
Dried blood spot sampling as an alternative for the improvement of hepatitis B and C diagnosis in key populations
2021-05-08 05:09
World Journal of Hepatology 2021年4期
Geane Lopes Flores,Helena Medina Cruz,Juliana Custódio Miguel,Lia Laura Lewis-Ximenez,Livia Melo Villar, Viral Hepatitis Laboratory,FIOCRUZ,Rio de Janeiro 21040360,Brazil
Jakeline Ribeiro Barbosa,Jeová Keny Baima Colares, Postgraduate Program in Pathology,Federal University of Ceará,Fortaleza 60020181,Ceara,Brazil
Denise Vigo Potsch, Clementino Fraga Filho Hospital,Federal University of Rio de Janeiro,Rio de Janeiro 21040360,Brazil
José Henrique Pilotto,Nova Iguaçu General Hospital,Nova Iguaçu 26041061,Brazil
José Henrique Pilotto,Molecular Immunology Laboratory,Oswaldo Cruz Institute,Rio de Janeiro 21040360,Brazil
Danielle Malta Lima,Postgraduate Program in Medical Sciences,University of Fortaleza,Fortaleza 60811905,Ceará,Brazil
Carlos Eduardo Brandão-Mello,Marcia Maria Amendola Pires,Escola de Medicina e Cirurgia,Gaffrée & Guinle University Hospital,Federal University of Rio de Janeiro State,Rio de Janeiro 20270901,Brazil
Jurema Corrêa da Mota,Francisco I Bastos,Institute of Communication and Information on Science and Technology in Health,FIOCRUZ,Rio de Janeiro 21040360,Brazil
Abstract BACKGROUND To achieve the elimination of hepatitis B and C,there is an urgent need to develop alternative strategies to increase the access of diagnosis,particularly among key populations such as people living with human immunodeficiency virus (HIV),individuals with coagulopathies and chronic kidney disease (CKD) patients.AIM To evaluate the use of dried blood spot (DBS) in the detection of hepatitis B virus(HBV) and hepatitis C virus (HCV) markers.METHODS A total of 430 individuals comprised of people living with HIV,coagulopathies and CKD provided paired serum and DBS samples. HBsAg,anti-HBc and anti-HCV were tested in those samples using a commercial electrochemiluminescence.Demographic and selected behavioral variables were evaluated to assess possible association with HBV and HCV positivity.RESULTS Using DBS,HBsAg prevalence varied from 3.9% to 22.1%,anti-HBc rates varied from 25.5% to 45.6% and anti-HCV positivity ranged from 15.9% to 41.2% in key populations. Specificities of HBV and HCV tests using DBS varied from 88.9% to 100%. The HBsAg assay demonstrated the best performance in CKD and coagulopathy individuals and the anti-HCV test had a sensitivity and specificity of 100% in people living with HIV. Accuracy of HBV and HCV detection in DBS varied from 90.2% to 100%. In the CKD group,HBsAg positivity was associated with infrequent use of condoms,and anti-HBc positivity was associated with sharing nail cutters/razors/toothbrushes. Anti-HCV reactivity was positively associated with a history of transplantation and length of time using hemodialysis in both specimens. In people living with HIV,only the male gender was associated with anti-HBc positivity in serum and DBS.CONCLUSION DBS with electrochemiluminescence are useful tools for the diagnosis and prevalence studies of hepatitis B and C among key populations and may increase the opportunity to foster prevention and treatment.
Key Words: Dried blood spot; Electrochemiluminescence; Hepatitis B; Hepatitis C; Key populations; Diagnosis
INTRODUCTION
Viral hepatitis is an important public health challenge with an estimated 257 million people living with chronic hepatitis B virus (HBV) and 71 million people living with chronic hepatitis C virus (HCV) worldwide[1,2]. HBV and HCV infection have a heterogeneous distribution in Latin America,where 7-12 million people have been infected with HBV and less than 2% are infected with HCV[3].
Some groups may be exposed more frequently to HBV and HCV infection mainly due to repeated exposure to contaminated blood that may occur during transfusions,hospitalizations,surgeries as well as other invasive procedures (including the management of chronic kidney disease (CKD)viahemodialysis) and last but not least coagulopathy individuals. In these groups,HBsAg prevalence varies from 3.9% to 7.0% and anti-HCV prevalence from 12.6% to 47.0%[4-8]. Another group at-risk for acquiring HBV and HCV is composed of people living with human immunodeficiency virus (HIV),as those viruses share common modes of transmission,such as sexual and parenteral transmission. Among people living with HIV,HBV prevalence varies from 2.8% to 10.3%,while HCV prevalence varies from 4.6% to 6.4%[3,7,9,10].
