
Relationship between high sensitivity C-reactive protein and angiographic severity of coronary artery disease
2020-07-24 05:23:10NadiaBouzidiMejdiBenMessaoudFaouziMaatoukHabibGamraSalimaFerchichi
Journal of Geriatric Cardiology 2020年5期
Nadia Bouzidi, Mejdi Ben Messaoud, Faouzi Maatouk, Habib Gamra, Salima Ferchichi
1University of Monastir, Faculty of Pharmacy, Clinical and Molecular Biology Unit, Monastir, Tunisia
2University of Monastir, Cardiology A Department Fattouma Bourguiba University Hospital, Cardiothrombosis Research Laboratory, Tunisia
3University of Monastir, Cardiology B Department Fattouma Bourguiba University Hospital, Cardiothrombosis Research Laboratory, Tunisia
Abstract Background Coronary artery disease (CAD) remains a leading cause of morbidity and mortality. Cytokines play a potential role in atherosclerosis pathogenesis and progression. We investigated the association between high sensitive C-reactive protein (hsCRP) and severity of CAD. Methods CAD patients were stratified according to hsCRP cut-off value into high levels hsCRP group (≥ 8.4 mg/L) and low levels hsCRP group (< 8.4 mg/L). Severity of CAD was assessed according to artery stenosis degree and the number of vessel involved.Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS, version 23.0). Results The mean age was 60.3 ±11.0 years. The level of hsCRP was increased and ranged from 0.2 to 1020.0 mg/L. Biochemical risk factors and severity of CAD didn’t show significant differences between the two groups. In multivariate linear analysis, cardiac troponin I (cTnI) and serum amyloid A (SAA)were predictors of hsCRP. As shown in receiver operating characteristic (ROC) curve analysis performed in patients with ST-segment elevation myocardial infarction (STEMI) and compared to myonecrosis biomarkers, hsCRP (area under the curve (AUC): 0.905; 95%CI:0.844-0.966; P < 0.001) could be a powerful predictor marker in evaluating the infarct size after myocardial infarction but not better than cTnI. Conclusions HsCRP levels were not associated with the severity of CAD but could be useful in the evaluation of myocardial necrosis in patients with STEMI.
J Geriatr Cardiol 2020; 17: 256-263. doi:10.11909/j.issn.1671-5411.2020.05.003
Keywords: Coronary artery disease; High sensitive C-reactive protein; Severity
1 Introduction
Inflammation plays an essential role in the development,progression, and prognosis of coronary artery disease (CAD),and has been widely concerned as an independent risk factor for the development of CAD.[1]It is involved in many steps of atherosclerosis, and the activation of inflammatory responses may be a major contributor to plaque instability.[1,2]The activation of proinflammatory cells and the upregulation of adhesion molecules increase the production of cytokines and procoagulant substances. Theses molecules promote the thickening or rupture of atherosclerotic plaques and lead to the occurrence and development of acute coronary syndrome (ACS).[1,3]C-Reactive Protein (CRP) is a liver protein whose synthesis depends on several transacting cytokines of interleukin-6 (IL-6), IL-1 and tumor necrosis factor α (TNF-α).[4]Measurement of CRP is useful for the detection and evaluation of infection, tissue injury, inflammatory disorders, and associated diseases.[5]High concentrations of CRP were shown in patients with metabolic disorders such as insulin resistance, obesity, lipid metabolism and unstable angina (UA).[4]It has been suggested that high levels of high-sensitivity CRP (hsCRP) are associated with adverse events in various cardiovascular diseases, including heart failure, ischemic stroke, atrial fibrillation, type 2 diabetes mellitus (T2DM), hypertension and myocardial infarction(MI).[6]HsCRP levels are recognized as a strong independent risk marker for the identification of individuals at risk for future cardiovascular disease, which may be useful as an independent marker of prognosis for recurrent events in patients with stable coronary disease or ACS.[5]In this study,we investigate the relationship between hsCRP levels and severity of CAD in patients undergoing angiography.
2 Methods
2.1 Study patients
In this investigation, 310 patients with CAD undergoing coronary angiography in our University Hospital (Monastir,Tunisia) were enrolled. Patients were divided into two groups according to hsCRP cut-off levels. The first group with low hsCRP levels (< 8.4 mg/L) and the second group with high hsCRP levels (≥ 8.4 mg/L). The exclusion criteria of patients were the presence of severe respiratory disease,kidney disease, liver disease, concomitant inflammatory diseases such as infections and autoimmune disorders, or malignancy. Informed consent was obtained from all participants prior to the study. The study was approved by the National Committee for Medical and Research Ethics of Farhat Hached University Hospital (Sousse, Tunisia), which complied with the ethical principles of the WMA Declaration of Helsinki.
