
Morin attenuates L-arginine induced acute pancreatitis in rats by downregulating myeloperoxidase and lipid peroxidation
2021-03-19 01:25KanwalRehmanUmmaraRashidKomalJabeenMuhammadSajidHamidAkash
Kanwal Rehman, Ummara Rashid, Komal Jabeen, Muhammad Sajid Hamid Akash
1Department of Pharmacy, University of Agriculture, Faisalabad, Pakistan
2Institute of Physiology and Pharmacology, University of Agriculture, Faisalabad, Pakistan
3Department of Pharmaceutical Chemistry, Government College University Faisalabad, Pakistan
ABSTRACT
KEYWORDS: Morin; Acute pancreatitis; Diclofenac sodium;L-arginine
1. Introduction
Pancreatitis is an inflammatory condition of the pancreas which may vary from mild to severe stage termed as acute or chronic pancreatitis, respectively. Acute pancreatitis (AP) is a self-limited stage where inflammation can be resolved using simple medical management and can be cured if diagnosed and treated earlier,otherwise, it may lead to chronic pancreatitis or pancreatic fibrosis which ultimately leads to pancreatic cancer that is more difficult to cure[1]. AP has become one of the most common gastrointestinal disorders nowadays which requires hospitalization worldwide[2]. In the United States, approximately 5 000 new cases of pancreatitis are reported every year with a mortality rate of 9% to 20%. Common causes of pancreatitis include gallstones and idiopathic diseases[3,4].Common symptoms associated with AP are abdominal pain, nausea,and vomiting. Patients may have a low-grade fever, hypotension,and tachycardia. Serum concentration of α-amylase may also increase during pancreatitis[5,6]. Progression of AP involves several steps. As the first step, injury is initiated in the acinar cell resulting from many factors like biliary tract obstruction due to untreated gallstones. Further, the acinar cell can initiate the local activation of the immune system and may cause recruitment and activation of macrophages, T-cells, fibroblasts, dendritic cells, and other endothelial cells that start to contribute for inflammation within pancreas. Later, the aggravation of this inflammation may lead to the induction and further progression of AP[7].
The prevalence of AP may lead to systemic illness and can cause systemic inflammatory response syndrome that may progress to multiple organ dysfunction and even death. Inflammatory molecules like cytokines, chemokines, platelet-activating factor, tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6) and interleukin-8 (IL-8)generated during pathogenesis of AP are considered responsible for the development of multiple organ failure[8]. Xanthine oxidase is also involved as a causative factor for the production of reactive oxygen species during AP which causes mild to severe pancreatitis.These free radicals are produced at the early stage of pancreatitis.Cytokines are the most important inflammatory mediators that are found to be present in systematic circulation during AP. IL-6 and TNF-α which are derived from macrophages can be directly associated with progression of pancreatitis and complications in the functioning of other organs. IL-6 levels have been observed to be very high in the case of AP[9]. As far as the experimental induction of AP for study purpose is concerned, previous studies have shown that intraperitoneal administration of a high dose of L-arginine to rats may result in the development of AP[10,11]. L-Arginine also has a role in inducing nitrosative and oxidative stress by producing nitric oxide synthase. These pathways might further contribute to pancreatic injury[12]. Single intraperitoneal injection of L-arginine at a dose (400 mg/100 g body weight) can induce pancreatitis in mice however, in rats, 500 mg/100 g dose of L-arginine has been used to induce pancreatitis. Nevertheless, such a high dose in rats as a single injection has been proved to cause mortality, therefore,divided doses (2×250 mg/l00 g body weight) has been preferred at 1 h interval to induce AP in rats[13]. As for the treatment approaches for AP, multiple strategies like analgesic, steroid therapy, and antiinflammatory agents, have been used to treat pancreatitis. But these synthetic agents are associated with multiple alterations in numerous other physiological effects which may cause various complications.On the other hand, natural agents have also shown the potential to treat many kinds of inflammatory diseases. These natural agents have minimum side effects with maximum therapeutic potential to cure disease and also have the edge of being cost effective[14].