Diagnosis of infections with these viruses can be difficult in these at-risk groups,such as CKD individuals undergoing hemodialysis,coagulopathy individuals and people living with HIV,due to the difficulty of blood sample collection by venipuncture,their remote location and lack of health care.
In these real-life situations,biosecurity is an ever-present problem. In addition to difficulties affecting proper storage and transport of materials and samples,trained personnel are usually absent or scarce. Dried blood spot (DBS) samples could be a key alternative to serum obtained by venipuncture,which would increase access to diagnosis. These samples are easily collected using finger puncture and can be transported and stored at room temperature. Some studies have demonstrated the detection of HBV and HCV markers using DBS along with enzyme-linked immunosorbent assay in several groups,including monoinfected hepatitis patients and those coinfected with HIV[11-13].
Most studies aiming to detect hepatitis markers in DBS have employed enzyme immunoassays,but recently several laboratories have replaced manual or semimanual enzyme-linked immunosorbent assay with electrochemiluminescence (ECLIA). This technique is highly accurate,presents a low detection limit and delivers results quickly[14]. ECLIA has been used for detecting HBsAg and anti-HCV in DBS samples in monoinfected individuals with high sensitivity and specificity[15]. However,there is no information regarding the performance of ECLIA for the detection of HBV and HCV markers in DBS samples in key populations,such as individuals with coagulopathies,CKD patients and people living with HIV.
The main objective of this study was to investigate the putative influence of HIV infection as well as pathophysiological alterations in individuals with coagulopathies(hemophilia and von Willebrand disease) or CKD,vis-à-vis the performance of optimized ECLIA for the detection of HBsAg,anti-HBc and anti-HCV markers in DBS samples. This study also aimed to provide new data on the prevalence of these markers using DBS coupled with ECLIA.
MATERIALS AND METHODS
Study design and population
A cross-sectional study was conducted in different macro-regions of the country from June 2014 to March 2017. Basic sociodemographic data were collected using a standard questionnaire. While analyzing at-risk populations in Brazil presents inherent limitations in the sample-frames available,this study aimed to create a panel that was as broad as possible to maximize the use of individuals and samples obtained under the protocol.
Convenience samples include those as follows:Coagulopathy individuals,CKD patients and people living with HIV. Potential participants were recruited from hemodialysis clinics. Among them,coagulopathy individuals under follow-up in referral clinics as well as patients from HIV/AIDS services located in the northeastern and southeastern regions of Brazil were recruited.
These geographical domains correspond to an involuntary but insurmountable limitation. Although there are some data on the southernmost regions of Brazil from other research groups,data on the far north and central west locations represent a challenge in terms of budgetary constraints and logistics. To send research teams to such locations and to transport biological samples over such huge distances requires a sustained effort and costs comparable to travel across the whole territory of western Europe. Furthermore in Brazil,personnel (both technicians and ancillary personnel)and sample transportation remain a challenge due to a fractured and sometimes nonexistent aerial and terrestrial network.
Inclusion criteria for the selection of participants were as follows:Individuals of both sexes,aged 18 years or older,attending the healthcare centers involved in this study for their different medical conditions.
Three groups were included in this study:(1) Individuals with coagulopathies(hemophilia and von Willebrand disease) recruited from the coagulopathy outpatient clinic of the public Hematology and Hemotherapy Center of Ceará (Hemoce),located in Fortaleza city; (2) CKD patients on hemodialysis recruited from three private nephrology clinics that receive individuals from the public and private healthcare systems located in the states of Ceará and Rio de Janeiro; and (3) People living with HIV referred to the viral hepatitis ambulatory clinic (FIOCRUZ,RJ) from the gastroenterology outpatient clinic of the Gaffrée and Guinle Hospital (UNIRIO,RJ)infectious disease unit at Nova Iguaçu Hospital and the infectious disease outpatient clinic at the Clementino Fraga Filho Hospital (UFRJ).
Demographic characteristics and risk factors such as behavior,age,gender,marital status and education were defined using categories in the Brazilian Census and major national household surveys (e.g.,PNAD). All patients enrolled read and signed the informed consent form. The FIOCRUZ Ethics Committee approved this study (CAAE No. 34049514.7.3006.5258 e 34049514.7.3009.5051).