2.2 Angiographic diagnostic criteria
CAD was defined as the presence of 50% obstructive stenosis in at least one major coronary artery (left main coronary artery (LMCA), left anterior descending (LAD),left circumflex (LCx) or right coronary artery (RA) or major branches). Clinical characteristics of patients were recorded from hospital records. ST-elevation myocardial infarction(STEMI) was defined as the presence of chest pain (> 20 min) associated with persistent electrocardiographic elevation of the ST segment and increased concentrations of cardiac troponin I (cTnI) reflecting an acute total coronary occlusion. A rapid, complete, and sustained reperfusion by primary angioplasty or fibrinolytic therapy is mandatory.The diagnosis of non-ST segment elevation myocardial infarction (NSTEMI) was defined as the presence of persistent or transient ST-segment depression or T-wave inversion,flat T waves, pseudo-normalization of T waves, or no ECG changes at presentation. Patients have also ischemic symptoms associated with high concentrations of cTnI but without any marked change in the electrocardiogram. UA was defined as the presence of chest pain which was accelerated on exertion or rest angina. No elevation of cTnI concentrations was detected in the diagnosis. The exclusion criteria in this study were inflammatory diseases (infections, autoimmune disorders…), pregnancy, renal dysfunction, respiratory and liver disease.
2.3 The assessment of CAD severity
All patients were angiographically examined and underwent percutaneous coronary intervention (PCI). The severity of CAD was evaluated according to the number and the degree of coronary artery significant stenosis. Stenosis was defined as moderate (50%-70% stenosis), and severe (70%-99% stenosis). Patients were divided into single- and multivessel disease subgroups according to the stenosis vessels number.[7]
2.4 Laboratory tests
Serum samples were collected from study participants,and stored in aliquots at -80 °C pending use. Triglycerides(TG), total cholesterol (TC), high density lipoprotein-cholesterol (HDL-C), hsCRP, glucose, urea, creatinine, creatine phosphokinase (CPK) and creatine kinase (CK)-MB isoforms were measured using an analyser (Cobas Integra 400,Roche Diagnostic, Germany) for patients upon admission.Low density lipoprotein-cholesterol (LDL-C) was estimated by the Friedewald equation. Serum IL-6 levels was measured by electrochemiluminescence immunoassay (ECLIA)using a Cobas E601 analyzer (Roche Diagnostics, Germany). Serum amyloid A (SAA) was measured using an analyser (BN ProSpec, Siemens, Germany). Homocysteine was measured by Fluorescence polarization immunoassay(FPIA) using an analyser (Axym, Abbott, Germany).
2.5 Statistical analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS, version 23.0). Continuous variables were described as mean ± SD for normally distributed data or medians (minimum-maximum) for non-normally distributed data, as appropriate. Categorical data were summarized as frequencies or percentages. HsCRP was log transformed before analyses because its non-normally distribution. Differences in quantitative parameters between groups were performed using independent-samplesttest or Mann-WhitneyUtest, as appropriate. The univariate and multivariate linear analysis were used to identify independent factors for hsCRP levels. The predictive values of different biomarkers for the presence of CAD and evaluating infarct size, were determined by constructing receiver operating characteristic(ROC) curves and the area under the curve (AUC) was calculated.P< 0.05 were considered as significant.
3 Results
3.1 Characteristics of the study subjects
The baseline characteristics of the 310 patients with CAD are listed in Table 1. The mean age of patients was 60.3 ± 11.0 years, and consisted of 74.8% men. The prevalence of cardiovascular risk factors were: diabetes mellitus(48.4%), hypertension (47.1%), smoking (41.0%) and menopause (90.8%).
3.2 Relationship between hsCRP levels and biochemical parameters
According to the hsCRP cut-off value, patients were di-vided into high levels group (hsCRP > 8.4 mg/L) and low levels group (hsCRP < 8.4 mg/L). In Table 2, only inflammatory parameters (white blood cells (WBC), IL-6 and SAA) were significantly increased in the high hsCRP levels group respectively (WBC: 10.3 × 103/µL, IL-6: 19.8 (4.3-3640.0) pg/mL and SAA: 18.3 (1.6-1020.0) mg/L). The other biochemical parameters didn’t show any significant differences between the two groups.