Among natural flavanols, morin has many pharmacological effects such as anti-inflammatory, antioxidant, cardio-effective, and antineoplastic activities. Morin has shown anticancer and antioxidant effects by inhibiting the proliferation of tumor cells including leukemia and colon cancer via suppressing the expression of certain genes[15-17]. Morin has also been reported to improve the pathological condition of glucose intolerance, insulin resistance,and hyperglycemia as well. Antioxidant activity of morin is well known for its effectiveness against free radicals as a scavenger in a variety of diseases. Further, it is a potent anti-inflammatory agent as it has shown its effects by inhibiting the activation of macrophages both in vivo and in vitro[18]. Morin reduces the level of lipid peroxide and is also effective in the reduction of inflammatory cytokine levels. After administration of morin, levels and/or expressions of TNF-α have also been decreased[19]. Morin has protective effects in many pathological conditions that may result in the generation of reactive oxygen species and inflammation. Morin is found to exhibit anti-oxidative and anti-inflammatory activity by stimulating the expression of antioxidant proteins, such as glutathione reductase,glutathione peroxidase, hemeoxygenase-l, superoxide dismutase,and catalase. By this mechanism, morin provokes the upregulation of antioxidant enzyme synthesis and thus controls the various cell signaling pathways[20,21].
To the best of our information, the anti-inflammatory and antioxidative activities of morin against AP remain to be determined.Therefore, the purpose of this study was to evaluate the effect of morin on L-arginine induced AP in rats.
2. Materials and methods
2.1. Induction of pancreatitis
A total number of 20 Wistar albino rats with an average weight of 250-350 g were purchased from the University of Agriculture Faisalabad, Pakistan. They were kept at (25 ± 4) ℃ in an animal house of the University of Agriculture Faisalabad. All the rats were given a standard diet with water ad libitum throughout the study period. The rats were assigned to four groups (n=5). According to the study protocol, for the induction of AP, groups 2-4 received two intraperitoneal injections of L-arginine (250 mg/100 g body weight)at 1 h interval. Group 2 served as pancreatitis control group in which no treatment was given throughout the study period. Groups 3 and 4 were treated with morin (30 mg/kg) and diclofenac sodium (30 mg/kg), respectively, for 30 d.
2.2. Blood sampling and biochemical analysis
For biochemical analysis of predefined biomarkers, about 0.5 mL blood sample was collected from a rat tail vein. The collected blood samples were centrifuged at 3 000 rpm for 20 min and separated serum was stored at —20 ℃ till further biochemical analysis.
2.2.1. Estimation of glycemic biomarkers
To determine the effect of morin treatment on glycemia in experimental AP rats, blood glucose level was measured on the 1st, 7th, 14th, 21st and 28th day, while serum level of insulin was measured on the 1st, 14th and 28th day of the study period.The blood glucose levels were estimated by a glucometer (Accu-Check) and the insulin level was estimated in the serum samples of all experimental groups using insulin ELISA kit (Cat Number:INS5275, Elabscience, USA) and the absorbance was measured at 450 nm using microplate ELISA reader (BI, 800TS-UV, USA).
2.2.2. Determination of insulin sensitivity
Before the end of treatment, we measured the basal blood glucose via a glucometer and serum insulin level via ELISA kit to assess the effect of treatment on insulin sensitivity using homeostasis model assessment (HOMA).
2.2.3. Estimation of carbohydrate digestive enzyme
α-Amylase is an enzyme that helps to breakdown the starch and carbohydrates into sugar molecules. Increased level of this enzyme is usually associated with the occurrence of pancreatitis. To assess the effect of morin treatment on α-amylase activity after the induction of AP, we measured the serum level of α-amylase from the collected blood samples of all experimental rats on the 1st, 14th and 28th day of the study period by using α-amylase ELISA kit (Cat Number:E-EL-R2544, Elabscience, USA) and the absorbance was measured at 450 nm using microplate ELISA reader.
2.2.4. Estimation of lipid peroxidation and inflammatory status
The serum level of malondialdehyde (MDA) and myeloperoxidase(MPO) was measured as biomarkers of lipid peroxidation and neutrophil infiltration at the site of inflammation, respectively. These levels were determined on the 1st, 14th and 28th day of the study period using MDA (Cat Number: E-EL-0060, Elabscience, USA)and MPO (Cat Number: SG-20791, Immuno USA) ELISA kits and the absorbance was measured at 450 nm using microplate ELISA reader.