Laboratory tests
Paired serum and DBS samples were obtained by venipuncture. Whole blood (6 mL)was collected from each patient and 75 μL of this was applied to a 12 mm,preprinted circular disc on Whatman 903 protein protective card (Whatman,GE Healthcare,NJ,United States). To elute DBS samples,the 12 mm disc of filter paper was cut and transferred to a microtube containing 500 μL of 0.5% PBS/BSA for 18 h to 24 h[15]. The analysis of the serum samples was the gold standard for the detection of HBsAg,anti-HBc and anti-HCV. Serological markers were detected using a commercial ECLIA technique (Cobas E411,Roche,United States).
ECLIA in DBS samples
The ECLIA technique was used for the evaluation of HBsAg,anti-HBc and anti-HCV in DBS samples (Elecsys anti-HCV II,Elecsys HBsAg II and Elecsys anti-HBc II - Roche Diagnostics) following the manufacturer’s instructions. In the anti-HCV and HBsAg assay,samples with sample/cutoff values < 1.0 were considered nonreactive,whereas for the anti-HBc assay,non-reactive samples should have an sample/cutoff value of >1.0.
Statistical analysis
Absolute and estimated infection frequencies were calculated as well as mean and standard deviation of the patients’ sociodemographic and clinical characteristics. For the association study,populations and markers were analyzed using the Chi-square test for homogeneity with aPvalue of 0.05. Variables with a proportion of missing values greater than 10.0% for each diagnostic test were excluded from the analysis.Unadjusted odds ratios (ORs) and respective 95% confidence intervals (95%CIs) were calculated for sociodemographic,behavioral and clinical variables as well as for each one of the diagnostic tests/seromarkers.
Associations were further analyzed using multiple logistic regression. Nonreactive samples were taken as the reference categories to which all other categories were cross-compared,yielding adjusted ORs and respective CIs. Only variables with statistical association at the level of 20% were entered into the multivariate models using a forward stepwise procedure. Maximum likelihood and the Wald test were used to assess the parsimony and fitness of intermediate models contemplating the exclusion or inclusion of different variables. Intermediate models were evaluated using the Hosmer-Lemeshow goodness-of-fit test using a 95%CI.
Taking ECLIA as the gold standard method for the sake of our analysis,sensitivity,specificity and positive and negative predictive values as well as accuracy were calculated for each biological outcome.
RESULTS
CKD patients
Among CKD patients (n= 284),HBsAg,anti-HBc and anti-HCV were detected in serum in 4.6%,39.9% and 16.3% of individuals,respectively and were detected by DBS in 4.9%,33.6% and 15.9% of individuals,respectively. Table 1 shows the sociodemographic and clinical characteristics of this population.

Table 1 Main sociodemographic and clinical characteristics of chronic kidney disease individuals,people living with human immunodeficiency virus and coagulopathy individuals

I_CKD:Chronic kidney disease individuals; HBV:Hepatitis B virus; I_COAG:Coagulopathy individuals; P_HIV:People living with human immunodeficiency virus; STI:Sexually transmitted infection.
Most CKD patients were male (62.7%),over 30-years-old (93.0%),black (72.4%) and had up to 8 years of education (51.1%). The most risk behaviors were:Shared nail cutters/razors/toothbrushes (66.9%),previous transfusion of plasma or blood (63.3%),inconsistent use of condoms (74.4%) and the use of hemodialysis up to 3 times a week(89.5%).
HBV and HCV serological markers in DBS and serum were evaluated according to demographic and clinical data. Only statistically significant data are presented in Table 2. Infrequent use of condoms was associated with HBsAg positivity in serum and DBS (OR = 5.6 for serum and 4.4 for DBS). Sharing nail cutters/razors/toothbrushes was associated with anti-HBc positivity in serum and DBS (OR = 2.7 for serum and 2.6 for DBS). On the other hand,acupuncture and hemodialysis exposure was associated with anti-HBc detection in serum and a history of transplantation in DBS. Anti-HCV positivity was associated with a history of transplantation (OR = 2.8 for serum and DBS) and hemodialysis exposure (OR = 1.01 for both specimens).
People living with HIV
Among people living with HIV (n= 95),the mean age was 44.1 ± 11.4 years. Most individuals were male (61.1%),unmarried (64.8%),over 30-years-old (90.4%) and sharing nail cutters/razors/toothbrushes (74.5%) (Table 1). The prevalence of HBsAg+in serum/DBS was 21.0%/22.1%,of anti-HBc+was 40.0%/45.6% and anti-of HCV+was 25.5%/25.5%.