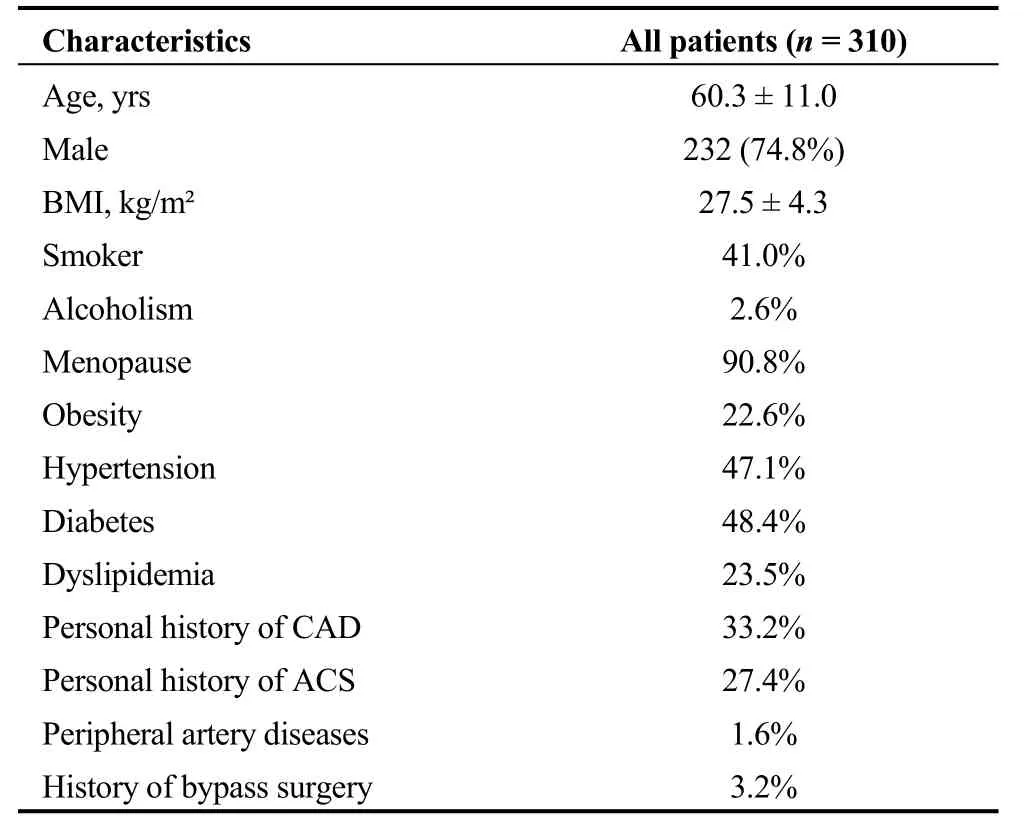
Table 1. Baseline characteristics of the study population.
3.3 Relationship between hsCRP and severity of CAD
Clinical and angiographic characteristics of patients are presented in Table 3. 71.7% of patients had severe stenosis(P= 0.157). 56.7% of patients had multi vessel disease (P=0.793). Both groups of high- and low-hsCRP levels were not associated with stenosis degree and involved vessel number. Heart rate levels in the high hsCRP levels patient group were significantly higher than levels shown in the other group (P= 0.045). To further evaluate the relation of hsCRP with the extent and severity of CAD, we measured its serum levels according to angiographic characteristics.HsCRP levels tended to be significantly associated with coronary total occlusion (P= 0.078) (Table 4). Comparing the logarithm (log) (hsCRP) values in the two patient groups between both stenosis degree and the number of vessel disease (Figure 1) showed no significant difference in each group, hsCRP levels were not associated with the severity of CAD.
