
肿瘤坏死因子-α基因多态性与首发抑郁症及舍曲林疗效的关联研究
2020-11-06 07:22刘玉芝寇海燕
中国当代医药 2020年26期
刘玉芝 寇海燕


[摘要]目的 探討肿瘤坏死因子-α(TNF-α)基因多态性与首发抑郁症及舍曲林疗效之间的相关性。方法 选取2011年6月~2018年6月于滨州市优抚医院住院及门诊就诊的265例首发抑郁症患者作为病例组,另选取同期380名滨州市及周围市县的健康献血者作为对照组。采用聚合酶链反应-限制性片段长度多态性分析方法检测首发抑郁症患者、健康对照者各个多态性位点的基因型。采用SHEsis在线软件对TNF-α -G238A(rs361525)、-G308A(rs1800629)、-C857T(rs1799724)、-C863A(rs1800630)进行统计学分析。265例首发抑郁症患者使用舍曲林治疗8周后,以汉密尔顿抑郁量表(HAMD)评定疗效。结果 病例组与对照组的rs1800629在基因型和等位基因频率分布比较,差异均有统计学意义(P<0.05),Bonferroni校正后,基因型频率分布比较差异仍有统计学意义(P<0.05)。而病例组与对照组的rs361525、rs1800630、rs1799724在基因型和等位基因频率分布比较,差异均无统计学意义(P>0.05)。病例组和对照组的单倍型频率分布比较,差异无统计学意义(P>0.05)。舍曲林治疗8周后,采用χ2检验分析首发抑郁症患者TNF-α基因4个SNPS多态性位点的等位基因和基因型频率分布与舍曲林疗效的关系,结果显示,有效组与无效组的rs1800629在基因型频率分布比较,差异无统计学意义(P>0.05),而等位基因频率分布比较,差异有统计学意义(P<0.05);Bonferroni校正后,等位基因频率分布比较,差异无统计学意义(P>0.05)。有效组与无效组的rs361525在基因型和等位基因频率分布比较,差异均有统计学意义(P<0.05);Bonferroni校正后,rs361525在基因型和等位基因频率分布比较,差异均有统计学意义(P<0.01)。有效组与无效组的rs1800630、rs1799724在基因型和等位基因频率分布比较,差异均无统计学意义(P>0.05)。有效组和无效组的单倍型频率分布比较,差异均无统计学意义(P>0.05)。结论 TNF-α基因rs1800629多态性可能与首发抑郁症的易感性有关,rs361525多态性可能与舍曲林的疗效有关。
[关键词]首发抑郁症;肿瘤坏死因子-α;舍曲林;单核苷酸多态性
[中图分类号] R749 [文献标识码] A [文章编号] 1674-4721(2020)9(b)-0017-07
Research of tumor necrosis factor-α gene polymorphisms associated with first-episode depression and the efficacy of Sertraline
LIU Yu-zhi KOU Hai-yan
Department of Psychiatry, Binzhou Youfu Hospital, Shandong Province, Binzhou 256612, China
[Abstract] Objective To investigate the association between tumor necrosis factor-α (TNF-α) gene polymorphism with first-episode depression and efficacy of Sertraline. Methods A total of 265 inpatients and out-patients with first-episode depression diagnosed and treated in Binzhou Youfu Hospital from June 2011 to June 2018 were selected as the case group. In addition, 380 healthy blood donors from Binzhou City and surrounding counties were selected as the control