
血清PGⅠ、PGⅡ、CEA水平及Hp检测在胃癌早期筛查中的应用
2021-03-26 13:36王晓健郭守俊曾庆芳钟建明
中国医学创新 2021年20期
王晓健 郭守俊 曾庆芳 钟建明


【摘要】 目的:探讨血清PGⅠ、PGⅡ、CEA水平及Hp检测在胃癌早期筛查中的应用。方法:选取2020年1-12月在本院确诊的92例胃癌患者为胃癌组,104例慢性胃炎患者为慢性胃炎组,104例胃溃疡患者为胃溃疡组。比较三组血清PGⅠ、PGⅡ、CEA水平及Hp阳性率。绘制ROC曲线并评估PGⅠ、PGⅡ、CEA和Hp在胃癌早期患者筛查中的应用价值。结果:胃癌组患者PGⅠ、PGⅡ水平均低于慢性胃炎组和胃溃疡组,CEA水平高于慢性胃炎组和胃溃疡组,差异均有统计学意义(P<0.05)。胃癌组、慢性胃炎组和胃溃疡组的Hp阳性率分别为92.39%、85.58%和79.81%,三组患者Hp阳性率比较,差异有统计学意义(P<0.05)。PGⅠ、PGⅡ、CEA及Hp预测胃癌发生的曲线下面积分别为0.768、0.721、0.796和0.608,低于PGⅠ、PGⅡ、CEA及Hp联合检测的0.867。结论:血清PGⅠ、PGⅡ、CEA水平及Hp检测对胃癌早期患者筛查具有临床价值。
【关键词】 胃蛋白酶原Ⅰ 胃蛋白酶原Ⅱ 癌胚抗原 幽门螺杆菌 胃癌
Application of Serum PGⅠ, PGⅡ, CEA Levels and Hp Detection in the Early Screening of Gastric Cancer/WANG Xiaojian, GUO Shoujun, ZENG Qingfang, ZHONG Jianming. //Medical Innovation of China, 2021, 18(20): -127
[Abstract] Objective: To explore the application of serum PGⅠ, PGⅡ, CEA levels and Hp detection in the early screening of gastric cancer. Method: A total of 92 gastric cancer patients diagnosed in our hospital from January to December 2020 were selected as the gastric cancer group, 104 cases of chronic gastritis as the chronic gastritis group, and 104 cases of gastric ulcer as the gastric ulcer group. The levels of serum PGⅠ, PGⅡ, CEA and the positive rate of Hp were compared among the three groups. The ROC curve was drawn and the application value of PGⅠ, PGⅡ, CEA and Hp in the screening of early gastric cancer patients was evaluated. Result: The levels of PGⅠ, PGⅡ and CEA of gastric cancer group were lower than those of chronic gastritis group and gastric ulcer group, while CEA level was higher than those of chronic gastritis group and gastric ulcer group, the differences were statistically significant (P<0.05). The positive rates of Hp in gastric cancer group, chronic gastritis group and gastric ulcer group were 92.39%, 85.58% and 79.81%, respectively, and the difference of Hp positive rates among the three groups was statistically significant (P<0.05). The area under the curve for predicting the occurrence of gastric cancer were 0.768, 0.721, 0.796 and 0.608 for PGⅠ, PGⅡ, CEA and Hp, respectively, which were lower than 0.867 for PGⅠ, PGⅡ, CEA and Hp combined detection. Conclusion: Serum PGⅠ, PGⅡ, CEA levels and Hp detection have clinical value in screening patients with early gastric cancer.