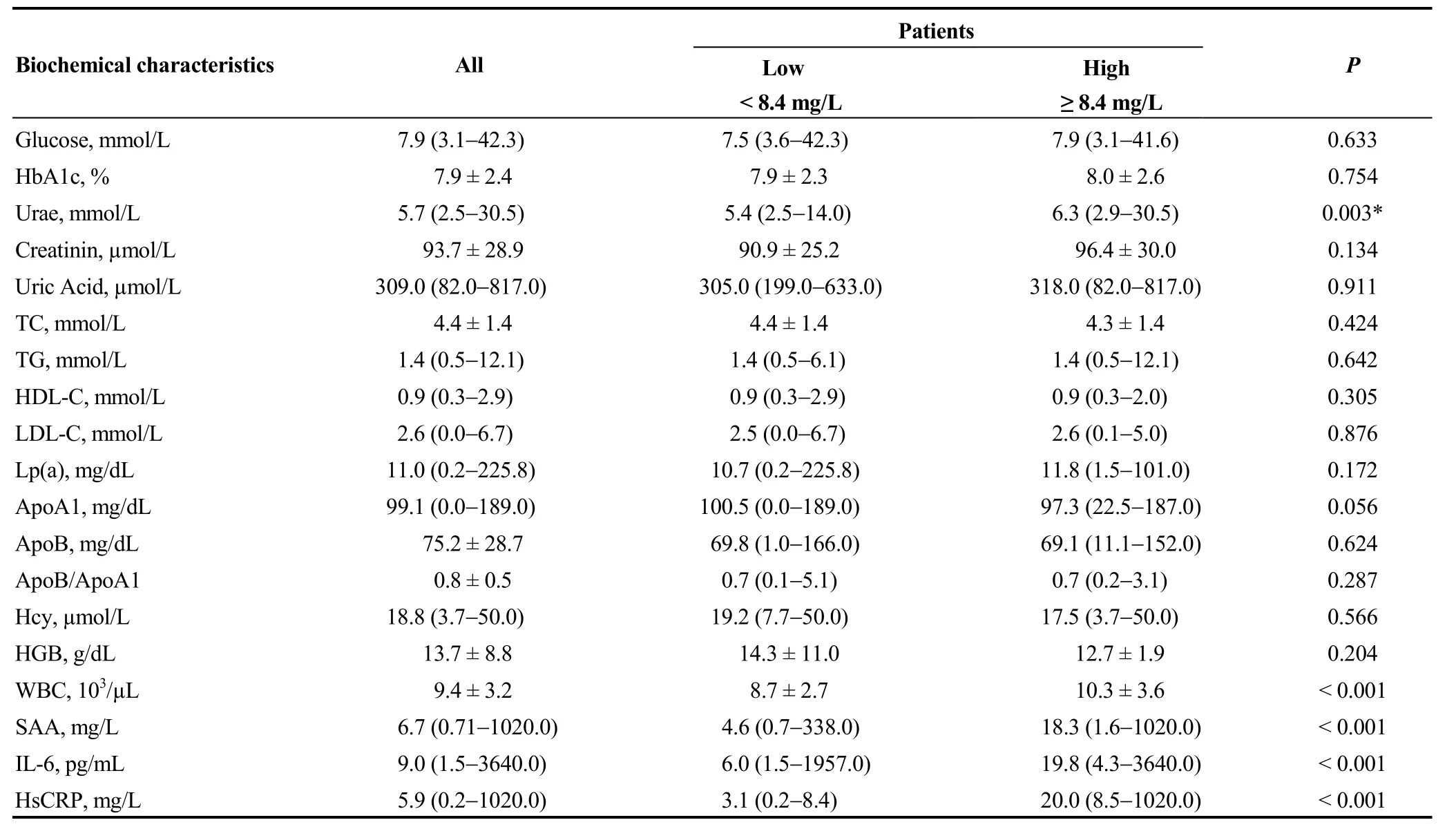
Table 2. Biochemical characteristics of patients.
