
Process of becoming a mother in women receiving donated egg: Based on the grounded theory
2020-07-11 02:02:34MitraZandiSaharDabaghiNargesBagheriLankaraniRezaOmaniSamaniMojtabaNaderiTaheri
Mitra Zandi, Sahar Dabaghi, Narges Bagheri-Lankarani, Reza Omani-Samani, Mojtaba Naderi-Taheri
1Nursing Department, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Epidemiology and Reproductive Health, Reproductive Biomedicine Research Center, Royan Institute for Reproductive Biomedicine, ACECR,Tehran, Iran
3Department of Community Health and Geriatric Nursing, School of Nursing and Midwifery, University of Medical Sciences, Tehran, Iran
ABSTRACT
KEYWORDS: Infertility; Motherhood process; Donated egg;Identity insecurity; Grounded theory; Nursing; Iran
1.Introduction
Some important factors contribute to infertility, one of which is ovulation in women that is influenced by different factors such as ovarian failure, anatomical disorders, older age, menopause,problems in the immune system, transmittable genetic disorders,and various treatments (radiotherapy, chemotherapy, etc.) leading to futile oocyte[1,2].Oocyte donation is one of the methods that have led to the treatment of many infertile couples.Some infertile women cannot produce patent oocyte due to inactivity of the ovaries though they have a competent uterus.Yet, they can get pregnant by donated eggs of a healthy woman[3].Hence, the resulted child is genetically related to the father and not to the mother who has borne it[4,5].The first report of successful oocyte donation dates back to 1984[4,5].Since then, several thousands of in vitro fertilization (IVF)births have been reported around the world[3].Egg donation has been used extensively in the US and more than 3 000 live births by fresh egg donation cycles occurred in 2015 of which 27% were twins.Over 1 400 children were born in the UK via oocyte donation and IVF in 2016[6].More than half of these cycles have occurred in women over 40 years of age or older[6].No accurate statistics are available on children born by egg donation.Women can become a mother through various ways like the natural method, assisted reproductive technique (ART), and child adoption[7].Regardless of motherhood method, transition to this role is associated with many challenges and damages[7,8].Women using ART face greater tensions[9,10].Paying attention to psychosocial needs of mothers is important in the motherhood process[8].Nurses play a significant role in facilitating the motherhood process through gaining the mothers' confidence and increasing their awareness[11].The mother-nurse rapport leads to the identification and perception of mothers' concerns and awareness of the health status of mothers[12].Nurses can help reduce mothers' fears and stresses by identifying their problems and barriers, thereby facilitating the acceptance of motherhood role via supporting and training mothers[7].Considering the importance of challenges faced by first-time mothers[7,8], many studies have been carried out on these mothers[11,13-16], indicating the challenges of first-time motherhood experience.However, there are many mental, social, and ethical problems in the oocyte donation process[4].Hence, becoming a mother with donated egg has its own problems.Mother's exposure to these issues demands a deep comprehensive investigation.
Grounded theory is a general methodology for developing theory that is grounded in data which is systematically gathered and analyzed[17].Despite the theoretical scientific advancements in infertility, few full-fledged studies have focused on this subpopulation of infertile women demanding the development of more research in the alternative theoretical frameworks[4].No study was found in review of literature to have directly explored the motherhood process via donated oocyte.Therefore, given the challenges faced by mothers in IVF and ART and lack of sufficient studies on the issue, this study aimed to elucidate the process of motherhood via donated eggs.
2.Materials and methods
2.1.Setting
The research setting was Royan Institute that was one of the leading IVF centers in Tehran, capital of Iran.