2.2.5. Estimation of liver function enzymes and cholesterolemia
To evaluate any probable damaging or harmful effects of L-arginine and protective and/or curative effects of morin and diclofenac sodium on hepatocytes after the induction of AP, liver function biomarkers including alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were estimated on the 1st, 14th and 28th day of the study period using their corresponding assay kits (Catalog Number: BD080918, Bioactiva Diagnostics GmbH, Germany for both kits) with the help of Micro Lab chemistry analyzer (MicroLab-300).
Augmented levels of cholesterol in the blood are one of the reasons for dyslipidemia which is known as hypercholesterolemia. To investigate the effect of morin treatment on hypercholesterolemia after the induction of AP, we estimated the serum level of cholesterol on the 1st, 14th and 28th day of the study period using its assay reagent kit (Cat Number: E-BC-K109-S, Elabscience, USA) with the help of Micro Lab chemistry analyzer (MicroLab-300).
2.3. Histopathological analysis
At the end of treatment, rats were killed mercifully and the pancreas was separated for histopathological examination. Sections were separated from isolated pancreas and were fixed in 10% buffered formalin. The fixed tissue was washed and dehydrated in alcohol.Afterwards, the tissue was placed in xylene. The clear tissue was infiltrated with melted paraffin for 2 h and embedded in paraffin wax. Later, tissues were cut into thin slices (5 µm) with a microtome.Sections were mounted directly on the slides. Finally, the mounted sections were stained by hematoxylin and eosin (H & E) stains and covered with glass cover slip. Slides were observed at 10× for histopathological analysis.
2.4. Ethical statement
All experimental procedures were carried out at the University of Agriculture Faisalabad. This study was approved by the Ethics Committee of University of Agriculture, Faisalabad, Pakistan with ethics code No. DGS/4313-16 and performed strictly in accordance with the institutional and international guide for animal care.
2.5. Statistical analysis
The values for all biochemical parameters were presented as mean± SD. The association among various biochemical parameters was investigated by non-linear regression analysis through GraphPad Prism 5. The probability value (P<0.05) was considered statistically significant and two-way ANOVA (analysis of variance) along with Bonferroni post-test was applied for comparison among the groups.For statistical analysis of HOMA-IR, one-way ANOVA followed by Tukey's Multiple Comparison Test was used.
3. Results
3.1. Effect of morin on glycemia and insulin sensitivity
We found that diclofenac sodium-treated AP rats effectively reduced the blood glucose level (P<0.01) as compared to that of AP-induced experimental rats (Figure 1A) and its effect continued and enhanced till the end of the experiment (P<0.001). Similarly, on the 28th day,the morin-treated group showed a highly significant (P<0.001)decline in the blood glucose level as compared to that of AP-induced experimental rats. The effect of treatment on insulin level is shown in Figure 1B. A significant increase in the level of insulin secretion was observed with time in groups that were either treated with morin(P<0.001) or diclofenac sodium (P<0.001) when compared with that of AP rats. On the 14th and 28th day, insulin secretion was improved(P<0.05 and P<0.001, respectively) in morin treated rats compared with the diclofenac sodium-treated group (Figure 1B). Moreover,both diclofenac sodium and morin treatment reduced the insulin resistance as compared to that of AP-induced experimental rats, but morin treatment ameliorated the insulin resistance more significantly(P<0.05) than diclofenac sodium (Figure 1C).