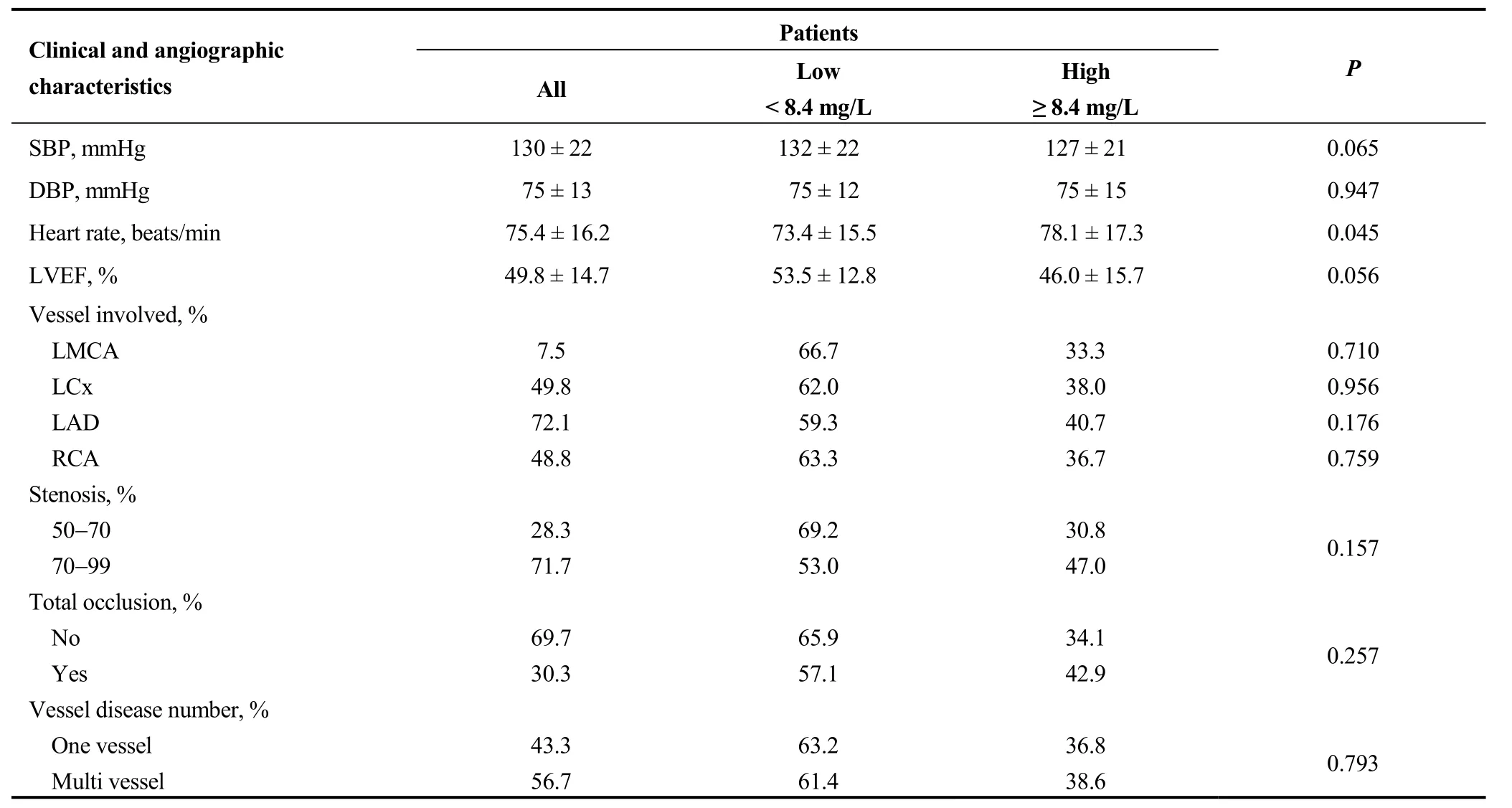
Table 3. Clinical and angiographic characteristics of patients.
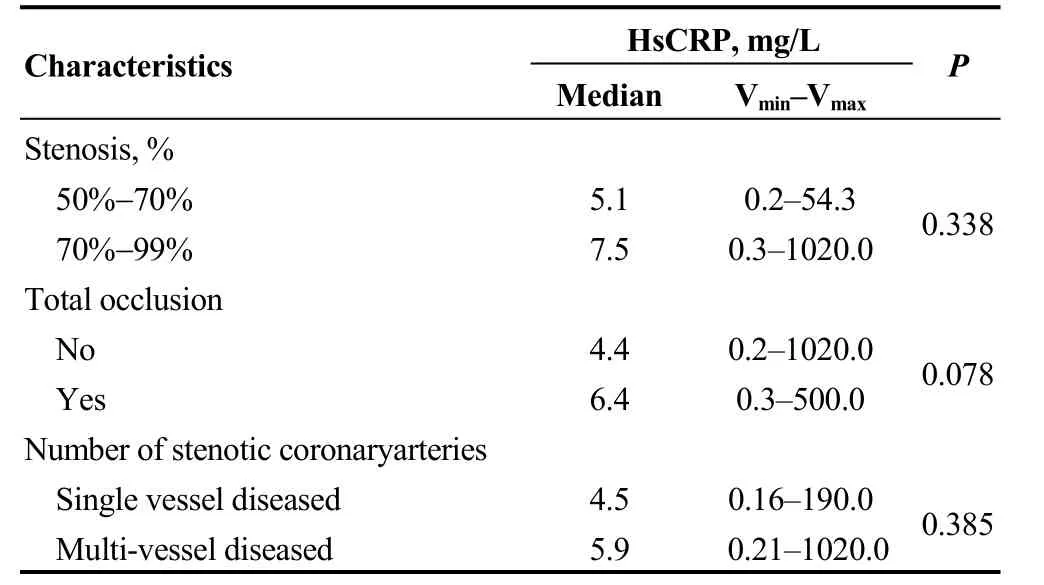
Table 4. HsCRP levels distribution according to angiographic profile.
