
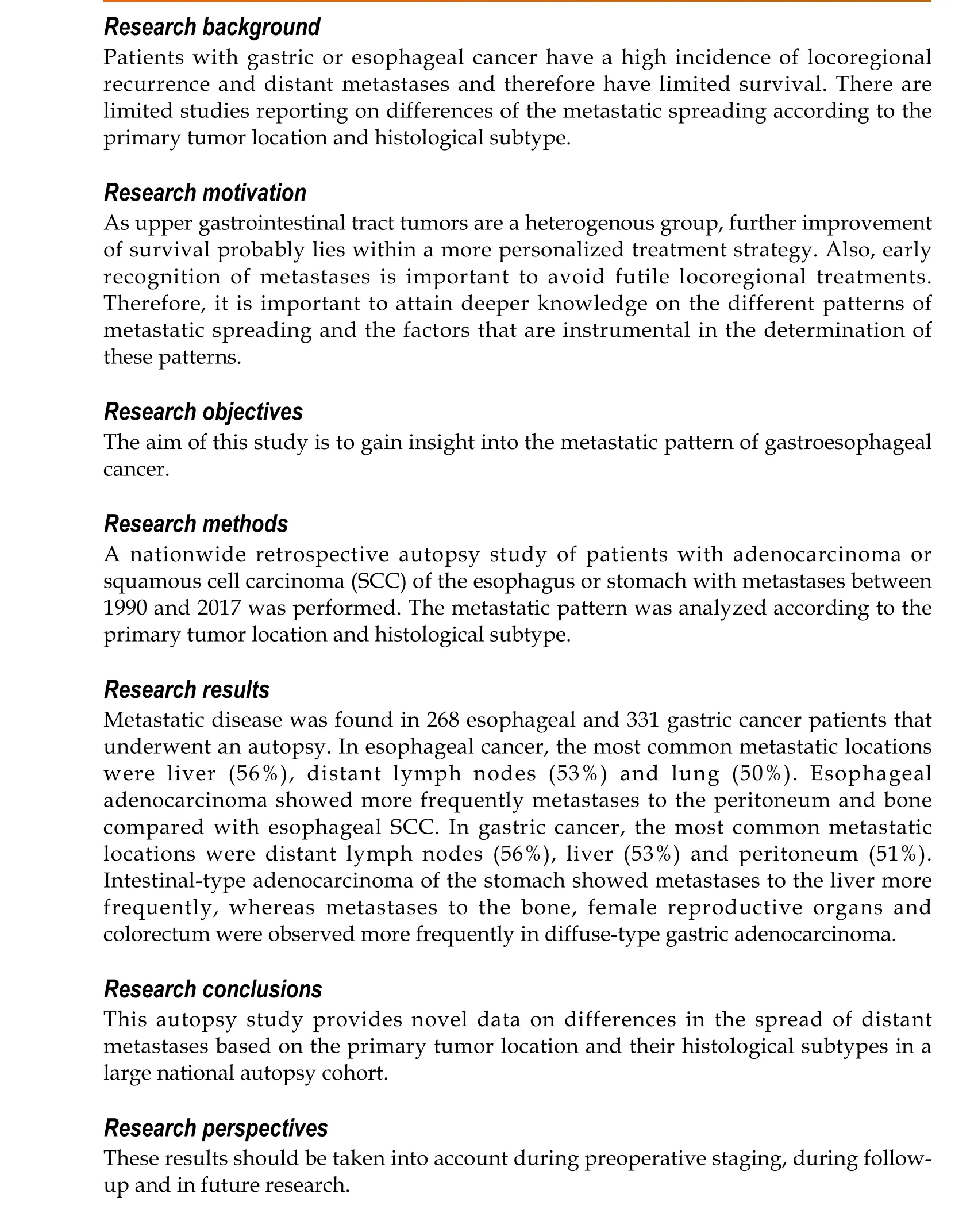
Metastatic pattern in esophageal and gastric cancer: Influenced by site and histology
2020-12-11 07:09:30MoniekHPVerstegenMitchellHarkerCarlijnvandeWaterJolandavanDierenNiekHugenIrisNagtegaalCamielRosmanRachelvanderPost
World Journal of Gastroenterology 2020年39期
Moniek HP Verstegen, Mitchell Harker, Carlijn van de Water, Jolanda van Dieren, Niek Hugen, Iris D Nagtegaal, Camiel Rosman, Rachel S van der Post
Abstract
Key Words: Esophageal cancer; Gastric cancer; Metastases; Histology; Gastroesophageal junction; Adenocarcinoma; Carcinoma; Squamous cell
INTRODUCTION
In 2018, over 570000 esophageal cancer and over 1000000 gastric cancer cases occurred globally, respectively the 6thand 3rdleading cause of cancer related death[1,2]. Over the last decade, peri-operative treatment modalities for patients with potentially curable esophageal or gastric cancer have improved. In the Netherlands, most patients with locally advanced esophageal cancer are treated with neo-adjuvant chemoradiotherapy, followed by resection[3]. Patients with potentially curable gastric cancer are treated with peri-operative chemotherapy and resection[4,5]. Despite the fact that these treatment modalities resulted in improved overall survival, the prognosis of patients with gastric or esophageal cancer is still dismal mainly due to the high incidence of locoregional recurrence and distant metastases. Moreover, up to 50% of gastroesophageal cancer patients present with metastatic disease at time of diagnosis[6,7]. Early recognition of metastases is important to avoid futile locoregional treatments. There is a wide variability in the timing, location and extent of metastatic disease. In order to optimize pretreatment evaluation of patients and to ensure adequate surveillance, it is essential to know more about the metastatic pattern occurring in this patient group.