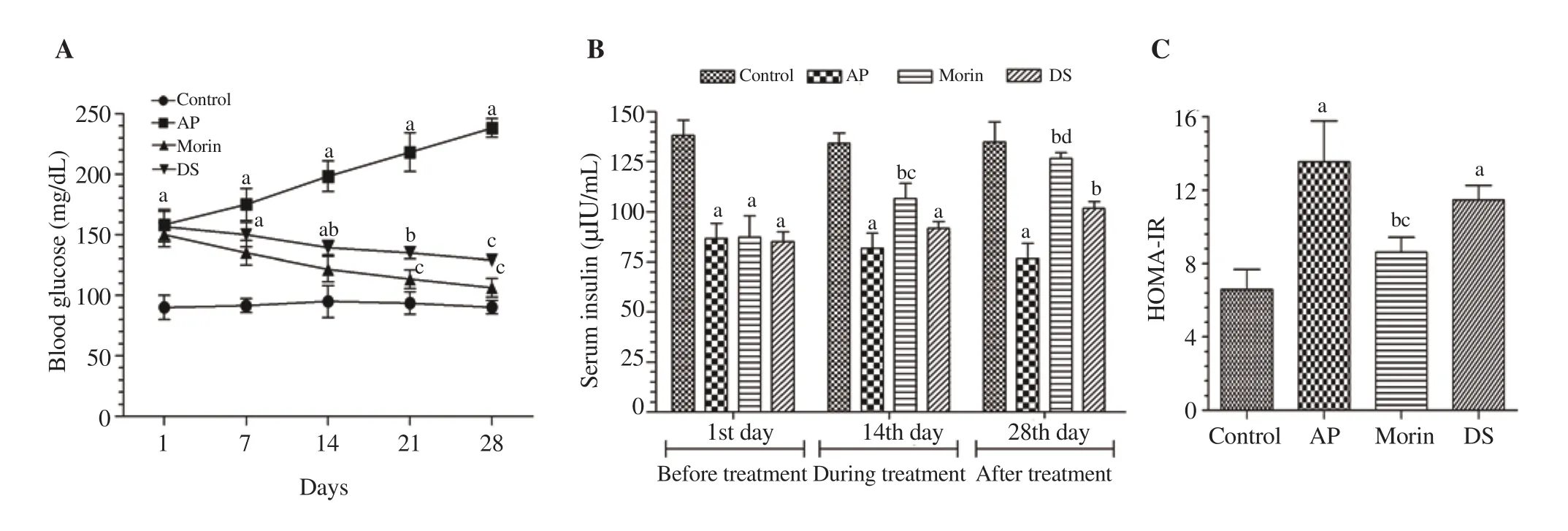
Figure 1. Effect of morin treatment on glycemia. (A) Blood glucose level was measured in all experimental groups on the 1st, 7th, 14th, 21st and 28th day of the treatment. aP<0.001 compared with the normal control group. bP<0.01 compared with the AP group. cP<0.001 compared with the AP group. (B) Serum insulin level was estimated in all experimental groups on the 1st, 14th, and 28th day. aP<0.001 compared with the normal control group. bP<0.001 compared with the AP group. cP<0.05, dP<0.001 compared with the DS group. (C) HOMA-IR was calculated by measuring the fasting levels of glucose and insulin before the end of treatment. The level of significant difference was estimated by Tukey's Multiple Comparison Test using one-way ANOVA. aP<0.001 compared with the normal control group. bP<0.001 compared with the AP group. cP<0.05 compared with the DS group. DS: diclofenac sodium, AP: acute pancreatitis,HOMA-IR: homeostatic model assessment for insulin resistance.
3.2. Effect of morin on carbohydrate digestive enzyme
L-arginine-administered rats showed a higher level (P<0.001) of serum α-amylase than that of the normal control group. However,on the 14th day, morin significantly decreased α-amylase level(P<0.001) compared to that in AP-induced experimental rats. A similar pattern was also observed in diclofenac sodium-treated rats(P<0.01). On the other hand, morin treatment was more effective(P<0.01) in decreasing the serum α-amylase level than diclofenac sodium at the end of the treatment (Figure 2).
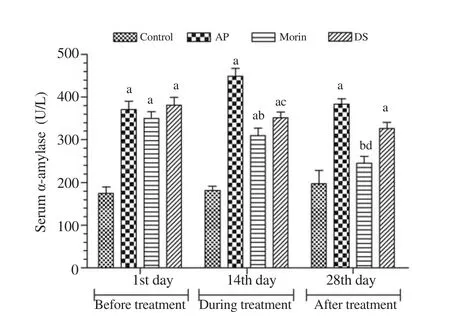
Figure 2. Effect of morin on α-amylase. Serum level of α-amylase was measured on the 1st, 14th, and 28th day. aP<0.001 when compared with the normal control group. bP<0.001, cP<0.01 compared with the AP group.dP<0.01 compared with the DS group.