2.2.Participants
Mothers at the gestational age or postpartum who received donated eggs, spoke Persian, and were inclined for participating in this study were included in the study.Sampling was done using purposive sampling method from among the women available at the Royan Institute followed by theoretical sampling.Mothers who had not decided definitely to participate and had not started the treatment course yet were excluded from the study; moreover, this study had no exclusion criteria.The 26 participating mothers were 28-44 years old with a mean age of (37.00±2.49) years.To make comparisons plausible, the mothers' ages were calculated since the birth of the offspring.As for the education level, 20(76.9%) women had diploma and sub diploma, and 6(23.1%) women had bachelor and master degree; for occupation, 22(84.6%) women were housekeepers and 4(15.4%) were employees; as for status, 5(19.2%) women were pregnant and 21(80.8%) with a child borne through donated egg.Time of infertility of the women ranged from 4 to 25 years, with an avearge time of (14.2±1.2) years.
2.3.Data gathering
The required data were gleaned by unstructured deep interviews.First, one of the staff at the Royan Institute that was in close contact with these mothers called in the participants and obtained their permission for participation and interviews.Then, if the participants agreed, their phone number was given to the researcher who subsequently contacted the participants, explained the research goals and procedures to them, and made an appointment for the interviews at the agreed time and place.The formal interviews were performed at a suitable place and time at the participants' convenience.Most participants suggested distant phone interview as they did not like to be identified.Finally, of 30 interviews completed, 7 were performed at the embryo center, 22 on the phone, and 1 in the park near the house of one participant.Moreover, there was the need for personnel's demographics in the theoretical sampling, so, an interview was done with the matron of the embryo center.Three participants were interviewed twice; hence, there were 30 interviews with 26 mothers and with one of the staff at the embryo center.All of the interviews were recorded digitally with the permission of the interviewees.The interview duration ranged between 19 to 74 min with a mean time of 40 min and they were performed individually.The data were collected during 7 months from July 2018 to January 2019.The first interview used an open-ended question: “Why did you choose to use donated egg?” The interview continued by co-construction technique using questions like “Would you please explain more”, “What do you mean by that?” “Can you give an example?...” to clarify the concept under study.Field notes were used to describe real happenings and to complete and validate the interview data.
2.4.Data analysis
The data were analyzed continuously during data collection by using Strauss & Corbin method[18]that included three phases of open, axial, and selective coding.The first author had an experience of qualitative research, especially grounded theory and each interview was assessed by one of the co-authors.Each interview was immediately transcribed verbatim and reviewed several times.The nonverbal communication and body language of the participants such as facial expressions, smiling, laughter, or giggling,pauses, emphasis, etc were recorded in parentheses along with their statements.After typing and importing the interview content into MAXQAD2010 (a software program designed for computerassisted qualitative and mixed methods data, text and multimedia analysis), the content was reread word for word and broken into semantic codes.The result of open coding was 1 786 primary codes without considering data overlaps.Semantically similar codes were categorized together as a primary category.The primary categories were revised repeatedly to form more abstract concepts.This trend continued until the categories seemed not to be able to be merged anymore, i.e., conceptual saturation was achieved.The outcome of axial coding in this study was 7 axial subcategories including:“exposure to socio-cultural constrains”, “feeling of insecurity in personal and familial identity”, “annoyance”, “protection of personal and familial identity”, “difficult and stressful treatment”, “perceived social support”, and “bitter and sweet consequences”.The final axial categories and the related subcategories were given in Figure 1.The definitions, characteristics, and interrelations of these categories would be discussed individually in the results section.

Figure 1.Axial categories and the related subcategories at the end of axial coding.
The main problem of the participants of the study was identified as“feeling of insecurity in personal and familial identity” through deep reviews of participants and reminders and considering the questions suggested by Strauss & Corbin.The next issue to be addressed after determining the participants' main problem, was the investigation of the participants' coping strategy for solving the problem and how they gradually solve the problem of feeling of insecurity in personal and familial identity.Story line was used to identify core concept during which the main problem of the participants was determined.The reaction and strategies used by the participants to solve the main problem of feeling of insecurity in personal and familial identity was“protection of personal and familial identity”.This concept was a conceptual umbrella that linked all the categories together and was identified as the axial concept.Though the interrelations among the categories rotate round the axial concept of “protection of personal and familial identity”, to create a better understanding of the interrelations in the conceptual story, the explanation of the concepts would be presented according to the course of their incidence in the field and their relations with the axial concept would be elucidated.After emergence of the core concept, the theory was determined again, this time by the use of concepts, not raw data or story line.In this study, memo recording was started with the first interview and continued till the last stages of drafting the study.A total of 83 memos were imported to MAXQDA2010.
