
Midventricular Takotsubo syndrome
2020-07-24 05:23:22KonstantinosTheodoropoulosIoannisFelekosChrisAbellNicholasPalmerTurabAli
Journal of Geriatric Cardiology 2020年5期
Konstantinos C Theodoropoulos, Ioannis Felekos, Chris Abell, Nicholas D Palmer, Turab Ali
Department of Cardiology, Liverpool Heart and Chest Hospital NHS Foundation Trust, Liverpool, UK
Keywords: Left ventriculography; Midventricular; Takotsubo syndrome
A 78-year-old woman with a background of type 2 diabetes mellitus, hyperlipidaemia and hypertension experienced sudden onset severe chest pain while in the emergency department, after a stressful emotional event. The pain lasted for 20-30 min and the patient developed widespread T-wave inversion on 12-lead ECG. Cardiac troponin was elevated, and a bedside transthoracic echocardiogram showed moderate left ventricular systolic dysfunction(LVSD) with no significant valvular abnormalities. Hence,she was treated as an acute coronary syndrome (ACS) and her symptoms subsequently improved.
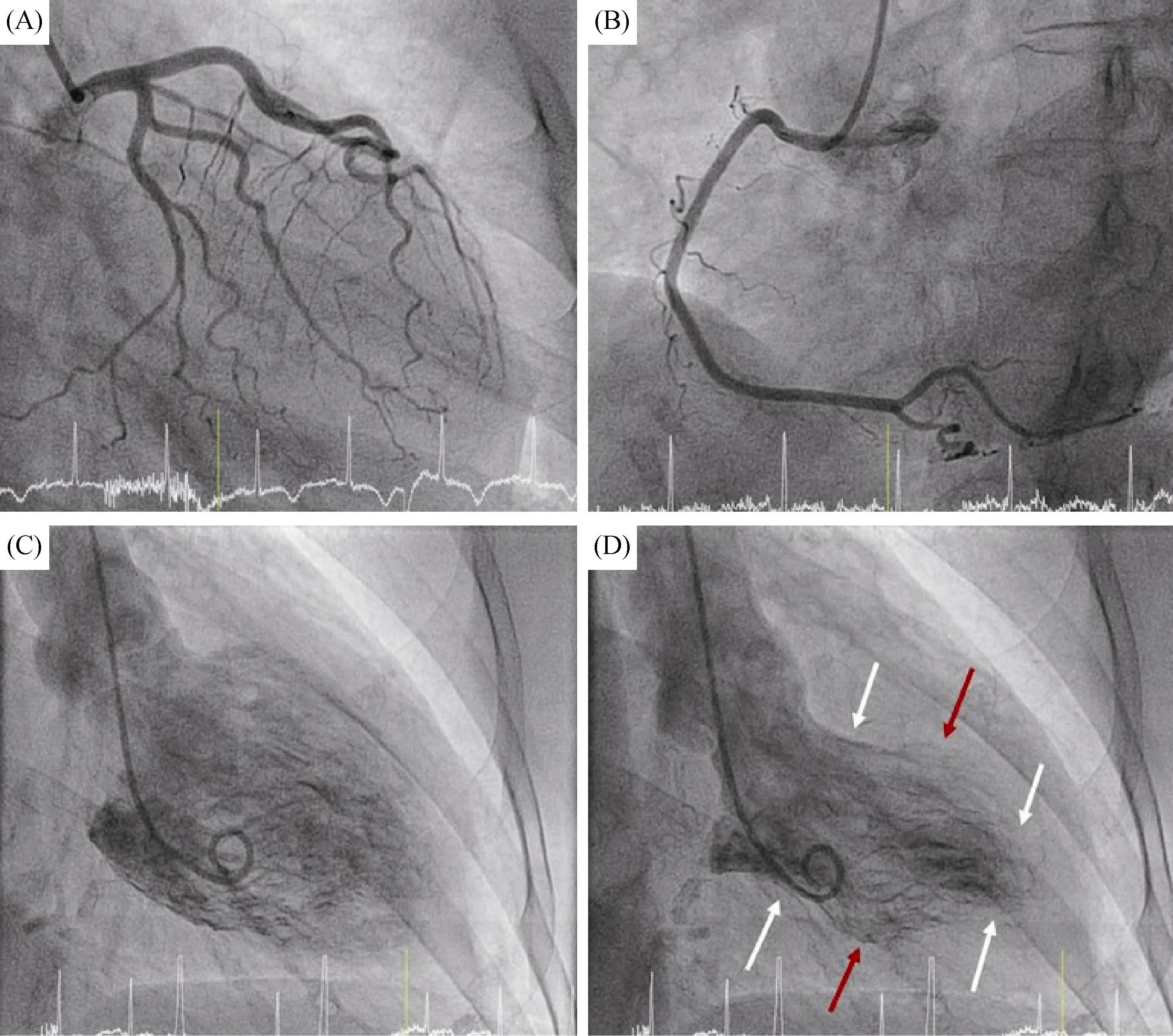
Figure 1. Invasive coronary angiography. (A): RAO caudal view showing unobstructed left coronary arteries; (B): LAO view showing unobstructed right coronary artery; (C): left ventriculography (RAO view) in diastole; and (D): left ventriculography (RAO view) in systole demonstrating akinesia of mid-level (red arrows) and preserved systolic function of basal and apical segments (white arrows). LAO: left anterior oblique; RAO: right anterior oblique.