3.3. Effect of morin on lipid peroxidation and inflammation
To estimate the effect of morin treatment on lipid peroxidation and inflammation, we measured the serum level of MDA and MPO respectively on the 1st, 14th and 28th day (Figure 3). The effect of MDA which is a lipid peroxidation biomarker is shown in Figure 3A. On the 1st day, L-arginine significantly increased the MDA level(P<0.001) and the increase continued till the end of experiment. On the 14th and 28th day of treatment, morin significantly declined the level of MDA (P<0.001) compared to that in AP rats (Figure 3), which was more effective than diclofenac sodium (P<0.05). Similarly, the inhibitory effect of morin on MPO level was also observed (Figure 3B).Before the start of treatment, it was observed that the level of MPO was elevated markedly (P<0.001) compared to that of the normal control group. On the 14th and 28th day, morin inhibited the serum level of MPO with more significant effect compared with diclofenac sodium(Figure 3B).
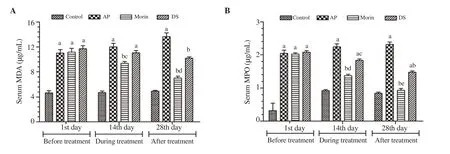
Figure 3. Effect of morin on lipid peroxidation and inflammatory response. (A) Serum level of MDA was measured on the 1st, 14th, and 28th day. aP<0.001 compared with the normal control group. bP<0.001 compared with the AP group. cP<0.05 compared with the DS group. dP<0.001 compared with the DS group.(B) Serum level of MPO was measured on the 1st, 14th, and 28th day. aP<0.001 compared with the normal control group. bP<0.001, cP<0.05 compared with the AP group. dP<0.01, eP<0.001 compared with the DS group. MDA: malondialdehyde, MPO: myeloperoxidase.
3.4. Effect of morin on liver function markers
On the 1st day, the serum level of AST and ALT was increased(P<0.001) in AP rats compared to the normal control group. On the 14th and 28th day, morin declined the serum AST and ALT level(P<0.001) induced by AP. The ameliorative effect of morin on the serum AST and ALT level was comparable to diclofenac sodium(P<0.01) (Figure 4).
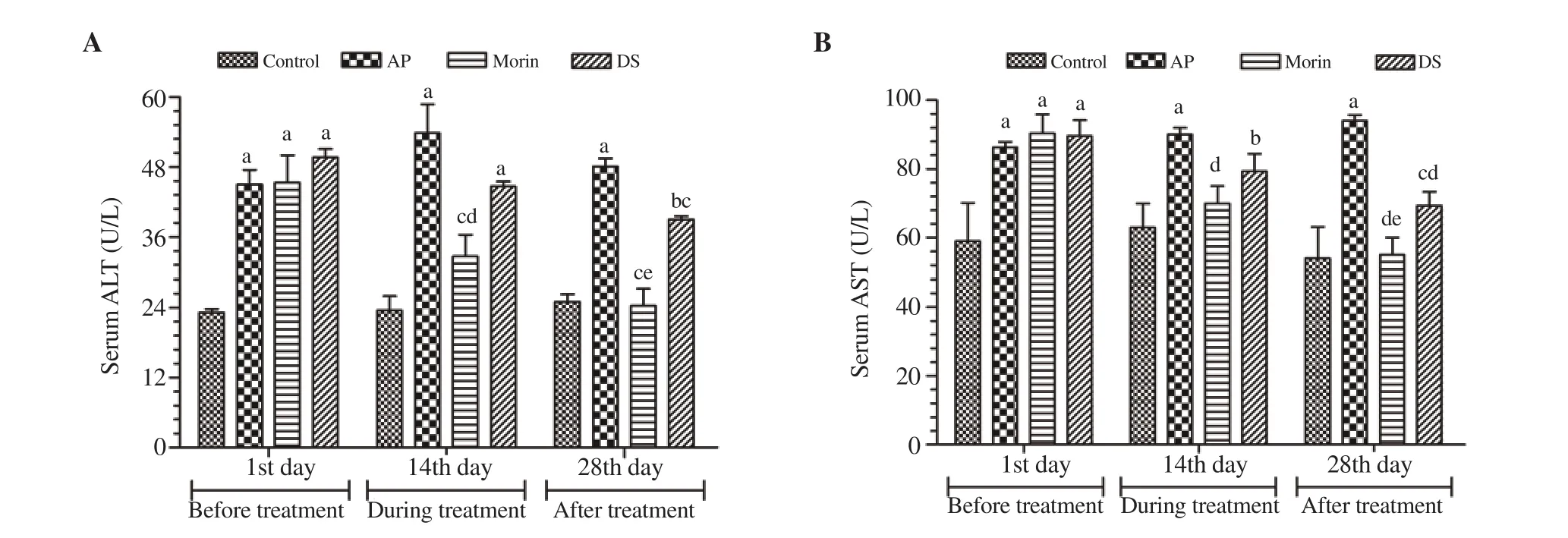