2.5.Trustworthiness
To enhance the credibility, confirmability, and dependability of findings, the research validation was conducted on the basis of 5 criteria of Lincoln & Guba as cited in the study by Polit and Beck[19]as the following: prolonged engagement with the research topic for more than 9 years, validation through member checks by 5 participants, checking data analysis by other members of the research team who were highly qualified in qualitative studies, the use of outsider opinions via etic perspective, triangulation of data resources via sampling mothers and personnel, and time triangulation via sampling mothers at various stages of pregnancy and postpartum.Also, accurate recording of data in all stages of this study was done to ensure of dependability, confirmability, and authenticity[19].
2.6.Ethical considerations
These included obtaining permission from Tehran Royan Institute(Ec/92/1083), explanation of the importance, goals, and research method, permission for digital recording of the interviews, voluntary participation or withdrawal at any stage, the right of disagreement with voice recording, making interview appointments at the participants' convenience, information confidentiality and anonymity,observation of the rights of the research team and embryo center, and finally, observation of ethical codes of COPE during all stages of drafting and publishing the data.
3.Results
3.1.Exposure to sociocultural constraints
The concept of “exposure to sociocultural constraints” referred to mothers' exposure to customs and ceremonies, rules and regulations,values and beliefs, and knowledge and thoughts of the community that were incompatible with the process of becoming a mother through receiving donated eggs.After their definite decision for receiving donated oocyte, mothers first faced “sociocultural constraint”.This theme had three subthemes of “unawareness of and negative attitude of the community toward infertility and treatment”, “religious barriers”, and “pressures by relatives”. With unawareness of and negative attitude of the community to infertility and treatment, we meant lack of a proper context and sufficient awareness for applying this method as an innovative technology in fertility, and rendering the method as an unnatural, taboo, and strange phenomenon.Community's unawareness of infertility treatments and its negative attitude of the community toward infertility and treatment induced “feeling of insecurity in personal and familial identity”, leading to “hiding” of egg reception.
“My mother-in-law's family are very traditional and look at it as something bad; also, we did not want them to know that we go to doctor for having a child because they might get sad or angry.It was not for our own sake; rather, we did not want them to feel that it was not their grandchild and to get annoyed” (Code 4).
Oocyte donation had not been approved by all Iranian religious authorities.When a couple decides that the only way of having a child is egg donation, sometimes they faced religious barriers as their religious authority did not approve this act and the infertile woman's husband and the donor had to be pronounced as husband and wife.Sometimes, the infertile couples had to convert to another religious authority or ignore treatment and pregnancy due to opposition of their religious authority.Pressures of relatives manifested as inappropriate reactions of community members, families, and relatives to infertility and to the use of adjunct technologies of infertility in IVF and ART.This was due to unawareness and negative attitudes of the community toward infertility and treatment.These inappropriate reactions appeared mostly as verbal scolding and sometimes as practical behaviors of over-inquisitiveness, ironical sarcasm, insulting, forcing them for divorce or remarriage, pressures for having a child, etc and formed the main factors in “annoyance”and “feeling of insecurity in personal and familial identity”.
“My husband was the only son of the family, so he hadn't any financial problems.One of his maternal female cousins told him that he could manage two wives and asked him to marry another girl.She told me: ‘you are too selfish as you do not allow him to marry again.He is the only son; when he gets old, what will he do? Who is going to inherit his properties?' She looked to be very stupid in her speech; yet, I thought she was somehow right.When I saw her again, I told her that gamete donation is much better.I wanted to adopt a child from the Iranian Well-being Organization.I was sure I did not have the qualifications for that.So, I believed this method was much better.If it responds, many of my problems will be solved.Then, I would not hear much nagging,scolding, or insulting from my relatives or friends (Code 21).