[Key words] Pepsinogen Ⅰ Pepsinogen Ⅱ Carcino-embryonic antigen Helicobacter pylori Gastric cancer
First-author’s address: Ganzhou Cancer Hospital, Ganzhou 341000, China
doi:10.3969/j.issn.1674-4985.2021.20.030
胃癌是起源于胃黏膜上皮的惡性肿瘤,早期常无明显症状,或出现与胃炎、胃溃疡类似的嗳气、上腹不适感等非特异性症状,易被忽视而导致早期诊断率降低[1-3]。胃癌的预后与其病理分型分期、部位、组织类型等因素有关,早期发现胃癌病变并及时给予有效的治疗,可提高患者5年生存率。因此,寻求可靠的检测指标对胃癌早期进行检查和诊断至关重要[4-6]。常用的胃癌筛查方法包括胃镜检查、血清胃蛋白酶原Ⅰ(pepsinogen Ⅰ,PGⅠ)、胃蛋白酶原Ⅱ(pepsinogen Ⅱ,PGⅡ)、血清癌胚抗原(carcinoembryonic antigen,CEA)等,胃镜检查虽具有较高的胃癌确诊准确率,但因其属于侵入式操作,部分患者难以配合检查,且检查费用昂贵,限制了其在胃癌早期筛查中的应用[7-8]。PGⅠ与PGⅡ可检测胃黏膜有无受损、受损的程度和部位以及Hp治疗效果[9]。CEA是一种肿瘤标志物,临床常作为胃癌的辅助诊断指标[10]。既往研究已证实,幽门螺杆菌(helicobacter pylori,Hp)与胃癌的发生有关[11-12]。本研究探讨分析了血清PGⅠ、PGⅡ、CEA水平及Hp检测在胃癌早期筛查中的应用,现报道如下。
1 资料与方法
1.1 一般资料 选取2020年1-12月在本院确诊的92例胃癌患者为胃癌组,104例慢性胃炎患者为慢性胃炎组,104例胃溃疡患者为胃溃疡组。(1)纳入标准:①经胃镜下病理活检检查分别符合胃癌、慢性胃炎和胃溃疡诊断标准[13-15];②入组前3个月内未接受任何影响胃肠功能药物或手术治疗。(2)排除标准:①合并严重心、肝、肾等脏器功能不全及其他免疫性相关性疾病;②合并上消化道出血;③合并心理、精神疾病。本研究经医院伦理委员会通过,患者及家属均知情同意。