group. Each genotype polymorphism loci of patients with first-episode depression and healthy subjects was analyzed by the polymerase chain reaction-restriction fragment length polymorphism. SHEsis online software was used to analyze the differences in genotype distribution and allele distribution of TNF-α -G238A (rs361525)、-G308A (rs 1800629)、-C857T (rs1799724)、-C863A (rs1800630). Curative effect of 265 patients with first-episode depression treated with Sertraline after eight weeks was evaluated with Hamilton rating scale for depression (HAMD). Results Significant difference was shown in frequency distribution of genotypes and alleles of TNF-α gene rs1800629 between case group and control group (P<0.05); after Bonferroni correction, difference in frequency distribution of genotype was still significant (P<0.05). There was no significant difference in the frequency distribution of genotypes and alleles of rs361525 and rs1799724, rs1800630 between two groups (P>0.05). There was no significant difference in frequency of haploid type between case group and control group (P>0.05). After 8 weeks of Sertraline treatment, the chi-square test was used to analyze the relationship between the frequency distribution of alleles and genotypes of the 4 SNPS polymorphisms of TNF-α gene and the efficacy of Sertraline in patients with first-episode depression, the results showed that there was no significant difference in frequency distribution of genotype in rs1800629 between effective group and ineffective group (P>0.05); significant difference was shown in frequency distribution of allele in rs1800629 between two groups (P<0.05). After Bonferroni correction, no significant difference was shown in frequency distribution of allele in rs1800629 between effective group and ineffective group (P>0.05). Significant difference was shown