.87 ± 11.49 years,and the proportion of male patients was 55.7%.We classif ed the 122 patients into dipper pattern,nondipper pattern,and riser pattern groups on the basis of the circadian blood pressure rhythm and compared their baseline clinical characteristics (Table1).There were no signif cant differences in age,sex,BMI,and NYHA class among the three groups (Table1),and the biochemical indicators of eGFR and fasting blood glucose level did not dif fer signif cantly among the three groups (Table1).In addition,a history of hypertension,diabetes,and atrial f brillation,and the prescription of angiotensin-converting enzyme inhibitors,angiotensin receptor blockers,β-receptor antagonists,Ca2+antagonists,or diuretics did not differ markedly among the three groups(Table1).Notably,there were signif cant differences in serum NT-proBNP levels among the three groups(Table1),although neither the left ventricular ejection fraction nor the left ventricular end-diastolic dimension was markedly dif ferent (Table1).Most importantly,the proportion of patients readmitted for heart failure,the mean number of heart failure admissions,and the proportion of patients readmitted for all causes,but not heart failure admission duration or all-cause deaths,dif fered signif cantly among the three groups (Table1).
ABPM Parameters in Patients with HFpEF
As shown in Table2,there were signif cant differences in 24-hour SBP,sleep SBP,and sleep DBP among the three groups,with no marked changes in 24-hour DBP,awake SBP,and awake DBP.Moreover,24-hour SBP,sleep SBP,and sleep DBP in the riser pattern group were signif cantly higher than in the dipper pattern group (Table2),and the sleep DBP in the nondipper pattern group wasmarkedly higher than in the dipper pattern group(Table2).
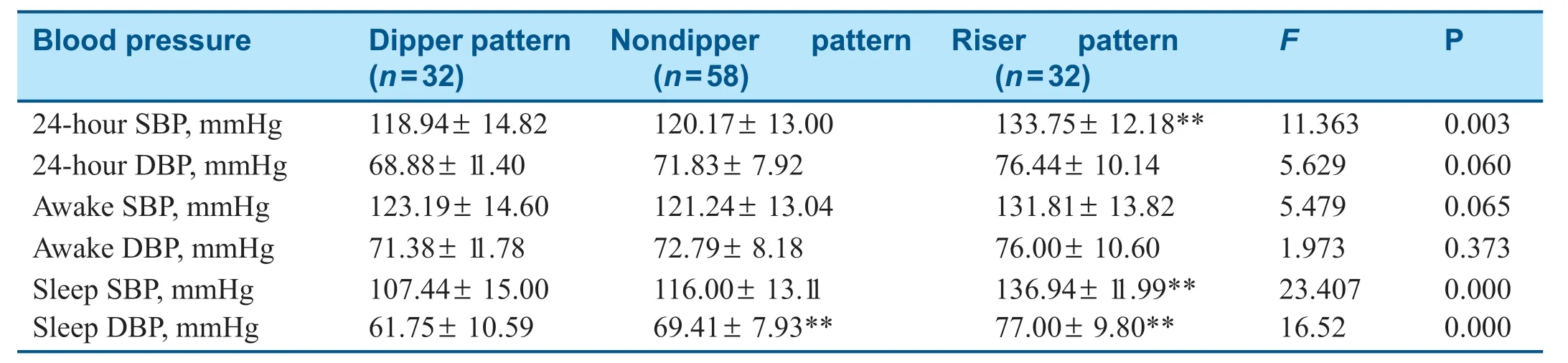
Table2:Ambulatory Blood Pressure Parameters in Different Groups.
The Relationship between Abnormal Circadian Blood Pressure Rhythm and Serum NT-proBNP Level in Patients with HFpEF
Univariate linear regression analysis showed that the riser pattern versus the nonriser pattern (which includes the dipper and nondipper patterns) was associated with a signif cantly elevated serum NT-proBNP level in patients with HFpEF (Table3).However,the riser pattern versus the dipper pattern and the nondipper pattern versus the dipper pattern were not correlated with serum NT-proBNP level in patients with HFpEF (Table3).We then performed a multivariate linear regression analysis to investigate factors associated with elevated serum NT-proBNP levels in patients with HFpEF.After adjustment for age,sex,BMI,history of hypertension,use of β blockers,24-hour SBP,sleep SBP,sleep DBP,and eGFR,the riser pattern ver -sus the nonriser pattern was still associated with a signif cantly increased serum NT-proBNP level in HFpEF patients (β=929.16,95% conf dence interval 178.79–1679.53,P=0.016),indicating its independent predictive value.