Figure 4. Effect of morin on liver function. (A) Serum level of ALT was measured on the 1st, 14th, and 28th day. aP<0.001, bP<0.01 compared with the normal control group. cP<0.001 compared with the AP group. dP<0.05, eP<0.01 compared with the DS group. (B) Serum level of AST was measured on the 1st, 14th,and 28th. aP<0.001, bP<0.01, and cP<0.05 compared with the normal control group. dP<0.001 compared with the AP group, eP<0.05 compared with the DS group. ALT: alanine aminotransferase, AST: aspartate aminotransferase.
3.5. Effect of morin on hypercholesterolemia
It was observed that before treatment, AP rats exhibited an increased level (P<0.001) of cholesterol compared to that in the normal control group. On the 14th day of treatment, both morin and diclofenac sodium treatments significantly declined the cholesterol level (P<0.05). At the end of treatment, morin-treated rats controlled the serum cholesterol level more significantly (P<0.001) compared to diclofenac sodiumtreated rats (Figure 5).
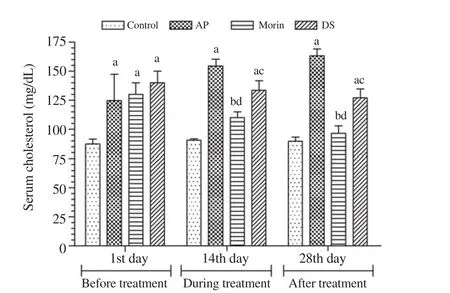
Figure 5. Effect of morin on hypercholesterolemia. Serum level of cholesterol was measured on the 1st, 14th, and 28th day. aP<0.001 compared with the control group. bP<0.001 and cP<0.05 compared with the AP group.dP<0.05 compared with the DS group.
3.6. Histopathology of the pancreas
The normal control rats showed a standard architecture of islets of Langerhans. Furthermore, the acinar cells were well-organized in the normal control group (Figure 6A). Conversely, AP rats showed the damages on pancreatic β-cells (Figure 6B). In addition, treatment with morin and diclofenac sodium showed improved β-cell by restoring the histological architecture of islets of Langerhans (Figure 6C and D).
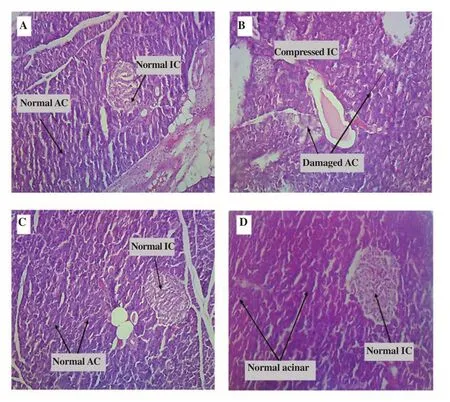
Figure 6. Effect of morin on histology of the pancreas: All slides were observed at 10× for histopathological analysis. (A) The normal control group exhibits the normal appearance of IC and well-distributed AC, while (B) the AP-group shows shrunken IC with damaged AC in the pancreas.However, the treatment with diclofenac sodium(C) or morin (D) shows a pronounced reduction in damaged and inflamed morphology of the pancreas. IC: islet cells, AC: acinar cells, AP: acute pancreatitis.