“Exposure to sociocultural constraints” led to “annoyance”, and“feeling of insecurity in personal and familial identity”.
3.2.Annoyance
Annoyance consisted of a combination of feeling of “anger and unhappiness” due to “pressures by relatives” and “feeling of failure”induced by infertility and the related therapies.
3.2.1.Anger and unhappiness
The taboo nature of infertility and inappropriate social behaviors like over-inquisitiveness, backbiting, insulting and scolding, and pressures for remarriage on one hand, and difficulties of repeated treatments and failures and repeated pregnancy losses, on the other hand, had predisposed to anger, dissatisfaction, and reduced threshold of tolerance.
“I could see several times they asked my husband: ‘Why do you overwork so much when you don't have a child? Whom do you want the money for? So, I got very sad when they asked me the same question,too.I got very angry and told them that we are humans, too, and want to have a happy life.We want to live for ourselves.We do not think of or rely on others” (Code 12).
3.2.2.Feeling of failure
This feeling showed failure and disappointment due to infertility and inability to have a child and included three subthemes of “regret for not having a child”, “feeling of a vacuum in life”, and “feeling of sinfulness”.Grieving for not having a child and feeling of vacuum in life existed in all participants; nonetheless, feeling of sin was created when the wife was the culprit for infertility and the husband was patent.In such cases, the infertile women felt sinful and tried to compensate the fault even through divorce.
As said before, annoyance was created along with feeling of insecurity in personal and familial identity in the context of sociocultural constraints.
3.3.Feeling of insecurity in personal and familial identity
This feeling was a collection of anxiety, hesitation, and lack of confidence experienced by the mothers and included the subthemes of “hesitation and lack of confidence”, “concern for disintegration of family foundation”, “concern for failed treatment”, “feeling of insecurity by the donor”, “fear of betrayal”, and “fear of not being accepted as mother”.All these threatened the personal and familial identity of the mother predisposing to the application of some strategies and reactions by her.“Confounded personal identity” resulted from concern for social stigma of infertility and discrimination from ordinary members of the community.“Confounded familial identity” referred to the concern for losing the familial integrity or not recognizing the family as an ordinary normal family with its own identity by the community.
“I couldn't confide in it.I say that I am just afraid of irrelevant interventions by others.I was very cautious in this issue and did not like to say anything about it.It is not up to others at all” (Code 25).
“I was afraid that the real mother may come and then I would lose both my husband and child; then, all people would know my secret and I would lose my reputation and the like“ (Code 14).
“I always thought of it.What about if the child resembles the real mother and not me? What about if the child has a different face from ours? I said that my husband and I have both white bright skins; what about if the child has a dark complexion? This thought did not leave me even for a moment” (Code 20).
“I feel they would say I am not the real mother of the child; well,daddy is its real father anyhow; a genetic test would say that he is the real father; yet, if they understand that I am not their real mother, they may gain a different feeling toward me; I am afraid of it” (Code 27).
3.4.Protection of individual and familial identity
This theme was the main concept and action/reaction mechanism of mothers for overcoming feelings of insecurity in individual and familial insecurity.It emerged as an axial concept since it demonstrated the mothers' coping strategies against insecurity and determined the relations between other categories and incidents.This concept referred to all strategies used to solve the challenge of feeling of insecurity in personal and familial identity and achieve confidence and tranquility.It affected the “perception of relative tranquility”; nevertheless, since some strategies were efficient, the mother experienced “continued identity threat” throughout the motherhood process.Protection of personal and familial identity had various characteristics including “gradual acceptance”, “attempts to maintain the marital life”, “sensitivity in selecting donor”, “sensitivity in fetal care”, “seeking information and consultation”, “challenging the internal restlessness”, and “treatment follow-up”.
3.4.1.Gradual acceptance
Accepting egg donation and even the definitive diagnosis of infertility was usually associated with some resistance.