Table3:Univariate and Multivariate Linear Regression Analysis of the Relationship between Circadian Blood Pressure Rhythm and Serum N-terminal pro-B-Type Natriuretic Peptide Level in Patients with Heart Failure with Preserved Ejection Fraction.
The Relationship between Abnormal Circadian Blood Pressure Rhythm and Readmission Risk in Patients with HFpEF
Univariate logistic regression analysis showed that the riser pattern versus the nonriser pattern was associated with a signif cantly increased risk of readmission in patients with HFpEF (Table4).Furthermore,the riser pattern versus the dipper pattern,but not the nondipper pattern versus the dipper pattern,was correlated with an increased risk of readmission in patients with HFpEF (Table4).We then performed a multivariate logistic regressionanalysis to investigate factors associated with increased readmission risk in patients with HFpEF.After adjustment for age,sex,BMI,history of hypertension,use of β blockers,24-hour SBP,sleep SBP,sleep DBP,NT-proBNP,and eGFR,the riser pattern versus the nonriser pattern was still associated with a signif cantly increased readmission risk for HFpEF patients (odds ratio 1 1.23,95% conf -dence interval 2.01–62.67,P=0.006).In addition,the riser pattern versus the dipper pattern was also associated with a markedly increased readmission risk in patients with HFpEF (odds ratio 2.84,95%conf dence interval 1.00–7.87,P=0.047).However,the nondipper pattern versus the dipper pattern was not associated with the risk of readmission in patients with HFpEF (Table4).

Table4:Univariate and Multivariate Logistic Analysis of the Relationship between Circadian Blood Pressure Rhythm and Readmission Rates in Patients with Heart Failure with Preserved Ejection Fraction.
Discussion
The present study demonstrates that 24-hour SBP,nocturnal SBP,and nocturnal DBP of HFpEF patients with the riser pattern were signif cantly higher than that in HFpEF patients with the dipper pattern,and the riser pattern versus the nonriser pattern was associated with a signif cantly increased serum NT-proBNP level and risk of readmission due to heart failure.The riser pattern constitutes an independent risk factor for elevated serum NT-proBNP level and readmission in patients with HFpEF.
Individuals with normotension have a pronounced diurnal rhythm in blood pressure.Blood pressure falls to its lowest level during the f rst few hours of sleep,and then surges markedly in the morning,coinciding with the transition from sleep to wakefulness.The average dif ference between daytime and nighttime SBP and DBP is 10 to 20% [13].The riser pattern is a manifestation of abnormal circadian blood pressure rhythm,and is associated with hypertensive tar get or gan damage and poor car -diovascular prognosis [14,15].Our analysis found associations between riser blood pressure pattern and increased readmission risk in patients with HFpEF independent of 24-hour SBP and sleep SBP,indicating a pathophysiological mechanism beyond blood pressure.There are three possible mechanisms accounting for this phenomenon.Firstly,the riser pattern is associated with advanced vascular disease,such as endothelial dysfunction and accelerated arterial stiffness [15].Secondly,the riser pattern has been demonstrated to be associated with increased circulating volume [16].Thirdly,the riser pattern is manifested as a higher sympathetic nerve activity [17].Recent clinical studies have shown that renal denervation signif cantly reduced 24-hour blood pressure,including nighttime blood pressure[18].All these factors contribute to the progression of heart failure by increasing cardiac preload or afterload,or directly impacting on the left ventricular remodeling.