A coronary angiogram performed via the left transradial approach, demonstrated unobstructed coronary arteries with no evidence of significant atherosclerotic disease (Figure 1A & B). The diagnosis of Takotsubo syndrome (TTS) was then formulated. Therefore, we proceeded to left ventriculography, which showed moderate LVSD with akinesia of mid-level LV myocardial walls and preserved systolic function of basal and apical segments (Figure 1C & D, Supplemental Video S1), compatible with mid-ventricular TTS.The LV end diastolic pressure was measured at 12 mmHg.She was discharged on a β-blocker and an ACE inhibitor,following an uncomplicated hospitalisation. A cardiac magnetic resonance (CMR) two months later confirmed complete LV systolic function recovery.
Takotsubo is an acute reversible heart failure syndrome which was first described in 1990 in Japan. It is estimated that 1% to 2% of patients with suspected ACS are eventually diagnosed with TTS. Diagnostic criteria include the presence of transient LV regional wall motion abnormalities,which usually extend beyond a single epicardial vascular distribution, in the absence of culprit atherosclerotic coronary artery disease.[1]A recently published international expert consensus document added the following criteria:Neurologic disorders (e.g. subarachnoid haemorrhage) or pheochromocytoma may serve as triggers for TTS. Myocarditis should be excluded with a CMR for confirmation of the diagnosis.[2]
There are four major anatomical variants of TTS: apical ballooning (75%-80% of cases), midventricular (10%-20%),basal or inverted (5%) and focal (< 1%). Other very rare variants (e.g., biventricular, isolated right or global) have also been described.[2]
The pathophysiological mechanism of the syndrome is unclear. Nevertheless, it appears that sympathetic stimulation and catecholamine surge play a central role.[1-3]An emotional,physical, or combined trigger can precede, predominantly affecting post-menopausal women. Physical triggers, which are more common in male patients can be other medical, surgical or psychiatric conditions.[1,2]Iatrogenic TTS (e.g., following stress echocardiography or an ablation procedure) has been described as well.[4,5]
Investigations are notable for various electrocardiographic abnormalities encompassing ST-segment elevation, ST depression, LBBB, T-wave inversion, and/or QTc prolongation.Cardiac biomarkers can be raised with elevation of both serum natriuretic peptides and troponin during the acute phase.[1-3]
With regards to prognosis, TTS initially believed to represent a benign condition. However, growing evidence suggests that more than 50% of the patients can have complications such as ventricular arrhythmias, acute heart failure, LV outflow tract obstruction, significant mitral regurgitation, thrombus formation in the akinetic apex and cardiogenic shock.[1,3]The LV systolic function can fully recover completely within three-to-six months.[1]
Our patient represents a case of mid-ventricular TTS who had uncomplicated recovery. Left ventriculography played a key role to final diagnosis demonstrating the characteristic mid-ventricular akinetic pattern which resembles to the ancient Greek vessel known as ‘amphora’.
 Journal of Geriatric Cardiology2020年5期
Journal of Geriatric Cardiology2020年5期
- Journal of Geriatric Cardiology的其它文章
- What is the cause of the neck hematoma? A rare complication of percutaneous coronary intervention of acute coronary syndrome: a case report
- Ischemia/hypoxia inhibits cardiomyocyte autophagy and promotes apoptosis via the Egr-1/Bim/Beclin-1 pathway
- Sagittal abdominal diameter as a marker of visceral obesity in older primary care patients
- Association of frailty with all-cause mortality and bleeding among elderly patients with acute myocardial infarction: a systematic review and meta-analysis
- Association between serum uric acid level and endothelial dysfunction in elderly individuals with untreated mild hypertension
- Relationship between high sensitivity C-reactive protein and angiographic severity of coronary artery disease