in frequency distribution of genotypes and alleles of TNF-α gene rs361525 between effective group and ineffective group (P<0.05), after Bonferroni correction, difference in frequency distribution of genotypes and alleles in rs361525 was still significant (P<0.01). There was no statistically significant difference in genotype and allele frequency distribution of rs1800630 and rs1799724 between the effective group and the ineffective group (P>0.05). There was no significant difference in frequency of haploid type between effective group and ineffective group (P>0.05). Conclusion TNF-α gene rs1800629 polymorphism may be associated with the susceptibility of first-episode depression, rs361525 polymorphism may be associated with the efficacy of Sertraline.
[Key words] First-episode depression; Tumor necrosis factor-α; Sertraline; Single-nucleotide polymorphism
抑郁症是一种常见的、危害极大的慢性精神疾病,至今抑郁症的具体病因及发病机制尚不明确。一些研究发现免疫系统与抑郁症发病有关[1-2],抑郁症患者普遍存在免疫激活[3-4]。肿瘤坏死因子-α(TNF-α)作为一种重要的促炎症细胞因子,与免疫激活密切相关,直接和间接参与炎症过程。研究发现,抑郁症患者血清TNF-α浓度异常[5-6],但研究结果有差异[7-8]。差异不仅有外在原因,遗传因素也不容忽视[9]。人的TNF-α基因长约2.76 kb,定位于第6对染色体(6p21.1-21.3)HLAш区。也有研究发现TNF-α基因启动区的基因多态性影响TNF-α基因表达[10]。TNF-α基因-238位点在启动子区与DNA-结合蛋白相结合的调节盒内,该位点等位基因的多态性影响启动子的活性[11]。-857和-863位点在十聚体蛋白(OCTl)和核因子(NF-κB)的结合序列中,SNP影响转录效率[12]。TNF-α的表达受相关基因多态性的调控,-308G/A作为TNF-α基因第一内含子,与TNF-α转录水平调节相关[13]。国内外就TNF-α基因多态性与抑郁症的相关性进行了相关研究,研究结果不尽一致[14-15]。关于TNF-α基因多态性与抗抑郁药物的研究则更是鲜有报道。本研究选取以上4个影响TNF-α表达的位点,旨在进一步明确TNF-α基因多态性在抑郁症发病机制中的潜在作用,在临床领域探讨TNF-α基因多态性和抗抑郁症药物的关联,现报道如下。
1资料与方法
1.1一般资料
选取2011年6月~2018年6月于滨州市优抚医院住院及门诊就诊的265例首发抑郁症患者作为病例组。纳入标准:汉族,年龄18~60岁;均符合国际疾病分类第10次修订本(International Statistical Classification of Diseases and Related Health Problems,10th Revision,ICD-10)[16]抑郁症诊断标准,汉密尔顿抑郁量表(Hamilton rating scale for depression,HAMD)17项评分≥18分;初次发病的抑郁症患者。