Table 3 shows the factors associated with the detection of HBV and HCV serological markers using DBS and serum in this group. Male gender (OR = 4.9) and blood transfusion (OR = 4.6) were associated with HBsAg reactivity in serum,while male gender was associated with anti-HBc positivity in serum (OR = 3.2) and DBS (OR =2.9). No variable was associated with anti-HCV in this group.
Individuals with coagulopathy
Among coagulopathy patients (n= 51),the mean age was 31.3 ± 9.4 years and the main characteristics were:Male gender (98.0%),unmarried (66.7%),black (70.8%),had undergone blood or plasma transfusion (70.0%) and had severe hemophilia (71.7%)(Table 1).
The prevalence for each seromarker in serum was 3.9% for HBsAg,31.4% for anti-HBc and 47.1% for anti-HCV. The prevalence for each seromarker from DBS was 3.9%for HBsAg,25.5% for anti-HBc and 41.2% for anti-HCV. It was not possible to make a statistical analysis of this group due to the small size of the sample population.
Performance of ECLIA for HBV and HCV detection using DBS samples in high-risk groups
Among coagulopathy patients,HBsAg assay demonstrated the best performance(100% sensitivity and specificity) followed by anti-HBc (81.3% sensitivity and 100%specificity) and anti-HCV (83.3% sensitivity and 96.3% specificity). Among CKD patients,the best performance was observed for HBsAg (100% sensitivity and 99.6%specificity) followed by anti-HCV (93.5% sensitivity and 99.2% specificity) and anti-HBc (79.6% sensitivity and 97.1% specificity). Among people living with HIV,the best performance was observed for anti-HCV (100% sensitivity and specificity) followed by anti-HBc (97.2% sensitivity and 88.9% specificity) and HBsAg (85.0% sensitivity and 94.7% specificity).
Accuracy varied from 90.2% to 100% and incorrect classification was below 10% in all markers. Estimated prevalence varied between serum and DBS in coagulopathy patients,and CKD individuals showed low values of prevalence using DBS for anti-HBc and anti-HCV. In people living with HIV,estimated prevalence for HBsAg and anti-HBc were higher using DBS (Table 4).
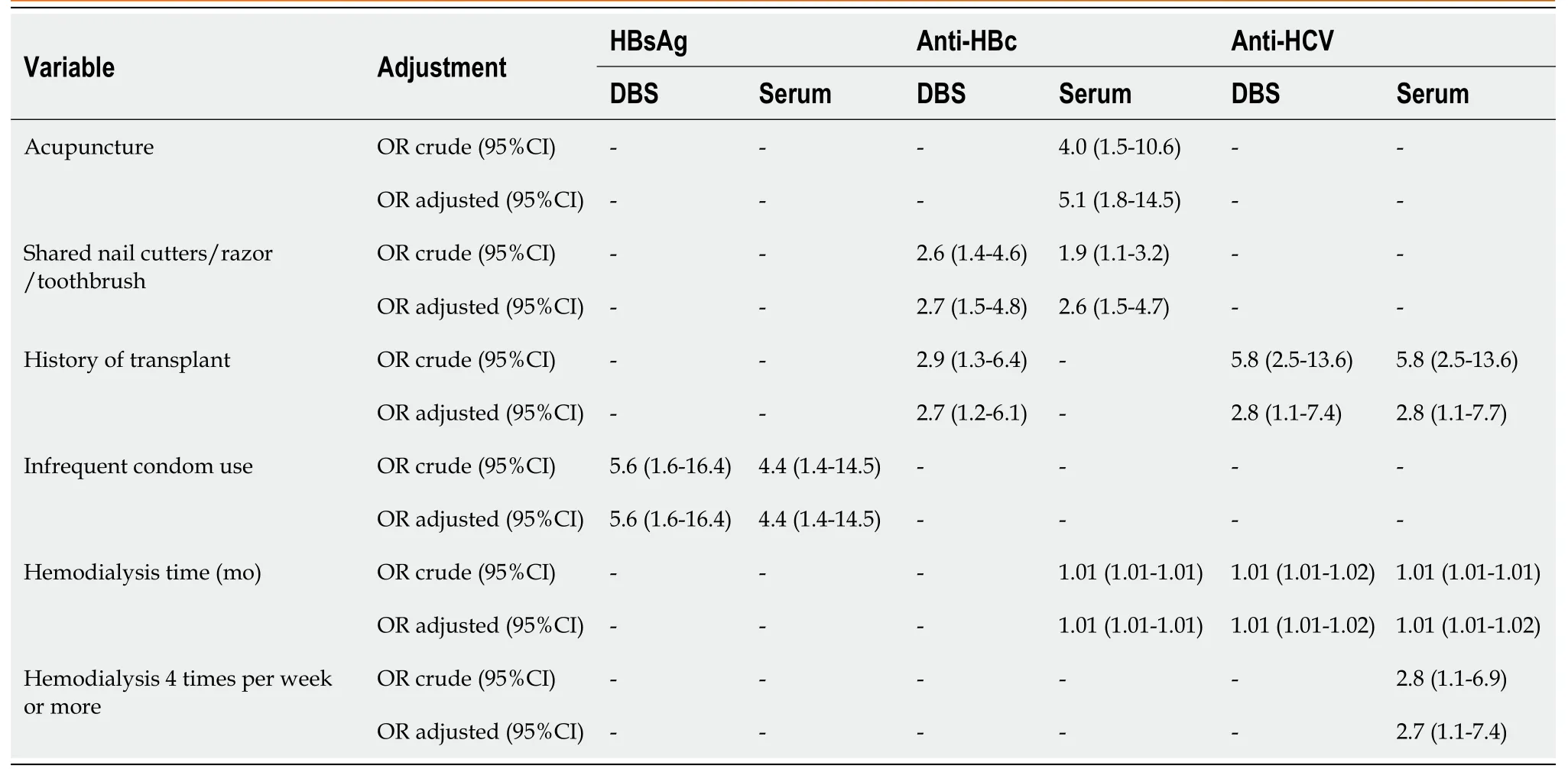
Table 2 Bivariate analysis of sociodemographic and clinical characteristics according to hepatitis B virus and hepatitis C virus markers in chronic kidney disease individuals

Table 3 Bivariate analysis of sociodemographic and clinical characteristics according to hepatitis B virus and hepatitis C virus markers in people living with human immunodeficiency virus