1.2 方法 于入院后次日清晨,抽取三组患者空腹静脉血5 mL,采用酶联免疫法(试剂盒由上海广锐生物科技有限公司生产)检测血清PGⅠ、PGⅡ、CEA水平,PGⅠ正常参考值67~200 ng/mL,PGⅡ正常参考值0~15 ng/mL,CEA正常参考值0~4.7 ng/mL;
采用13C呼气试验检测三组患者Hp水平,以DOB>4.4‰为阳性,DOB<3.6‰为阴性。
1.3 观察指标与判定标准 比较三组患者血清PGⅠ、PGⅡ、CEA及Hp,其中PGⅠ<67 ng/mL、PGⅡ>15 ng/mL、CEA>4.7 ng/mL为阳性,阳性结果代表胃癌患病风险高。
1.4 统计学处理 采用SPSS 18.0统计学软件进行数据分析,计量资料用(x±s)表示,两两比较采用独立样本t检验,三组比较采用单因素方法分析;计数资料以率(%)表示,比较采用字2检验。采用受试者工作特征(receiver operating characteristic,ROC)曲线分析PGⅠ、PGⅡ、CEA及Hp对胃癌的诊断效能。以P<0.05为差异有统计学意义。
2 结果
2.1 三组患者一般资料比较 三组患者一般资料比较,差异均无统计学意义(P>0.05),具有可比性,见表1。
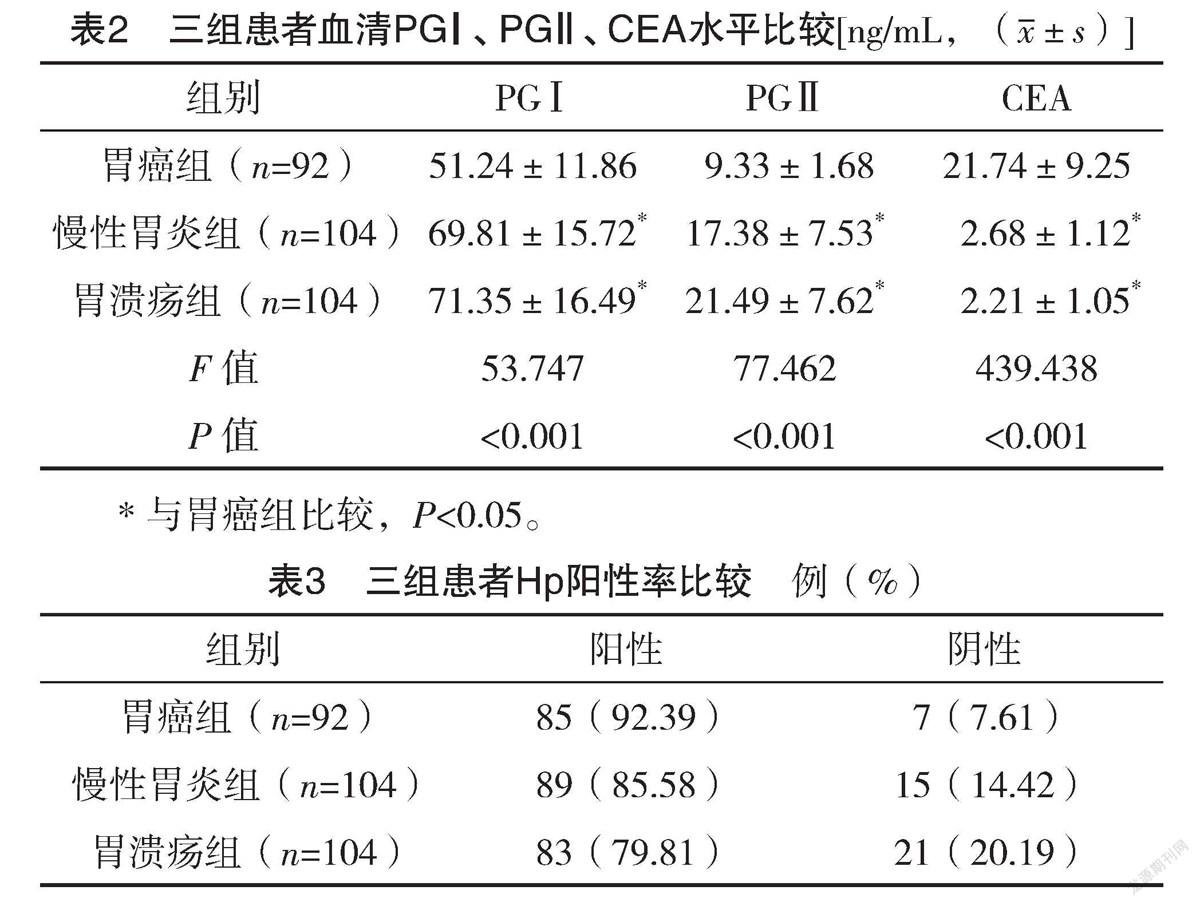
2.2 三组患者血清PGⅠ、PGⅡ、CEA水平比
较 胃癌组患者PGⅠ、PGⅡ水平均低于慢性胃炎组和胃溃疡组,CEA水平高于慢性胃炎组和胃溃疡组,差异均有统计学意义(P<0.05),见表2。
2.3 三组患者Hp阳性率比较 三组患者Hp阳性率分别为92.39%、85.58%和79.81%,三组患者Hp阳性率比较,差异有统计学意义(字2=6.270,P<0.05),见表3。
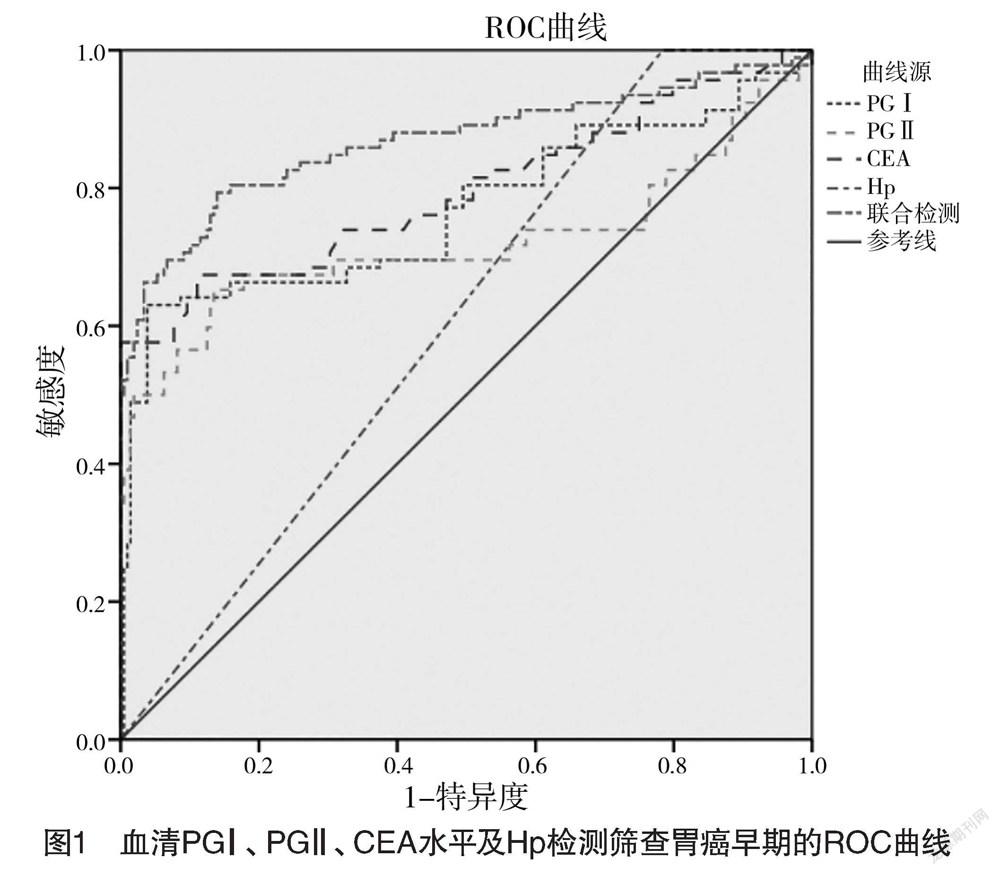
2.4 血清PGⅠ、PGⅡ、CEA水平及Hp检测对胃癌早期的预测作用 采用变量赋值,胃癌组=1,非胃癌组=0。PGⅠ、PGⅡ、CEA及Hp预测胃癌发生的曲线下面积(area under curve,AUC)分别为0.768、0.721、0.796和0.608,PGⅠ、PGⅡ、CEA及Hp联合检测的AUC最大,为0.867,即聯合检测对早期胃癌具有最好诊断价值。见图1、表4。
3 讨论
近年来,胃癌在我国各种恶性肿瘤中发病率逐年上升,给患者身心健康造成严重影响。胃癌早期无论是否有无淋巴结转移,手术后5年生存率均在90%以上,早期筛查和干预对降低胃癌死亡率有重要意义[16]。本研究探讨分析PGⅠ、PGⅡ、CEA水平及Hp检测在胃癌早期筛查中的应用价值。