排除标准:酒精成瘾及药物滥用者;患有双相情感障碍等常见精神疾病;罹患严重躯体疾病者,实验室检查(肝功、血常规、肾功等)和心电图明显异常者;妊娠、哺乳妇女及月经期女性;半年内服用过免疫抑制剂及免疫增强剂,半月内服用过精神药物或解热镇痛药者;半月内有急性感染、创伤、炎症、发 热、过敏者;半月内有接受过电抽搐治疗、睡眠剥夺治疗者。另选取同期380名滨州市及周围市县的健康献血者作为对照组。排除标准:①有重大躯体疾病、内分泌疾病;②有各种免疫性感染性疾病;③有精神疾病或精神疾病家族史;④有药物过敏史,药物和酒精滥用者。病例组中,男137例,女128例;年龄21~53岁,平均(37.3±6.5)岁;病程(7.6±3.5)年。对照组中,男221名,女159名;年龄22~57岁,平均(41.1±5.3)岁。两组的性别、年龄等一般资料比较,差异无统计学意义(P>0.05),具有可比性。本研究获得我院医学伦理委员会同意,全部参加者均签署了知情同意书。
1.2方法
1.2.1临床治疗 采用临床自然入组法,病例组入组后给予舍曲林片(浙江华海药业股份有限公司,国药准字 H20080141,产品批号:023B19009)单一药物治疗,观察8周。舍曲林起始剂量为25 mg/d,最大剂量150~200 mg/d,根据个体治疗反应于2周内达到100 mg/d或患者出现症状改善的剂量。不合并使用其他抗抑郁药物;可使用苯二氮?类药物,但不得连续使用超过7 d。
1.2.2血标本采集及基因分型 取病例组及对照组所有研究对象外周血10 ml(EDTA抗凝),按常规酚-氯仿法抽提研究对象外周血白细胞DNA。采用聚合酶链式反应-限制性片段长度多态性(PCR-RFLP)扩增DNA目的片段。
PCR扩增采用10 μl反应体系:基因组DNA 2 μl,2×PCR缓冲液5 μl,15 mmol/L MgCl2 20.5 μl,上下游引物各0.25 μl,Tag酶0.5 μl(北京天根)。采用PCR-RFLP技術检测TNF-α 4个位点[-G238A(rs361525)、-G308A(rs1800629)、-C857T(rs1799724)、-C863A(rs1800630)]。TNF-α基因-308G/A、-857C/T和-1031T/C位点的引物均参照文献[17]。所有位点的引物、产物长度、PCR反应退火温度和酶切片段见表1。
PCR反应条件:95℃预变性5 min;30个循环(95℃变性30 s,一定的退火温度35 s,72℃延伸40 s);72℃延伸10 min,最后4℃保存。
5 μl酶切反应体系:PCR产物3 μl,限制性内切酶5 U,后加无菌双蒸水补齐。37℃温育过夜,酶切产物用3.0%琼脂糖凝胶(含溴化乙锭)电泳分离,经凝胶成像仪系统处理后进行基因型判读。随机抽取30例样本使用基因测序法对结果进行验证,一致率达98.5%以上。
1.3评价标准
两名评分者不参与实验设计。对评分者进行统一量表培训及一致性检验,Kappa值为0.96。分别于治疗前及治疗第8周末采用HAMD评估。疗效评定标准以HAMD总分减分率判定临床疗效,分为痊愈、显著进步、进步和无效。痊愈:减分率≥75%,显著进步:75%>减分率≥50%,进步:50%>减分率≥25%,无效:减分率<25%。总有效=痊愈+显著进步+进步[18]。
1.4统计学方法
采用SPSS 17.0统计软件进行分析,计量资料用均数±标准差(x±s)表示,两组间比较采用t检验;计数资料采用率表示,组间比较采用χ2检验。采用SHEsis[19]在线软件(http://analysis.Bio-x.cn/myAnalysis.php)进行等位基因、基因型频率分布、Hardy-Weinberg平衡及单倍型的关联分析。所有项目检测均为双侧检验,统计学显著性水平设为双侧P<0.05。采用Bonferroni多重检验校正。
2结果
2.1 Hardy-Weinberg遗传平衡度检验
经χ2检验,rs1800629(病例组:χ2=3.08,P=0.08;对照组:χ2=0.83,P=0.36)、rs361525(病例组:χ2=1.99,P=0.16;对照组:χ2=1.11,P=0.29)、rs1800630(病例组:χ2=1.65,P=0.20;对照组:χ2=2.25,P=0.13)、rs1799724(病例组:χ2=3.30,P=0.07;对照组:χ2=2.39,P=0.12)4个SNP位点基因型的频数分布均符合Hardy-Weinberg遗传平衡法则(P>0.05)。