DISCUSSION
To date,there are several studies reporting the importance of diagnosing hepatitis B and C in DBS samples[16-18]. However,the majority have focused only on HBsAg[13,16]and anti-HCV[11]along with manual assays. In the present study,an automated assay was evaluated for the detection of HBsAg,anti-HBc and anti-HCV in DBS samples from key populations demonstrating high sensitivities and specificities comparable to those observed in the general population[15]. These findings reinforce the importance of using DBS samples to reach these key populations in the diagnosis of viral hepatitis,which can be further facilitated using ECLIA.
Among CKD patients,HBsAg positivity in DBS or serum was associated with infrequent condom use,which was also found among young men enlisted in the Brazilian Army,demonstrating the importance of health campaigns with a focus on condom use[19]. Anti-HBc positivity in serum and DBS was associated with shared nail cutters/razor/toothbrush and highlights the discussion of the role of manicurists in the transmission of HBV. Villaret al[20]found a prevalence of 5.9% of anti-HBc in beauty professionals in southeast Brazil.
Anti-HCV positivity in serum and DBS was associated with a previous history of transplantation in CKD patients. A study that assessed the risk of transplant recipient infections showed that this will depend on the prevalence and incidence of HCV in a given population of donors and other risk exposures such as injecting drug use,menwho have sex with men,piercings and tattoos. These,among other risk factors,are already associated with transmission for the general population[21].

Table 4 Test parameter values according to individuals with coagulopathies,chronic kidney disease and people living with human immunodeficiency virus
Among people living with HIV,HBsAg positivity was associated with male gender and blood and plasma transfusion using serum results,and anti-HBc positivity was associated with male gender using the results of both fluids. In Brazil,most HBV infected individuals were male (54.5%)[22],probably due to higher exposure to risk factors,such as promiscuity and drug use[23,24]. Although blood is screened for HBsAg and anti-HBc in blood banks in Brazil,molecular assays were only included in 2015.While rare,occult hepatitis B infection,mutations that escape vaccination and infected individuals occupying a certain immunological window could be potential donors of contaminated blood samples allowing HBV transmission[25,26].