本研究结果显示,胃癌组患者PGⅠ、PGⅡ水平均低于慢性胃炎组和胃溃疡组,CEA水平高于慢性胃炎组和胃溃疡组,差异均有统计学意义(P<0.05)。既往研究显示,PGⅠ和PGⅡ水平变化可反映胃基础分泌水平和胃黏膜功能及状态,早期胃癌患者常出现局部胃组织坏死,造成胃黏膜功能严重受损,影响胃底腺分泌的PGⅠ、PGⅡ,从而引起血清PGⅠ、PGⅡ水平均显著降低,因此,血清PGⅠ、PGⅡ水平在胃癌预警中具有重要意义[17-18]。本研究结果与其基本一致,证实了血清PGⅠ和PGⅡ水平检测有利于胃癌检出。大量研究证实,CEA作为一种血液肿瘤标记物,主要反映了胃肠道肿瘤,尤其对胃癌最为敏感。胃癌患者血清CEA常呈倍数增长,且肿瘤恶性程度越高,血清CEA数值越高[19]。Hp是胃癌的致癌原,机体感染Hp后可引起胃黏膜细胞发生萎缩肠化,进一步发展为不典型增生,最终发生癌变。流行病学显示,感染Hp是引起胃癌的高危因素,Hp感染率和胃癌发生率一致,在Hp感染患者中,胃癌发生率也增高[20]。本研究中,三组患者Hp阳性率分别为92.39%、85.58%和79.81%,三组患者Hp阳性率比较,差异有统计学意义(P<0.05)。证实了Hp在胃癌患者中具有较高的检出率。
ROC曲线结果显示,PGⅠ、PGⅡ、CEA及Hp预测胃癌发生的曲线下面积分别为0.768、0.721、0.796和0.608,低于PGⅠ、PGⅡ、CEA及Hp联合检测的0.867。说明联合检测对胃癌早期具有较好诊断价值,证实了血清PGⅠ、PGⅡ、CEA及Hp联合检测对胃癌早期患者的诊断效能明显好于慢性胃炎组和胃溃疡组。
综上所述,血清PGⅠ、PGⅡ、CEA及Hp水平与胃癌发生关系密切,可作为胃癌早期的筛查手段,为临床诊治提供依据。
参考文献
[1] Smyth E C,Nilsson M,Grabsch H I,et al.Gastric cancer[J].Lancet,2020,29(10):635-648.
[2] Necula L,Matei L,Dragu D,et al.Recent advances in gastric cancer early diagnosis[J].World Journal Gastroenterology,2019,5(17):2029-2044.