3.4 Independent predictors of hsCRP levels
Univariate linear regression analysis was performed to evaluate the contribution of potential confounders on altered hsCRP levels in CAD. These include age, gender, body mass index (BMI), diabetes, hypertension, dyslipidemia,smoking, history of CAD and the admission clinical and biochemical diagnosis. Results from Table 5 showed that heart rate and CPK were independent predictor factors of hsCRP levels. Multivariate analysis demonstrated that only cTnI and SAA were independent predictor factors of hsCRP levels (Table 5).
3.5 Levels of hsCRP in clinical groups
HsCRP levels measured in clinical groups UA (n= 107),NSTEMI (n= 111) and STEMI (n= 92) were respectively 8.2 ± 19.2, 28.6 ± 114.5 and 30.7 ± 45.4 mg/L; medians were 3.4, 6.2 and 12.3 mg/L, respectively. The hsCRP level was significantly different between the three patient groups,and the highest levels were shown in STEMI patients(Figure 2).
3.6 Prediction of infarct size in patients with MI by ROC curve analysis
Despite the absence of correlation between hsCRP and cTnI and CPK and CK-MB in patients with MI (results are not shown), the analysis by ROC curve for hsCRP, cTnI and enzymatic markers (Figure 3) showed an AUC for hsCRP 0.905 (95% CI: 0.844-0.966;P< 0.001); CPK 0.727 (95%CI: 0.619-0.834;P< 0.001); CKMB 0.720 (95% CI: 0.618-0.821;P< 0.001); cTnI 1.00 (95% CI: 0.619-0.834;P< 0.001).These results suggest that hsCRP and cTnI were better than CKMB and CPK in predicting infarct size.
4 Discussion

Figure 1. HsCRP and severity of CAD in low and high patient group. (A): HsCRP levels in high and low groups according to stenosis degree; and (B): HsCRP levels in high and low groups according to the number of vessel disease. *P > 0.05; **P > 0.05. CAD: coronary artery disease; HsCRP: high C reactive protein.
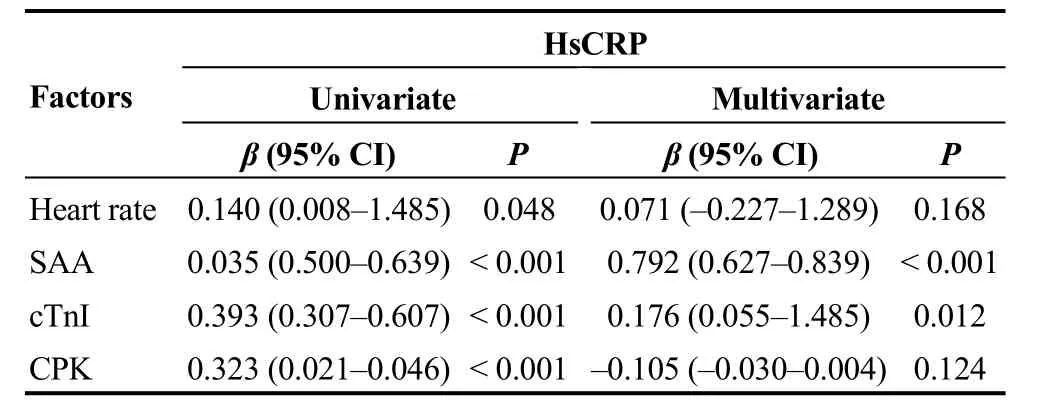
Table 5. Univariate and multivariate analysis for hsCRP.