Metastases of esophageal cancer are most frequently seen in the liver, lung and distant lymph nodes[8-10]. The most common metastatic sites of gastric cancer are the liver, peritoneum and distant lymph nodes[11,12]. There are limited studies reporting on differences of the metastatic spreading according to the primary tumor location, for example, upper esophagealvsdistal esophageal cancer or cardiavsnon-cardia gastric cancer[9,12]. Few studies reported data on differences in metastatic site according to histological subtype[8,9,11,12].
As upper gastrointestinal tract tumors are a heterogenous group, further improvement of survival probably lies within a more personalized treatment strategy. Therefore, it is important to attain deeper knowledge on the different patterns of metastatic spreading and the factors that are instrumental in the determination of these patterns. The aim of this study is to gain insight into the location of metastases and the metastatic pattern according to the primary tumor site and the histology of the primary tumor.
MATERIALS AND METHODS
Study design
A nationwide retrospective review was conducted of pathological records of patients diagnosed with esophageal or gastric cancer who underwent autopsy between 1990 and 2017. Patients were selected from the nationwide network and registry of histopathology and cytopathology in the Netherlands (PALGA)[13]. In the Netherlands, post-mortem examination is performed at the request of the family or treating physician with consent of the family and is carried out by a pathologist. All autopsies included in this study were performed in order to obtain information on the medical status of the deceased or to determine the exact cause of death. This type of study does not require approval from an ethics committee under Dutch law.
Inclusion and exclusion criteria
Patients with a history of esophageal or gastric cancer who underwent autopsy were selected from the Dutch pathology registry (PALGA). Only patients with a history of esophageal or gastric cancer with metastases, or those who were diagnosed with metastatic esophageal or gastric cancer during autopsy, were included. Patients with a primary diagnosis of a premalignant lesion, (i.e.dysplasia and in-situ carcinoma), neuroendocrine neoplasm, mesenchymal tumor, lymphoma or metastases from elsewhere to the esophagus or stomach were excluded. Incomplete autopsies were excluded. Patients were excluded if the location of the metastases could not be retrieved from the records.
Study characteristics and outcome parameters
Gender, date of autopsy, age at autopsy, type of autopsy (body or body and brain), location of primary cancer (proximal esophagus, mid esophagus, distal esophagus [incl. gastro-esophageal junction (GEJ)], proximal stomach (i.e.cardia and fundus), stomach corpus, distal stomach (i.e.antrum, pylorus and linitis plastica), number of metastases and location of metastases were recorded. The histological type of carcinoma was recorded according to the World Health Organization and Laurén classification. In case of adenocarcinoma not otherwise specified, the carcinoma was assigned to the intestinal-type adenocarcinoma group. In case of metastases to the abdominal organs, records where thoroughly screened whether it was a peritoneal metastasis rather than an organ specific metastasis.
Statistical analysis
Statistical analyses were performed with the statistical software package IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, United States). For dichotomous data, frequencies are presented. Continuous data are presented as mean and range. Values are compared by the chi2-squared test. All tests of significance were two-tailed:Pvalues of < 0.05 were considered to be significant.