“At first, I felt that the child would not become a part of my body because it has no gene in my existence.I had this feeling even when the child was 1.5 months old.When it was in my abdomen and did fetal movements, I made a good relation with it; yet, when it was born, I felt it is not a part of my body.When it was born, it resembled me greatly so that my relatives said that we were like two peas in a pod; yet, I felt it was not a part of my existence though now I am ready to sacrifice myself for it” (Code 2).
3.4.2.Attempts to maintain marital life
Another strategy for overcoming feeling of insecurity in personal and familial identity was attempts to maintain familial integrity and prevent disintegration of family foundation.This was accomplished by treatment follow-up due to fear of husband's remarriage, attempts to convince the husband for accepting donated egg, ignoring the scolding and insulting observed in the community, and attempts to maintain the family and the husband.
3.4.3.Sensitivity in selecting the donor
Mothers were sensitive and obsessive in selecting the donor.All mothers had some preset criteria for selecting the donor including physical and mental health, appearance features, personality, lack of smoking or drug addiction, religious beliefs, similar values and beliefs, and education and IQ features.
“The donor should be a believer in God and religious; she should not be after debauchery and profligacy; I don't like these manners; yet, I was after such women” (Code 14).
3.4.4.Sensitivity in fetal care
This included medicinal diet, pregnancy diet, fetal healthcare,preventing damage to the fetus, staying at home to prevent abortion,attempts to breed an intelligent believer child, etc.This was another strategy used by mothers to protect the personal and familial identity.“I observed the medication regimen they told me and the nutritional diet as well; I tried to take care of myself and my child.I did what they ordered me.I bought a book entitled “Paradise Flower” and tried to do most of its useful instructions” (Code 8).
3.4.5.Seeking information and consultation
Mothers attempted to satisfy their informational needs from various sources like internet sites, books, peers, consultation with religious authorities, physicians, and IVF personnel.
“I read books and used internet; I knew, for example, what happens in the first trimester of gestation.I read it month by month and explained it to my husband.We watched internet films of pregnancy” (Code 8).
3.4.6.Treatment follow-up
Mother and husband attempted to find and introduce the donor,sought about religious issues and religiosity of the egg donation method, turned to several physicians, and followed-up the prescribed treatments.
“Then, we turned to the embryo center; they told us to await our appointment; yet, we tried to find an oocyte donor” (Code 16).
3.4.7.Challenging internal restlessness
This was one of the most important strategies used by mothers to cope with feeling of insecurity in personal and familial insecurity.It included subthemes of “association and companionship”, “selfrestraint”, “resorting to spirituality”, “hiding and seclusion”,“confidence-seeking”, “ignoring and suppression”, and “conviction”.These were the most common strategies used by the participants.
“As I worked, the time passed for me very slowly; yet, I used to wake one hour before the morning call-to-prayer time and said the recommended night prayers.I also recited some verses of the holy Qur'an as I do it now daily.I had an oblation, too.I had a vow of Salavat, i.e., praising to God, Mohammad, and his descendants.I had other vows as well before my pregnancy” (Code 8).
“When I went to Royan Institute for the last time, they told me there is no need for the test sheets/papers anymore; so, I threw all the test sheets away, etc.because they were labeled ‘Royan” (Code 19).
The strategies used by mothers were affected by influential factors some of which were debilitative and some were facilitative.One intervening variable that either facilitates or debilitates the application of the strategy of “protection of personal and familial identity” was “perceived social support”.
3.5.Perceived social support
This referred to the support perceived by mothers completely or incompletely from their available supportive sources, family,or community that can have spiritual, financial, informational,therapeutic, and care-giving aspects.It included the subthemes of“helping to maintain tolerance”, “provision of suitable healthcare”,and “confounded support”.
3.5.1.Helping to maintain tolerance
It consisted of two smaller subcategories including “husband's support and association” and “relatives' support”.
“My sister told me: ‘have a child first for God's sake and then for your own sake.You wished to have a child for many years.I am ready to donate my gamete'. She suffered much as a donor; she went back and forth between home and embryo center.Yet, she tolerated it” (Code 13).