2.2病例组与对照组及有效组与无效组TNF-α基因型和等位基因频率分布的比较
病例组与对照组的rs1800629在基因型和等位基因(OR=0.63,95%CI:0.44~0.92)频率分布比较,差异均有统计学意义(P<0.05)。Bonferroni校正后,基因型频率分布比较差异仍然有统计学意义(P<0.05)。而病例组与对照组的rs361525、rs1800630、rs1799724在基因型和等位基因频率分布比较,差异均无统计学意义(P>0.05)(表2)。
舍曲林治疗8周后,有效组232例,无效组33例,采用χ2检验分析首发抑郁症患者TNF-α基因4个SNPS多态性位点的等位基因和基因型频率分布与舍曲林疗效的关系,结果显示,有效组与无效组的rs1800629在基因型频率分布比较,差异无统计学意义(P>0.05),而等位基因频率分布比较,差异有统计学意义(P=0.03,OR=2.26,95%CI:1.06~4.82);Bonferroni校正后,等位基因频率分布比较,差异无统计学意义(P>0.05)。有效组与无效组的rs361525在基因型和等位基因(OR=3.60,95%CI:1.72~7.51)频率分布比较,差异均有统计学意义(P<0.05);Bonferroni校正后,rs361525在基因型和等位基因頻率分布比较,差异均有统计学意义(P<0.01)。有效组与无效组的rs1800630、rs1799724在基因型和等位基因频率分布比较,差异均无统计学意义(P>0.05)(表3)。
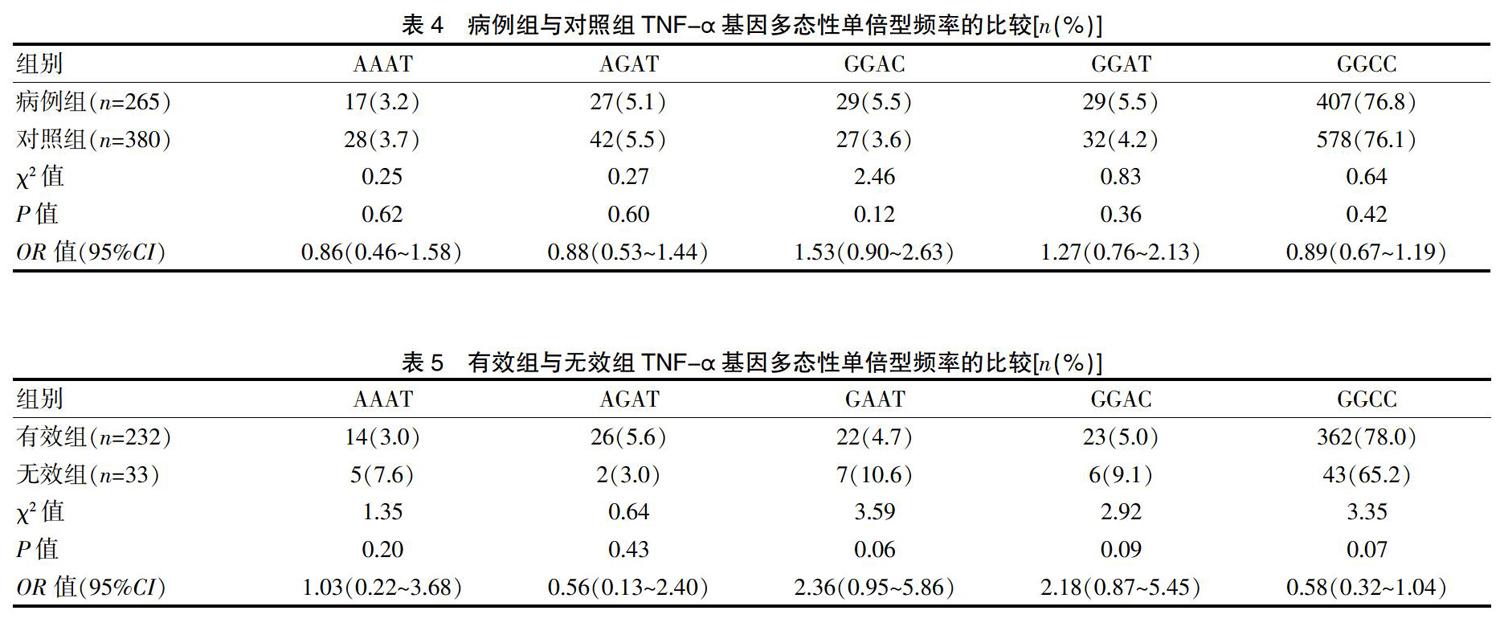
2.3病例组与对照组TNF-α基因多态性单倍型频率的比较
采用SHEsis计算单倍型频率及其组间差异,频率<0.03的单倍型未纳入统计,结果显示,病例组和对照组的单倍型频率分布比较,差异均无统计学意义(P>0.05)(表4)。
2.4有效组与无效组TNF-α基因多态性单倍型频率的比较
采用SHEsis计算单倍型频率及其组间差异,频率<0.03的单倍型未纳入统计,结果显示,有效组和无效组的单倍型频率分布比较,差异均无统计学意义(P>0.05)(表5)。
3讨论
1999年Maes提出抑郁症与炎症应答系统的激活有关,外周免疫激活通过释放前炎症细胞因子导致与抑郁症相关的各种行为、神经内分泌和神经生化改变的“抑郁症的细胞因子假说”[20]。许多动物研究证实了动物外周免疫反应过程中,无论是免疫反应还是急性或慢性应激都会引起免疫细胞因子的激活,会导致中枢神经元细胞的再生障碍及神经营养支持的减少[21-22]。研究发现,脂多糖(LPS)能有效地刺激前炎症细胞因子[白介素-1(IL-1)、白介素-6(IL-6)、TNF-α及γ-干扰素(IFN-γ)]的产生和分泌,给大鼠施用LPS可减少大鼠获取糖精溶液的频率,反映快感丧失[23]。
有证据显示,细胞因子可引起单胺递质减少。Kamata等[24]发现大鼠脑室内注射细胞因子降低额叶皮质5-羟色胺(5-HT)含量,中脑和纹状体内5-HT及其代谢产物5-HIAA都减少。研究发现,细胞因子可激活吲哚胺2,3-双加氧酶(indoleamine 2,3-dioxygenase,IDO),此酶可分解前体色胺酸(tryptophan,TRP),降低TRP的血浓度,5-HT的合成在很大程度上依赖于TRP,导致脑内5-HT含量下降[25]。此外,细胞因子激活的IDO导致犬尿氨酸通路的代谢物产生增加,导致活性氧(reactive oxygen species,ROS)过量产生和单胺氧化酶(MAO)活性增加,导致5-HT快速消耗,进一步加剧了突触前可利用5-HT的降低[26]。5-HT系统功能低下被认为是抑郁症发病的重要机制之一。