[3] Bergquist J R,Leiting J L,Habermann E B,et al.Early-onset gastric cancer is a distinct disease with worrisome trends and oncogenic features[J].Surgery,2019,166(4):547-555.
[4] Eusebi L H,Telese A,Marasco G,et al.Gastric cancer prevention strategies:A global perspective[J].Journal Gastroenterology Hepatology,2020,35(9):1495-1502.
[5] Wu D,Zhang P,Ma J,et al.Serum biomarker panels for the diagnosis of gastric cancer[J].Cancer Medicine,2019,8(4):1576-1583.
[6] Yao K,Uedo N,Kamada T,et al.Guidelines for endoscopic diagnosis of early gastric cancer[J].Digestive Endoscopy,2020,32(5):663-698.
[7] Suzuki T,Kitagawa Y,Nankinzan R,et al.Early gastric cancer diagnostic ability of ultrathin endoscope loaded with laser light source[J].World Journal Gastroenterology,2019,25(11):1378-1386.
[8] Chiang T H,Chiu S Y,Chen S L,et al.Serum Pepsinogen as a Predictor for Gastric Cancer Death:A 16-Year Community-based Cohort Study[J].Journal Clinical Gastroenterology,2019,53(5):186-193.
[9] Yuan L,Zhao J B,Zhou Y L,et al.Type Ⅰ and type Ⅱ Helicobacter pylori infection status and their impact on gastrin and pepsinogen level in a gastric cancer prevalent area[J].World Journal Gastroenterology,2020,26(25):3673-3685.
[10] Gomes C,Almeida A,Barreira A,et al.Carcinoembryonic antigen carrying SLeX as a new biomarker of more aggressive gastric carcinomas[J].Theranostics,2019,9(24):7431-7446.
[11] Wu J Y,Lee Y C,Graham D Y.The eradication of Helicobacter pylori to prevent gastric cancer a critical appraisal[J].Expert Review of Gastroenterology and Hepatology,2019,13(1):17-24.
[12] Ford A C,Yuan Y,Moayyedi P.Helicobacter pylori eradication therapy to prevent gastric cancer:systematic review and meta-analysis[J].Gut,2020,69(12):2113-2121.
[13]陈光勇,黄受方.WHO消化系统肿瘤分类第5版关于胃癌的解读:着重对早期胃癌的理解和认识[J].中华病理学杂志,2020,49(9):882-885.
[14]朱静怡,翟惠虹,李鹏.慢性萎缩性胃炎的诊断与随访[J].中华内科杂志,2020,59(1):71-74.
[15]马凤梅,谭诗云,程玉,等.内镜超声检查对活检阴性及愈合期恶性胃溃疡的诊断价值[J].中华消化内镜杂志,2019,36(9):702-704.
[16] Eusebi L H,Telese A,Marasco G,et al.Gastric cancer prevention strategies:A global perspective[J].Journal Gastroenterology Hepatology,2020,35(9):1495-1502.
[17] Yu G,Wang G X,Wang H G,et al.The value of detecting pepsinogen and gastrin-17 levels in serum for pre-cancerous lesion screening in gastric cancer[J].Neoplasma,2019,66(4):637-640.
[18] Mansour-Ghanaei F,Joukar F,Baghaee M,et al.Only serum pepsinogen Ⅰ and pepsinogen Ⅰ/Ⅱ ratio are specific and sensitive biomarkers for screening of gastric cancer[J].Biomolecular Concepts,2019,10(1):82-90.
[19]徐風.胃癌患者血清CA199,CEA,CRP和CA72-4检测临床意义[J].中华肿瘤防治杂志,2019,26(1):76,78.
[20]马丹,孟凡冬.幽门螺杆菌感染与胃癌的早期诊治[J].中华内科杂志,2020,59(5):392-394.
(收稿日期:2021-05-24) (本文编辑:张明澜)
猜你喜欢
文萃报·周二版(2020年36期)2020-09-29
康颐(2020年4期)2020-09-10
科学导报·学术(2019年27期)2019-09-10
家庭医学(2017年3期)2017-05-27
中国实用医药(2016年29期)2016-12-26
中国民族民间医药·上半月(2016年11期)2016-12-26
中国现代医生(2016年27期)2016-12-21
家庭用药(2016年9期)2016-12-03
医学信息(2016年29期)2016-11-28
中国现代医生(2016年25期)2016-11-19