RESULTS
A total of 3876 autopsy records were initially retrieved in this study: Esophageal cancer was diagnosed in 1686 cases, gastric cancer in 2190 cases. We excluded 3277 patients from further analysis, since they did not have metastatic disease (n= 2919), tumor type was not specified (n= 7) or patients did not have a primary gastroesophageal carcinoma (n= 351). The remaining 599 patients were included in our analysis; 268 (45%) patients had primary esophageal and 331 (55%) gastric carcinoma. Two hundred four patients (34.1%) underwent a resection. The mean age of patients at diagnosis was 66 years (range 25-94 years) and age of patients at death was 67 years (range 25-94 years). In only 28 (5%) cases the neurocranium was examined. The mean number of metastatic locations per patient was 3 (SD 1.86) and 21% of the patients had only one metastasis at the time of death.
Of the 268 esophageal cancer patients with metastatic disease, 62% had AC (167 cases) and 38% SCC (101 cases). AC was subdivided into intestinal-type (144 cases, 86%) and diffuse-type AC (23 cases, 14%). The 331 gastric adenocarcinoma patients were categorized as diffuse-type (including signet-ring cell carcinoma) in 37% (122 cases) or intestinal-type AC in 63% (209 cases). Clinicopathological data of metastatic esophageal and gastric cancer patients are presented in Table 1.
Pattern of metastases in 268 esophageal cancer patients
Of the 268 esophageal cancer patients, 54.5% had multiple (3 or more) metastases, 23.9% had 2 metastases and 21.6% had only one metastasis. Overall, esophageal cancer patients presented most frequently with liver, distant lymph node and lung metastases (56.0%, 52.6%, and 50.0% respectively) (Figure 1). Metastases to the liver were most common in AC (59.9%), whereas metastases to the lungs were most frequently seen in SCC (57.4%). There were three major differences in metastatic pattern between histological subtypes (Figure 2A and B). AC more frequently had metastases to the peritoneum and bone compared with SCC, 34.7%vs15.8% (P< 0.01) and 29.9%vs17.8% (P< 0.05), respectively. Lung metastases were observed more frequently in SCC (57.4%) compared with AC (45.5%,P= 0.059). Patients with a single metastatic location predominantly seem to have a liver metastasis in AC and a liver or lung metastasis in SCC esophageal cancer (Figure 2A and B).
由图3可知,1.064 μm在平流雾中的前向散射最强.由表1和表2可知,1.064 μm在平流雾中的散射系数(4.3296 km-1)大于在辐射雾中的散射系数(3.612 3 km-1).说明1.064 μm在平流雾中前向散射大、散射能力强,多次散射对透过率的贡献较大,所以相同传输距离下,1.064 μm在平流雾中的衰减小于在辐射雾中的衰减.
Pattern of metastases in 331 gastric cancer patients
Of the gastric cancer patients, 54.1% had multiple (3 or more) metastases, 26.3% had 2 metastases and 19.6% had only one metastasis. Overall, gastric cancer patients presented most frequently with distant lymph node, liver and peritoneal metastases (55.9%, 52.9%, and 51.4% respectively) (Figure 3). Intestinal-type AC showed predominantly metastases to the liver (67.5%), whereas diffuse-type AC more likely present with metastases to the peritoneum (57.4%). Significant differences were found in the occurrence of metastases to the liver (67.5% in intestinal-typevs27.9% in diffusetype,P< 0.0001), bone (15.3% in intestinal-typevs29.5% in diffuse-type,P< 0.01), female reproductive organs (5.7% in intestinal-typevs16.4% in diffuse-type,P< 0.01) and colorectum (1.0% in intestinal-typevs5.7% in diffuse-type,P< 0.05). In diffusetype gastric cancer, patients with metastases to the female productive organs often were simultaneously diagnosed with metastases to the peritoneal cavity (Figure 2C and D).
Pattern of metastases according to primary tumor location
Esophagealvsgastric carcinomas: For both esophageal (including GEJ) and gastric cancer (all histological types), the liver was the most frequent metastatic site (56.0% and 52.9%, respectively). Esophageal cancer was more likely to show metastases to the lung (50.0%vs35.3%,P< 0.0001) and heart (13.4%vs7.0%,P< 0.01). Metastases to the peritoneum (e.g.peritoneum, mesentery, omentum, abdominal cavity not further specified) (27.6%vs51.4%,P< 0.0001), female reproductive organs (1.1%vs9.7%,P< 0.0001) and the urinary bladder (0.4%vs2.4%,P< 0.05) were seen more often in gastric cancer.
Proximal and mid esophageal carcinomasvsdistal esophageal and GEJ carcinomas: A sub-analysis for the metastatic site of proximal and midvsdistal esophageal cancer (including GEJ carcinoma) was impeded due to the small number of upper esophageal carcinomas (n= 25). Upper esophageal carcinomas tend to show metastases to the spleen more often (3 out of 25 patients (12%)vs2 out of 174 patients (1.1%),P< 0.01), while distal esophageal carcinomas more often showed metastases to the peritoneum (3 out of 25 patients (12%)vs57vs174 patients (32.8%),P< 0.05).