关于TNF-α基因多态性与抑郁症关联的研究,国内外均有研究,但结果不尽一致。在病例对照研究中,Jun等[27]在朝鲜人发现TNF-α-308A与抑郁症的易感性存在关联,Cerri等[28]在意大利人发现TNF-α-308G/G基因型与抑郁症的发病存在关联,Clerici等[29]在意大利人发现TNF-α-G308A与抑郁症不存在关联;Kim等[30-31]在朝鲜人发现TNF-α-308A与脑卒中(中风)后抑郁存在关联,在企图自杀的抑郁症中TNF-α-G308A是一个独立危险因素。Haastrup等[32]在丹麦人TNF-α-G238A、-G308A、-C857T、-T1031C均未发现与抑郁症存在关联。国内马心慧等[33]发现TNF-α基因启动子-857C/T位点的基因型及等位基因频率分布在重度抑郁障碍症组与正常对照组间存在统计学差异。其中,-857T的等位基因频率只在男性重度抑郁障碍症组与对照组间存在显著差异,而-308A位点的等位基因频率只在女性病例组与对照组间存在统计学差异。本研究结果显示,rs1800629基因型和等位基因在病例组和对照组之间,差异有统计学意义(P<0.05),经Bonferroni校正后,基因型仍然具有统计学意义(P<0.05)。与Jun等[27-28]的研究结果较一致。而病例组与对照组的rs361525、rs1800630、rs1799724在基因型和等位基因频率分布比较,差异均无统计学意义(P>0.05)。Holtzman等[34]在加拿大人横断面研究中,没发现TNF-α-G308A与抑郁症存在关联。Lotrich等[35]在前瞻性研究中发现TNF-α-308A与易怒有关联,而与抑郁无关。Misener等[36]在高加索、罗马、非洲人种中采用家系研究发现TNF-α多态性与起病于儿童期的情绪障碍无关。
舍曲林是一种应用较普遍的抗抑郁药物,本研究病例组应用其治疗8周后,结果显示,有效组和无效组的rs361525在基因型和等位基因频率分布比较,差异有统计学意义(P<0.05),经Bonferroni校正后,基因型和等位基因频率分布比较差异仍然有统计学意义(P<0.05)。而有效组与无效组的rs1800630、rs1799724在基因型和等位基因频率分布比较,差异均无统计学意义(P>0.05)。提示rs361525A等位基因是临床疗效欠佳的一个影响因素。
大量基因关联研究[37-38]显示,在抑郁症等多基因复杂疾病的病因学研究中,单个位点多态性的作用可能会由于其他与之连锁不平衡的位点的影响而被混淆,连锁不平衡分析及单倍型分析对于基因型-表型的关联研究可能会更为有效。本研究结果显示,在病例组与对照组、舍曲林治疗有效组与无效组不存在连锁不平衡,因此,本研究分析4位点单倍型对抑郁症易感性、舍曲林临床疗效的影响,结果提示,单倍型与抑郁症易感性、舍曲林临床疗效无关联。
研究之所以出现不同结果有多种原因:①选择的研究方法存在差异,如病例对照、家系、横断面、前瞻性研究等;②种族、民族差异;③抑郁症患者存在临床异质性,关注抑郁症的临床亚型将有助于减少临床异质性的发生,从而增加发现疾病致病因的效能,因此在今后的研究中应当将抑郁症的临床亚型症状(如典型性、非典型、合并其他的抑郁型);④研究的样本相对较小;⑤在药物与多态性方面的研究相对较少。
综上所述,rs1800629可能与中国北方汉族重度抑郁障碍患者的发病存在关系,其中-308A可能是其易感基因。在疗效方面,有效组和无效组的rs361525在基因型和等位基因频率比较,差异有统计学意义,提示rs361525A等位基因是临床疗效欠佳的一个影响因素。后期需将加大样本量进行研究,做深做细,在性别、民族、族群、种族、增加基因位点方面进行补充。再通过体内和体外研究将基因多态性与mRNA的转录和蛋白的表达联系起来,以揭示基因变异对表达水平产生的影响,进一步为临床病因和疗效指明方向。
[参考文献]
[1]Hodes GE,Kana V,Menard C,et al.Neuroimmune mechanisms of depression[J].Nat Neurosci,2015,18(10):1386-1393.
[2]Oglodek E,Szota A,Just M,et al.The role of the neuroendocrine and immune systems in the pathogenesis of depression[J].Phamacol Rep,2014,66(5):776-781.
[3]Felger JC,Cole SW,Pace TW,et al.Molecular signatures of peripheral blood mononuclear cells during chronic interferon-α treatment:Relationship with depression and fatigue[J].Psychol Med,2012,42(8):1591-1603.