DBS testing for HBsAg,anti-HBc and anti-HCV using ECLIA demonstrated high sensitivity and specificity in all groups. HBsAg testing demonstrated the best performance in coagulopathy individuals and CKD patients. Anti-HCV testing demonstrated higher efficiency in CKD individuals and people living with HIV and anti-HBc detection was more accurate in people living with HIV. The differences observed could be the result of different prevalences and risk behavior,such as multiple exposure to blood products that could interfere in the efficiency of the assay.
HBsAg and anti-HCV prevalence estimated by serum and DBS were similar in demonstrating that ECLIA along with DBS could be a potential tool for diagnosis of infected individuals in key populations. In contrast,anti-HBc prevalence varied by more than 5% between serum and DBS in all groups evaluated. In the present study,anti-HBc sensitivity varies from 79.6% to 97.2%,which is similar to findings in other studies that reported sensitivities from 76.9% to 97.6% using ECLIA or enzyme-linked immunosorbent assay for anti-HBc in the general population and people living with HIV[12,13,16]. Although there are differences found in anti-HBc prevalence in serum and DBS,there is an overlapping CI value for those specimens showing that DBS could be used for prevalence studies in key populations.
CONCLUSION
This study demonstrated the utility of HBsAg,anti-HBc and anti-HCV detection in DBS using ECLIA in high-risk populations. The use of DBS samples is much less invasive,easier than venipuncture and could increase the access of diagnosis in people with limited social access as well as in people where it is difficult to draw blood.Automated assays such as ECLIA using DBS increases diagnostic speed,generating the diagnosis of many samples at once,which can be important during potential outbreaks in hemotherapy clinics for example. However,the anti-HBc marker should be used with due care,especially in the population of coagulopathy individuals and CKD patients,which due to multiple exposures may not show agreement with gold standard samples and therefore requires further study.
ARTICLE HIGHLIGHTS
Research background
Diagnosis of hepatitis B virus and hepatitis C virus (HCV) can be difficult in chronic kidney disease (CKD) individuals undergoing hemodialysis,coagulopathy individuals and people living with human immunodeficiency virus (HIV) due to the difficulty of blood sample collection by venipuncture,remote location and lack of health care.
Research motivation
There is no information regarding the performance of electrochemiluminescence(ECLIA) for the detection of hepatitis B virus and HCV markers in dried blood spot(DBS) samples in key populations,such as individuals with coagulopathies,CKD patients and people living with HIV.
Research objectives
To investigate the putative influence of HIV infection as well as pathophysiological alterations in individuals with coagulopathies (hemophilia and von Willebrand disease) or CKD in the performance of optimized ECLIA for the detection of HBsAg,anti-HBc and anti-HCV markers in DBS samples.
Research methods
The ECLIA technique was used for the evaluation of HBsAg,anti-HBc,and anti-HCV tests in DBS samples of CKD individuals undergoing hemodialysis,coagulopathy individuals and people living with HIV.
Research results
HBsAg detection presented sensitivities of 100% among coagulopathy and CKD patients and low sensitivity (85.0%) in people living with HIV. Anti-HBc detection had the best performance in people living with HIV followed by coagulopathy and CKD patients. Anti-HCV detection showed sensitivities above 83.0% in all groups.Specificities of these assays varied from 88.9% to 100%. Estimated prevalence was similar among serum and DBS except for the anti-HBc marker.
Research conclusions
This study demonstrated the utility of HBsAg,anti-HBc and anti-HCV detection in DBS using ECLIA in high-risk populations.
Research perspectives
Automated assays such as ECLIA using DBS increases diagnostic speed,generating the diagnosis of many samples at once,which can be important during potential outbreaks in hemotherapy clinics.
ACKNOWLEDGEMENTS
The authors would like to acknowledge technicians of the Viral Hepatitis Laboratory,especially,da Silva EF for technical assistance in the sample processing.
 World Journal of Hepatology2021年4期
World Journal of Hepatology2021年4期
- World Journal of Hepatology的其它文章
- Pathologic and molecular features of hepatocellular carcinoma:An update
- Infantile giant cell hepatitis with autoimmune hemolytic anemia
- Long-term albumin infusion in decompensated cirrhosis:A review of current literature
- Bile acid indices as biomarkers for liver diseases I:Diagnostic markers
- Elderly patients (≥80years) with acute calculous cholangitis have similar outcomes as non-elderly patients (<80years):Propensity score-matched analysis
- Retrospective analysis of complications related to endoscopic retrograde cholangio-pancreatography in patients with cirrhosis vs patients without cirrhosis