3.5.2.Provision of suitable healthcare
This referred to a set of supportive training activities performed by some state IVF centers like the embryo center from the beginning of selecting this method by mothers till before delivery and rarely the time after that.It consisted of three smaller subthemes of“the center's support in selecting donor”, “giving awareness and consultation”, and “provision of the required facilities”.
“The counselor said that they would investigate the issue and find a donor at our level, for example, someone who is very similar to us in many aspects.Thanks to God, that thing happened” (Code 12).
3.5.3.Confounded support
This indicated insufficient support and lack of satisfaction of mothers' needs, and served as a debilitative factor in the process of becoming a mother.
“My husband's family did not support me at all.Once, my sister-inlaw even told me that I had violated the rights of their parents by not having a child.This annoyed me… If they supported us financially a little, that was good. I was financially in a very poor position.My father-in-law had thrown me out of their house.I did not have enough money to pay the rent.My husband stayed home due to spinal damage.He is a metal turner.He did not really have any money.I worked as a social worker in the center.Yet, all these things were difficult for me.The costs were heavy.It was a good thing for me if I could be insured for pregnancy” (Code 2).
Another debilitative factor in this process was “difficult stressful treatment” referred to by almost all participating mothers.It affected the mothers' decision on “temporary or permanent leaving of treatment”.
3.6.Difficult and stressful treatment
This theme consisted of five subthemes of “failure in treatment”,“difficulty in finding a suitable donor”, “deficiencies in healthcare provision system”, “financial challenges”, and “difficulties of treatment”.
3.6.1.Failure in treatment
This referred to the lack of any positive results from repeated infertility treatments and the loss of hope for having a child.It included the subthemes of “experience of repeated failures”,“incidence of complications”, and “fatigue and disappointment” due to failed treatment.
“I turned to the doctor again and again without any obvious results.I performed IUI twice; then, the doctors told me to continue it.I was really disappointed and tired of treatment” (Code 25).
“It was difficult for me.There was no end to it.The treatment process was very long.Take this pill for 20 or 30 days.Inject this ampoule this month and that vial the next month.I weighed 60 kg; now, I am nearly 85 kg.It is too heavy.It annoys me.Some of it was due to pregnancy;yet, I took much medicine, I mean, previously I injected some ampoules myself” (Code 11).
“I asked them to give me some pills to make my ovaries patent and they told me that it was no use as it would not make them patent and that I could not have a child.They disappointed me.When I came out,I was nearly knocked down by a truck.If he had not put on the brakes, I would have been overrun by it.I threw myself in front of it deliberately.I thought I was useless if I could not have a child.My family was everything for me.I loved my husband, yet it was useless without a child” (Code15).
3.6.2.Financial challenges
This included the high costs of diagnostic and therapeutic measures and also expenses due to going back and forth to treatment facilities,residence in the city where treatment was done, financial problems in leading the daily life, etc.“Financial problems” was one of the most important factors of “temporary or permanent leaving of treatment”.“The costs were backbreaking for me.It was a real challenge as I could not make the ends meet.How could I economize in daily costs so that nobody would notice it?” (Code 7).
3.6.3.Difficulty in finding a suitable donor
This included assignment of finding a suitable donor to infertile couples in most centers, difficulty in finding a donor that fitted the couple in physical appearance and other important features, difficulty in finding the donor due to sociocultural constraints, financial abuse by dealers, mediators, and even donors, recommendation of being pronounced by the donor, difficulties of going back and forth for finding a donor, withdrawal of the donor from donation, etc.
“They told us that we should find a donor ourselves.We tried much,but could not find anybody to talk to.Yet, when I talked to one of them,she was annoyed and got angry” (Code 27).
3.6.4.Difficulties of treatment
This included problems related to repeated presentations for treatment, difficulties of secret treatment, lack of a suitable residence,high mental pressure of treatment, prolonged course of treatment,spending much time for seeing the doctor, difficulties of treatment for the donor, and tolerating the pregnancy difficulties.