[4]Musil R,Schwarz MJ,Riedel M,et al.Elevated macrophage migration inhibitory factor and decreased transforming growth factor-beta levels in major depression-no influence of celecoxib treatment[J].J Affect Disord,2011,134(1-3):217-225.
[5]Chen Y,Ouyang J,Liu S,et al.The Role of Cytokines in the Peripheral Blood of Major Depressive Patients[J].Clin Lab,2017,63(7):1207-1212.
[6]Fan N,Luo Y,Ou Y,et al.Altered serum levels of TNF-α,IL-6,and IL-18 in depressive disorder patients[J].Hum Psychopharmacol,2017,32(4).doi:10.1002/hup.2588.
[7]張丽,何军,毕斌,等.首发重度抑郁症患者血清中促炎物质水平的检测[J].中华微生物学和免疫学杂志,2015, 35(1):33-36.
[8]杨权,林凌云,李景吾,等.抑郁症患者血清细胞因子水平的研究[J].中华精神科杂志,2001,34(1):13-14.
[9]Consortium C.Sparse whole-genome sequencing identifies two loci for major depressive disorder[J].Nature,2015,523(7562):588-591.
[10]Wilson AG,Symons JA,McDowell TL,et al.Effects of a polymorphism in the human tumor necrosis factor alpha promoter on transcriptional activation[J].Proc Natl Acad Sci U S A,1997,94(7):3195-3199.
[11]D′Alfonso S,Richiardi PM.A polymorphic variation in a putative regulation box of the TNFA promoter region[J].Immunogenetics,1994,39(2):150-154.
[12]van Heel DA,Udalova IA,De Silva AP,et al.Inflammatory bowel disease is associated with a TNF polymorphism that affects an interaction between the OCT1 and NF(-kappa)B transcription factors[J].Hum Mol Genet,2002,11(11):1281-1289.
[13]Noguchi E,Yokouchi Y,Shibasaki M,et al.Association between TNFA polymorphism and the development of asthma in the Japanese population[J].Am J Respir Crit Care Med,2002,166(1):43-46.
[14]Zhou R,Wang F,Zhao G,et al.Effects of tumor necrosis factor-α polymorphism on the brain structural changes of the patients with major depressive disorder[J].Transl Psychiatry,2018,8(1):217.
[15]Jun TY,Pae CU,Chae JH,et al.Tumor necrosis factor-beta gene polymorphism may not be associated with major depressive disorder in the Korean population[J].Psychiatry Clin Neurosci,2003,57(1):31-35.
[16]Innes K,Hooper J,Bramley M,et al.Creation of a clinical classification.International statistical classification of diseases and related health problems-10th revision,Australian modification(ICD-10-AM)[J].Health Inf Manag,1997,27(1):31-38.
[17]Haastrup E,Bukh JD,Bock,C,et al.Promoter variants in IL18 are associated with onset of depression in patients previously exposed to stressful-life events[J].J Affect Disord,2012,136(1-2):134-138.
[18]王云瓊,何影.帕罗西汀片和氯米帕明片治疗抑郁症的临床研究[J].中国临床药理学杂志,2017,33(15):1409-1411,1424.
[19]Li Z,Zhang Z,He Z,et al.A partition-ligation-combination-subdivision EM algorithm for haplotype inference with multiallelic markers:update of the SHEsis(http://analysi-s.bio-x.cn)[J].Cell Res,2009,19(4):519-523.
[20]Maes M.Major depression and activation of the inflammatory response system[J].Adv Exp Med Biol,1999,461:25-46.
[21]Chesnokova V,Pechnick RN,Wawrowsky K.Chronic peripheral inflammation,hippocampal neurogenesis,and behavior[J].Brain Behav Immun,2016,58:1-8.
[22]Hritcu L,Gorgan LD.Intranigral lipopolysaccharide induced anxiety and depression by altered BDNF mRNA expression in rat hippocampus[J].Prog Neuropsychopharmacol Biol Psychiatry,2014,51:126-132.