Distal esophageal, GEJ and cardia carcinomas: Comparing distal esophageal, GEJ and cardia adenocarcinomas (intestinal- and diffuse-type)vsnon-cardia gastric adenocarcinomas showed differences in the metastatic pattern. Metastases to the peritoneum and female reproductive organs were seen more frequently in non-cardia gastric cancer (56.3%vs37.6%,P< 0.001 and 12.2%vs2.1%,P< 0.001, respectively). Distal esophageal, GEJ and cardia carcinomas more often showed metastases to the liver (61.5%vs47.2%,P< 0.05), pleura (27.8%vs17.9%,P< 0.05) and heart (12.0%vs6.1%,P< 0.05) compared with non-cardia gastric carcinomas. Lung metastases were more frequently found when comparing only distal esophageal and GEJ carcinomas with cardia adenocarcinomas (49.2%vs36.2%,P< 0.05).

Table 1 Clinicopathological data of esophageal and gastric cancer patients with metastatic disease

Figure 1 Metastatic sites of patients with esophageal cancer. Other metastases of esophageal cancer (all types) with proportion ≥ 2%: pancreas (6%), brain (4%), mediastinum (3%), skin/subcutis (3%), thyroid gland (3%), spleen (3%), gallbladder (2%). AC: Adenocarcinoma; SSC: Squamous cell carcinoma.
DISCUSSION
This nationwide autopsy study provides insight into the metastatic patterns in patients with esophageal or gastric cancer (n= 599). The two most common metastatic sites for esophageal and gastric cancer are liver and distant lymph nodes. Lung metastases are more frequently observed in patients with esophageal cancer while peritoneal metastases are more common in gastric cancer patients. Furthermore, differences in metastatic pattern according to primary tumor location and histological subtype were observed.

Figure 2 Metastatic pattern of esophageal and gastric cancer by histological subtype. AC: Adenocarcinoma; SSC: Squamous cell carcinoma.

Figure 3 Metastatic sites of patients with gastric cancer. Other metastases of gastric cancer (all types) with proportion ≥ 2%: heart (7%), kidney (6%), pancreas (5%), thyroid gland (4%), brain (3%), large intestine (3%), small intestine (2%), mediastinum (2%), skin/subcutis (2%), urine bladder (2%). AC: Adenocarcinoma.
Overall, the most common metastatic sites of esophageal and gastric cancer found in this study are comparable to the literature[8-12]. Metastases to the liver are frequently observed in both esophageal and gastric cancer. The venous drainage of the distal esophagus is partly provided by the left gastric vein and by the gastroepiploic veins for the stomach which both drain directly into the portal vein. This may explain a high frequency of liver metastases in both groups. The other part of the venous drainage of the distal esophagus, as well as the mid and proximal part of the esophagus, is provided by the azygos vein which directly drains to the superior vena cava which probably explains the high frequency of lung metastases[14]. In addition to anatomical factors which promote specific spreading, organ specific tropism of circulating tumor cells as suggested by the seed and soil hypothesis[15]may also account for frequent metastases to the liver and lung. In esophageal and gastric cancer patients with metastatic disease, we surprisingly also observed frequent metastases in the adrenal gland (27% and 23%), heart (13% and 7%) and kidney (10% and 7%). In literature, metastases to the adrenal gland, heart and kidney are sparsely described. This can probably be explained by the fact that our study is based on autopsy cases, and these distant metastases might be later occurrences, that are also part of a more widespread disease[9,16-18]. Major differences in metastatic sites between histological subtypes were found. While esophageal AC had a predilection for peritoneal and bone metastases, SCC more often spread to the lungs, as is in line with previous findings[8,9]. Underlying mechanisms for differences in metastatic patterns between histological esophageal cancer subtypes are not clear, although the tumor location can be a confounding factor as ACs are generally located in the distal esophagus and SCC generally represent the more proximal tumors. For gastric intestinal adenocarcinoma, more metastases were found in the liver while diffuse-type gastric cancer spreads more often to bone, colorectum, peritoneum and female reproductive organs. The preference of signet-ring cell carcinoma for metastases to the female reproductive organs and peritoneum has been described before in colorectal cancer and may be organ specific tropism of circulating signet-ring cells[19]. Furthermore, previous research reported on the affinity of diffuse-type gastric cancer for peritoneal seeding[12,20]. However, subclassifying of adenocarcinomas into intestinal- and diffuse-type cancers may vary between pathologists since the subclassification of these carcinomas was ill-defined until very recently[21].