In this study, hsCRP levels were increased in participants and tended to be associated with coronary occlusion. Stratifying patients into low and high hsCRP levels group according to the cut-off value, showed an association between hsCRP and other inflammatory markers as IL-6 and SAA.Specifically, multiple linear analysis showed that the increased level of hsCRP was associated with cTnI. We demonstrated that the severity of CAD, assessed by the stenosis degree and the number of vessel disease was not associated with hsCRP levels. The analysis by ROC curve for cTnI, hsCRP, andt enzymatic markers as CPK and CKMB showed that cTnI and hsCRP were the best markers of MI which could predict the infarct size.
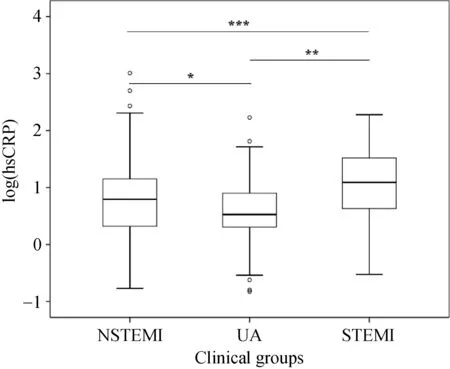
Figure 2. HsCRP levels in clinical subgroups. UA (n = 107),NSTEMI (n = 111) and STEMI (n = 92). HsCRP: high C reactive protein; STEMI: ST-segment elevation myocardial infarction;NSTEMI: non ST-segment elevation myocardial infarction; UA:unstable angina. *P = 0.044, **P < 0.001, ***P < 0.001.
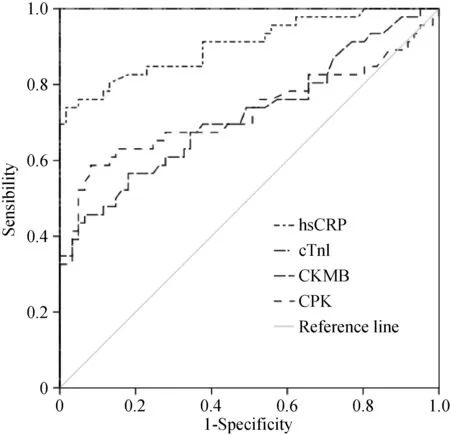
Figure 3. HsCRP in predicting infarct size in MI patients.ROC curve analysis, area under the curve for hsCRP: 0.905 (95%CI: 0.844-0.966; P < 0.001); CPK: 0.727 (95% CI: 0.619-0.834; P< 0.001); CKMB: 0.720 (95% CI: 0.618-0.821; P < 0.001); cTnI:1.00 (95% CI: 0.619-0.834; P < 0.001). CK-MB: creatine kinase MB; CPK: creatine phosphokinase; HsCRP: high C reactive protein; MI: myocardial infarction.
Inflammation is recognized as an essential factor contributing in all steps of atherosclerosis. Inflammatory markers are involved in ACS evolution by stimulating atheroma formation, destabilization of damaged atherosclerotic plaques, formation of occlusive thrombi and eventually thrombotic complications.[8,9]It has been shown that CRP is useful in MI and UA prognosis and a strong independent marker in the prediction of cardiovascular disease and mortality risk.[10-12]Elevated hsCRP concentrations were associated with endothelial dysfunction, differentiation of macrophages,smooth muscle cell proliferation and plaque vulnerability.[13]CRP promotes angiotensin proatherogenic activity, alterates structure and function of arteries, stimulates heart and vascular repair, vascular thickness, rise of peripheral vascular resistance. CRP interferes with mechanisms of arterial blood pressure regulation leading to vascular endothelium dysfunction.[14,15]The data reported in our study, didn’t show significant association between hsCRP levels and severity and extent of CAD, even when patients were categorized in low and high hsCRP levels group. According to prior investigations, the relationship between hsCRP concentrations and coronary artery stenosis grade is controversial. Previous studies showed that hsCRP didn’t correlate with stenosis degree.[16]Other studies showed that in CAD, hsCRP was associated with severity of coronary stenosis.[17,18]These controversial findings could be attributed to the difference in risk profile between patients. In fact, patients with one vessel disease could have a multiple significant and- or long plaques and stenosis, high inflammatory markers levels and high prevalence and number of cardiovascular risk factors.The multifactorial feature of CAD and the differences between clinical outcomes symptoms could explain the difference in the relationship between hsCRP and extent and severity in CAD patients.[19]Many conventional cardiovascular risk factors, such as smoking, diabetes and hypertension, were associated with elevated hsCRP levels.[20]It has been suggested that inflammation, genetic factors, age, hypercholesterolemia and diabetes caused discordance between cardiovascular risk factor burden and the extent of CAD.[19]Also, it has been found that hypolipidemic drugs decrease hsCRP levels, which supports its involvement in inflammation mechanism in cardiovascular disease.[21]Smoking as example can cause cholesterol proteins alteration stimulate lipid peroxidation, and platelet aggregation, which cause endothelial dysfunction.[22]Our findings indicated that heart rate was significantly associated with increased levels of hsCRP. It has been proposed that increased heart rate may reflect a disorder in the autonomic nervous system.[23]Following a vagal nerve stimulation, tumor necrosis factor and other cytokines were lowly expressed from macrophages inducing inflammation inhibition. Increased heart rate generates elevated mechanical stress frequency on the vascular endothelium.[24]