[23]Su Q,Tao W,Huang H,et al.Protective effect of liquiritigenin on depressive-like behavior in mice after lipopolysaccharide administration[J].Psychiatry Res,2016,240:131-136.
[24]Kamata M,Higuchi H,Yoshimoto M,et al.Effect of single intracerebroventricular injection of alpha-interferon on monoamine concentrations in the rat brain[J].Eur Neuropsychopharmacol,2000,10(2):129-132.
[25]Catena-Dell′Osso M,Rotella F,Dell′Osso A,et al.Inflammation,serotonin and major depression[J].Curr Drug Targets,2013,14(5):571-577.
[26]Wichers MC,Maes M.The role of indoleamine 2,3-dioxygenase (IDO) in the pathophysiology of interferon-alpha-induced depression[J].J Psychiatry Neurosci,2004,29(1):11-17.
[27]Jun TY,Pae CU,Hoon-Han,et al.Possible association between -G308A tumour necrosis factor-alpha gene polymorphism and major depressive disorder in the Korean population[J].Psychiatr Genet,2003,13(3):179-181.
[28]Cerri AP,Arosio B,Viazzoli C,et al.The -308(G/A) single nucleotide polymorphism in the TNF-alpha gene and the risk of major depression in the elderly[J].Int J Geriatr Psychiatry,2010,25(3):219-223.
[29]Clerici M,Arosio B,Mundo E,et al.Cytokine polymorphisms in the pathophysiology of mood disorders[J].CNS Spectr,2009,14(8):419-425.
[30]Kim YK,Hong JP,Hwang JA,et al.TNF-alpha -308G>A polymorphism is associated with suicide attempts in major depressive disorder[J].J Affect Disord,2013,150(2):668-672.
[31]Kim JM,Stewart R,Kim SW,et al.Associations of cytokine gene polymorphisms with post-stroke depression[J].World J Biol Psychiatry,2012,13(8):579-587.
[32]Haastrup E,Bukh JD,Bock C,et al.Promoter variants in IL18 are associated with onset of depression in patients previously exposed to stressful-life events[J].J Affect Disord,2012,136(1-2):134-138.
[33]馬心慧,付瑜,曹淑杰,等.重度抑郁障碍与肿瘤坏死因子α和白细胞介素6基因启动子区多态性的相关性[J].武警医学,2016,27(3):259-262.
[34]Holtzman S,Abbey SE,Chan C,et al.A genetic predisposition to produce low levels of IL-10 is related to depressive symptoms:a pilot study of patients with end stage renal disease[J].Psychosomatics,2012,53(2):155-161.
[35]Lotrich FE,Ferrell RE,Rabinovitz M,et al.Labile anger during interferon alfa treatment is associated with a polymorphism in tumor necrosis factor alpha[J].Clin Neuropharmacol,2010,33(4):191-197.
[36]Misener VL,Gomez L,Wigg KG,et al.Cytokine Genes TNF,IL1A,IL1B,IL6,IL1RN and IL10,and childhood-onset mood disorders[J].Neuropsychobiology,2008,58(2):71-80.
[37]李卓文,马靖松,戚东,等.5-羟色胺受体相关基因的交互作用与抑郁症自杀行为的关联研究[J].中华行为医学与脑科学杂志,2017,26(7):610-614.
[38]孙宁,徐勇,孙俊伟,等.去甲肾上腺素转运体基因与中国汉族人群重性抑郁症关联分析[J].中国神经精神疾病杂志,2007,33(7):416-419.
(收稿日期:2020-02-18)
猜你喜欢
中国民族民间医药·上半月(2016年12期)2017-01-11
中国实用医药(2016年30期)2016-12-28
中国实用医药(2016年23期)2016-12-26
糖尿病新世界(2016年16期)2016-12-09
中国实用医药(2016年27期)2016-11-30
中国实用医药(2016年21期)2016-08-19
中国实用医药(2016年19期)2016-08-05
中国实用医药(2016年17期)2016-07-26
中国实用医药(2016年13期)2016-07-05
中国实用医药(2016年14期)2016-05-20