“I tried to make pleasure out of the trips to the doctor and have a good dyadic journey with much fun; yet, I was burning from inside; I feel nauseous as soon as I enter the hospital.It makes no difference to do it there or elsewhere, it is difficult for me to tolerate.It is difficult to await it without knowing if the result is success or failure” (Code 7).
3.6.5.Deficiencies in the healthcare provision system
These deficiencies were present in healthcare provision by infertility centers in Tehran and other towns, hospitals, and private offices that performed IVF services.These faults served as debilitative factors that hindered the motherhood course.They included lack of investigation of medical history and health of the donor, introduction of mediating dealers by the treatment facilities for finding a donor,presence of dealers in the yard of the center, inhumane behaviors, not responding the clients' questions, long waiting list, lack of spiritual support by the physician, lack of giving information on religious issues, ineffective consultation, and sometimes lack of counseling on betraying the identity of the child.These may predispose to dissatisfaction with care-giving and served as an important factor in“temporary or permanent leaving of treatment”.
“Our obstetrician sent us to social support center and they made an appointment for five years hence” (Code 5).
Application of strategies by the mother led to some bitter and sweet consequences discussed below.
3.7.Bitter and sweet consequences
These included the four characteristics of “temporary or permanent leaving of treatment”, “continued identity threat”, “perception of relative tranquility”, and “sensitivity and obsession in child breeding”.
3.7.1.Temporary or permanent leaving of treatment
This can happen due to various causes.The most important inducers were “financial challenges” and “high costs of treatment”.Other causes included “difficult and stressful treatment” and “feeling of failure in treatment”.
“At first, my ovaries were patent.They were weak and I was told to take pills to strengthen them.I did not have time, so, I discontinued treatment as I had no penny.Then, I faced this problem and it was too late” (Code 15).
3.7.2.Continued threat of identity
Despite mothers' struggle to ward off feeling of insecurity in personal and familial identity, some features of insecurity continued including feeling stressful against others' inquisitiveness, concern for betrayal of child's identity, fear of the need for genetic test in future and future betrayal, fear of betrayal of a blood group different from that of the child, fear of child recovery by the donor, concern for child's marriage with first class relatives that were religiously banned to marry, husband's scolding for having a child with egg donation, feeling of not being accepted a s a mother, and husband's threat for remarriage.This was because mothers lived in the context of sociocultural constraints and they were constantly exposed to inappropriate behaviors in the community.
“I'm afraid he may get aware of it in future and get angry at me saying that I am not its real mother.So, I liked others not to be aware of my method of having a child so that the child may not be informed of it in future.Only my husband, the dealer, and I know the issue” (Code 17).
3.7.3.Perception of relative tranquility
Perception of tranquility and confidence existed in the motherhood process and had a relative nature rather than an absolute one.It consisted of subthemes of “perception of support”, “acquisition of confidence”, “removal of infertility stigma and approval of parental identity”, “new life with the birth of child”, “satisfaction with the received services”, and “satisfaction with the experience of pregnancy through egg donation”.
“I was happy that the child at least resembled its father.Now, it is exactly like him and I am completely relieved.Previously, I always prayed that the child resemble its father so that the child might not ask itself why it is not similar to the parents; then, there would be no gossips in the family” (Code 5).
3.7.4.Sensitivity and obsession in child breeding
Parents showed excessive sensitivity and obsession in childcare that added some extra load to the care process.These included sensitivity and meticulous attention in childcare, spending time for playing with children, concern for child's future, parents' excessive dependence on the child, etc.
“My husband worships the child; he loves it so much that he does not like me to train it.He gives it whatever it likes; he rides it on whatever it likes; I told my husband not to do that; it should grow up and know that we do not have everything it wishes” (Code 16).