Despite no significant association between hsCRP and angiographic risk profile was shown in our study, the increased levels of this cytokine support the concept that hsCRP is involved in different CAD outcomes pathophysiology. Furthermore, highest levels of hsCRP were significantly shown in STEMI patients compared to NSTEMI and UA patients. These results suggested a relationship between hsCRP levels and necrosis size after a MI. On the basis that necrosis biomarkers are used and available to estimate infarct size.[25-27]the analysis by ROC curve for cTnI, CK and CK-MB, and even more for hsCRP showed that hsCRP was a powerful marker but not better than cTnI in predicting infarct size. Cardiac troponins are the ideal biomarkers in ACS diagnosis and risk evaluation. Inflammatory biomarkers,such hsCRP may provide incremental prognostic report and assessing the extent and the severity of myocardial necrosis.[28-30]In fact, inflammatory responses during myocardial repair process may differ among patients profile, biomarkers short half-life, the time of patient admission and blood collection recruitment time. These factors could explain the no correlation between hsCRP levels and cardiovascular myonecrosis markers. Previous studies reported that higher hsCRP concentrations were associated with large myocardial necrosis acute phase of inflammatory response depends on ventricular function and repair, ischemic and reperfusion necrosis.[31]
In patients with STEMI, elevated levels of hsCRP were associated with myocardial damage size and major adverse cardiac events.[14]According to prior investigations and independently from other prognosis markers, early and highly expressed hsCRP in post infarction is associated with high risk of cardiac and early mechanical complication. This increase was not useful in the prognosis of reinfarction.[13,31]Many studies suggested that hsCRP could be a predictor marker of postprocedural complications,[13]mortality risk stratification, all-cause death[19,24]and total stroke.[32,33]
The patients enrolled in this study come from a single center and the number of participants was limited which make this study unable to present the Tunisian population.Despite the common pathophysiology process, CAD outcomes differ in clinical symptoms which distort results. We had a single measurement of hsCRP in this study, a kinetic study of hsCRP could provide more information about its role in CAD even more in STEMI patients.
HsCRP levels were not associated with the severity of CAD assessed by the stenosis degree and the number of diseased coronary vessels. Highest levels of hsCRP in patients with STEMI strongly suggest its role in myocardial necrosis evaluation.
Acknowledgements
Our study was funded by research organizations in Tunisia (Ministry of Public Health and Ministry of Higher Education and Scientific Research). The authors are grateful to the patients and volunteers for their collaboration, the entire team for collecting blood samples from patients (Cardiology Department, Fattouma Bourguiba University Hospital, Monastir, Tunisia); and the staff members of the Biochemistry Laboratory (Farhat Hached University Hospital, Sousse, Tunisia) for their technical support.
 Journal of Geriatric Cardiology2020年5期
Journal of Geriatric Cardiology2020年5期
- Journal of Geriatric Cardiology的其它文章
- Midventricular Takotsubo syndrome
- What is the cause of the neck hematoma? A rare complication of percutaneous coronary intervention of acute coronary syndrome: a case report
- Ischemia/hypoxia inhibits cardiomyocyte autophagy and promotes apoptosis via the Egr-1/Bim/Beclin-1 pathway
- Sagittal abdominal diameter as a marker of visceral obesity in older primary care patients
- Association of frailty with all-cause mortality and bleeding among elderly patients with acute myocardial infarction: a systematic review and meta-analysis
- Association between serum uric acid level and endothelial dysfunction in elderly individuals with untreated mild hypertension