ABPM can be used to measure 24-hour dynamic changes of blood pressure,blood pressure variability,and circadian blood pressure rhythm.Recent clinical studies have shown that ABPM parameters are more strongly associated with tar get or gan damage and cardiovascular disease events than off ce or clinical blood pressure parameters [6,8].Consistent with previous studies,we found that 24-hour SBP,sleep SBP,and sleep DBP in HFpEF patients with the riser pattern were signif cantly higher than in HFpEF patients with the dipper pattern.In clinical practice,physicians often initiate and intensify antihypertensive medications on the basis of off ce blood pressure.Thus,daytime blood pressure might be well controlled,but this may leave a proportion of medicated patients with undetected nocturnal hypertension,placing them at high risk of cardiovascular events.Recent studies have shown that both high nocturnal blood pressure and abnormal circadian blood pressure rhythm are important risk factors for cardiovascular events [7].Compared with daytime blood pressure,the impact of elevated nighttime blood pressure may depend on the clinical stage of hypertension.In the early stage of hypertension,where patients have upper limits of normal blood pressure or mild hyper -tension,daytime blood pressure may be a more important determinant of left ventricular hyper -trophy.Conversely,the prognostic value of nocturnal blood pressure will increase in patients with treated hypertension.ABPM is a standard method for measuring nighttime blood pressure,but it has not been widely used in clinical practice [19].Home blood pressure monitoring equipment with the function of monitoring nighttime blood pressure has recently become available,but is not yet in widespread use [20].To better manage patients with abnormal circadian blood pressure rhythm,nighttime blood pressure monitoring is therefore routinely needed to reduce the risk of cardiovascular events in these patients.
BNP and NT-proBNP are important biomarkers for evaluating the prognosis of patients with chronic heart failure [21].Compared with BNP,NT-proBNP has a longer half-life and is more ef fective in predicting the risk of readmission.The I-PRESERVE(Irbesartan in Heart Failure with Preserved Ejection Fraction) study found that a baseline NT -proBNP level of more than 339 pg/mL was associated with increased all-cause mortality,cardiovascular readmission,and heart failure readmission in HFpEF patients [22].The PEPCHF (Perindopril in Elderly People with Chronic Heart Failure) study revealed that as the quartile of NT -proBNP level increased,morbidity and mortality for heart failure patients also gradually increased [23].In addition,the CHARM-Preserved (Candesartan in Heart Failure-Assessment of Reduction in Mortality and Morbidity) study indicated that NT -proBNP level greater than 600 pg/mL was the sole predictor of cardiovascular mortality,heart failure readmission,myocardial infarction,or stroke [24].The present study found that the riser pattern is associated with increased serum NT-proBNP levels in patients with HFpEF,indicating its prognostic value.
In summary,abnormal circadian blood pressure rhythm,especially the riser pattern,is an independent risk factor for increased NT -proBNP level and readmission in patients with HFpEF.In clinical practice,more attention should be paid to the cir -cadian blood pressure rhythm with monitoring of ambulatory blood pressure to better manage nocturnal blood pressure and improve the prognosis of patients with HFpEF.
Sources of Funding
This study was supported by grants from the Medical Research Projects of the Chongqing Science and Technology Commission and Chongqing Health Committee (2020FYYX047).
Conf ilcts of lnterest
The authors declare that they have no conf icts of interest.
 Cardiovascular Innovations and Applications2021年2期
Cardiovascular Innovations and Applications2021年2期
- Cardiovascular Innovations and Applications的其它文章
- Myocardial Fibrosis in the Pathogenesis,Diagnosis,and Treatment of Hypertrophic Cardiomyopathy
- Using Three-Dimensional Lorenz Scatter Plots to Detect Patients with Atrioventricular Node Double Path Caused by lnterpolated Ventricular Premature Systoles:A Case Study
- Mediastinal Tuberculoma Mimicking Malignant Cardiac Tumor:A Case Report
- A Case of Pediatric Heart Failure Caused by Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery:Case Report and Literature Review
- Comparison of Diagnostic Effects of T2-Weighted lmaging,DWl,SWl,and DTl in Acute Cerebral lnfarction
- Calcium-Sensing Receptor of lmmune Cells and Diseases