4. Discussion
AP is a state in which the enzymes produced normally within the glands start to break down the proteins of the pancreas which lead to the abnormal production of antigens in the surrounding tissues of the pancreas. This ends up in starting the cascades of tissuespecific inflammatory responses. Increased inflammation is the result of proinflammatory cytokines, leukocytes, macrophages,and neutrophils that come to the site due to the hyperactivity of inflammatory mediators. Inflammatory mediators attract white blood cells like macrophages and neutrophils at the inflammatory site which further proliferates into other surrounding tissues.Macrophages are the cells that ingest the antigens and other unidentified bodies while neutrophils are attracted by the cytokines produced by macrophages. It has been found that white blood cells produce certain proteolytic enzymes which may lead to the deterioration of surrounding organs known as “the second attack”. If such symptoms are local, it is accompanied by the development of pancreatic necrosis, as it will be occurring in the local pancreatic site or pre-pancreatic area[22].
In the current study, we found that the effect of morin (30 mg/kg)for 30 d had a significant effect against hyperglycemic conditions in AP-induced experimental rats. The morin-treated rats declined blood glucose and improved the serum level of insulin. The most probable mechanism by which morin exerted its hypoglycemic effect might be the potentiating and/or mimetic effect of morin on pancreatic β-cells for insulin secretion as stated elsewhere[23]. This may also stimulate the membrane depolarization through an increase in Cainflux and further activation of insulin-secreting channels may act as a key phase of insulin secretion[24].
In the current work, we also assessed the effect of morin on serum α-amylase level as it is considered as the key enzyme that is altered during the initiation and progression of AP[25]. It was observed that morin was effective in decreasing the elevated serum α-amylase level in L-arginine induced AP rats. This may signify the partly protective role of morin against the progression of AP.
Moreover, specific inflammatory and lipid peroxidation responses in AP-induced experimental animals have also been reported as important biomarkers for the initiation and development of AP and their regulation could be a good way of therapeutic intervention against AP[26,27]. The effect of morin on lipid peroxidation and inflammatory biomarkers was determined by measuring the serum level of MDA and MPO because L-arginine-induced AP was associated with increased levels of MDA and MPO. Morin significantly declined the serum level of MDA and MPO and had better effects than a standard anti-inflammatory agent diclofenac sodium, which was in accordance with previously published reports[17].
Similarly, our study also verified the effect of morin on liver function biomarkers as published earlier[28]. We found that morin not only exhibited the anti-inflammatory and antioxidant effects against AP but also provided multi-organ protection by the same mechanism as detected in the current study through regulation of serum levels of ALT and AST. Moreover, in recent studies, it has also been found that lipid biomarkers may be altered during AP, and dyslipidemia was significantly reversed after the treatment of morin[29,30].Likewise, we found morin significantly declined the cholesterol level and alleviated hypercholesterolemia.
In conclusion, morin alleviates acute pancreatitis via redution of inflammatory responses and oxidative stress. These findings may be helpful for future drug development and therapeutic interventions against pancreatitis.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This work has been financially supported by the research grant(5661/Punjab/NRPU/R&D/HEC/2016, 6429/Punjab/NRPU/R&D/HEC/2016 and 8365/Punjab/NRPU/R&D/HEC/2017) received from Higher Education Commission of Pakistan.
Authors’ contributions
KR and MSHA conceived and designed research. UR and KJ conducted experiments and contributed new reagents. UR and KJ analyzed data. KR and MSHA wrote the manuscript. All authors read and approved the manuscript.
 Asian Pacific Journal of Tropical Biomedicine2021年4期
Asian Pacific Journal of Tropical Biomedicine2021年4期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- Cannabinoid CB2 receptors and spinal microglia are implicated in tingenonemediated antinociception in mice
- Natural compounds as potential inhibitors of SARS-CoV-2 main protease: An insilico study
- Lentinula edodes extract inhibits matrix metalloproteinase expression and increases typeⅠprocollagen expression via the p38 MAPK/c-Fos signaling pathway in ultraviolet A and B-irradiated HaCaT keratinocytes
- Reactive oxygen species and senescence modulatory effects of rice bran extract on 4T1 and NIH-3T3 cells co-treatment with doxorubicin