今天,寻找到杰出的圣多班已不再是一件难事了,随着勃艮第白葡萄酒越来越受到爱好者的关注,这个小小的村庄也发生了翻天覆地的变化。新生代的酒农们尤其看重葡萄园的打理,只为能够更好地反映出圣多班得天独厚的风土条件。现在的我也解开了10多年前的困惑,那块叫“一堆狗牙齿”葡萄园其实封存了圣多班村最杰出的风土。它地势陡峭,坡面向东,贫瘠的土壤中布满了无数小巧的菱形石灰石。在太阳的反射下,这些洁白的碎石好似退化了的犬类动物门齿,仿佛在某种层面上提醒着我们这片土地的古老历史和深邃潜力。
This study has limitations due to the retrospective nature of the study. Post-mortem studies offer a unique opportunity to examine the extent and location of metastases and can been seen as the gold standard in the study of cancer metastatic pattern. An autopsy study can lead to a biased population in which patients are included who have died postoperatively, had an unexpected clinical course, or died of other causes than esophageal or gastric cancer. However, previous studies confirmed the validity of data from autopsy studies in other cancer types where independent clinical trial and population-based cohorts showed identical patterns[19,22], illustrating that the bias is indeed limited. Unfortunately, the PALGA database does not include a broad spectrum of patient characteristics regarding, for example, comorbidities and demographics and therefore the exact external validity of this study is unclear. Another limitation is the problem of classifying cardia cancers, since the cardia is an ill-defined region of the stomach[23]. This may explain the differences in the metastatic pattern of proximal stomach (cardia) carcinomas in our cohort compared to literature[12].
Over the last decades, considerable improvements of diagnostic techniques in preoperative staging have been made[24]. Still, early recognition of metastases is necessary to avoid futile locoregional treatments. For example, diffuse-type gastric cancer has the tendency to spread to the peritoneal cavity, and therefore a diagnostic laparoscopy for the detection of peritoneal metastases is now common practice in the staging of gastric cancer[25]. Interestingly, this study shows that peritoneal metastases are also frequently observed in patients with metastatic distal esophageal and GEJ AC (38%). Few clinical studies do show the added value of a diagnostic laparoscopy for occult metastatic disease in distal esophageal and GEJ adenocarcinoma patients, whilst other studies report a relatively low rate of positive findings for routine laparoscopy in these patients. Further clinical studies are warranted to investigate if a pre-treatment diagnostic laparoscopy could also be of value for these patients[26,27]. Furthermore, knowledge of the preference location of metastases may help to develop individualized treatment strategies in case of metastatic disease such as Selective liver Internal Radiation therapy (SIRT) for liver metastases or adjuvant pressurized intraperitoneal aerosol chemotherapy or hyperthermic intraperitoneal chemotherapy for peritoneal metastases[28].
CONCLUSION
In conclusion, this autopsy study shows differences in the spread of distant metastases based on the primary tumor location and their histological subtypes in a large national cohort. These results should be taken into account during preoperative staging, during follow-up and in future research.
ARTICLE HIGHLIGHTS
猜你喜欢
青岛画报(2024年5期)2024-07-06 01:24:34
中国地市报人(2019年7期)2019-08-15 07:16:06
大众汽车(2018年11期)2018-12-26 08:44:18
东方企业家(2018年8期)2018-08-22 05:44:08
成都信息工程大学学报(2015年3期)2015-12-02 02:28:24
葡萄酒(2015年8期)2015-05-30 10:48:04
人生与伴侣·共同关注(2015年2期)2015-05-30 09:43:56
液晶与显示(2015年3期)2015-05-10 01:46:06
中学生天地(B版)(2015年4期)2015-05-08 08:11:33
女友·花园(2014年11期)2014-11-17 23:50:44
 World Journal of Gastroenterology2020年39期
World Journal of Gastroenterology2020年39期
- World Journal of Gastroenterology的其它文章
- Herbal cake-partitioned moxibustion inhibits colonic autophagy in Crohn’s disease via signaling involving distinct classes of phosphatidylinositol 3-kinases
- Identification of differentially expressed genes in ulcerative colitis and verification in a colitis mouse model by bioinformatics analyses
- Artificial intelligence technique in detection of early esophageal cancer
- Polyethylene glycol 35 ameliorates pancreatic inflammatory response in cerulein-induced acute pancreatitis in rats
- Impact of cap-assisted colonoscopy during transendoscopic enteral tubing: A randomized controlled trial
- Single access laparoscopic total colectomy for severe refractory ulcerative colitis