Generally, motherhood through egg donation in the sociocultural constrains would lead to the creation of feeling of insecurity in personal and familial identity.Mothers' methods of coping with this insecurity included protection of personal and familial identity through gradual acceptance, attempts to maintain marital life,sensitivity in selecting donor, sensitivity in fetal care, seeking information and consultation, challenging internal restlessness,and treatment follow-up.Perceived social support and difficult and stressful treatment were among the debilitative and facilitative factors in the application of strategies.Ultimately, the outcomes of the application of strategies for protecting personal and familial identity were influenced by intervening variables and can have bitter and sweet consequences (Figure 2).
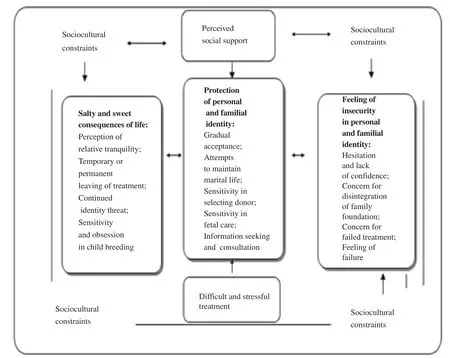
Figure 2.Suggested diagram of theory of protection of personal and familial identity.
4.Discussion
This study determined theoretically the concept of security and identity in mothers who received egg leading to the emergence of theory of “protection of personal and familial identity”.Protection of identity is mothers' conscious and deliberate struggle for coping feeling of insecurity in personal and familial identity.It manifests itself in various forms like attempts to maintain marital life, gradual acceptance, sensitivity in donor selection, sensitivity in fetal care, seeking information and consultation, challenging internal restlessness, and treatment follow-up.This happens in the context of sociocultural constraints and is, in turn, influenced by lack of some supportive parameters, anxiety, and difficulties of treatment.The sociocultural constraints that include mothers' coping with the customs and rituals, rules and regulations, values and beliefs,and knowledge and thoughts in the community incompatible with motherhood through egg donation are observed in other studies on infertility and ART technology.The study by Izadyar et al found that women sustain much mental, social, and personal pressures during their treatment[20].Moreover, the study by Zandi et al investigated infertile women's coping strategies against infertility and reported that coping with sociocultural constraints as socio-contextual conditions includes the four features of negative attitude of community toward infertility and treatments, insufficient knowledge on infertility treatments, community's inappropriate behavior toward infertility, and financial challenges[21].These results were similar to the findings on women who used surrogacy indicating that women sustained much mental pressure during the motherhood process[22].This study has been conducted in a socio-cultural context similar to the Iranian situation indicating the sociocultural pressures imposed on Iranian infertile couples.
As far as we know, no study has yet determined directly the motherhood process via oocyte donation nor has any study dealt with theoretical determination of security and identity or mothers' coping strategy against feeling of insecurity.As the findings suggested,mothers' main problem was feeling of insecurity in personal and familial identity.Some studies have referred to the masculine and feminine nature and the negative effects of infertility on these natures.For instance, the study by Loftus and Namaste[23]explained the effects of infertility on the feminine nature using identity theory.They showed that women attempt to substantiate their potential identity of motherhood and that they experience adverse consequences if there is a gap between their potential and actual identities.The study above that somehow highlights the threatened personal identity of infertile women refers to only one aspect of the major concerns of infertile women, i.e., insecurity in personal identity that is consistent with one aspect in our study.
Kirkman[24]addressed the mental aspects of having a child through a third party in their large project.Using narrative analysis, they investigated motherhood through a third party as one part of this large scale project.They focused on determining the meaning of this phenomenon for egg or fetus recipient women.A total of 36 women(21 egg and fetus recipients and 16 egg donors, and one woman as both egg recipient and fetus donor) participated in the study.In egg recipients' perspective, the genetic link with the child was of little importance in motherhood while it was not the case for oocyte donors[24].In our study, mothers emphasized their motherhood identity as real mothers and attached little importance to genetic link.This is indeed a defense mechanism against feeling of insecurity or feeling of threatened motherhood identity.
In another study, Mogobe[25]dealt with theoretical explanation of infertility from infertile women's perspective in an African community (Batswana) and found the theoretical framework of denying and preserving self.In this study, infertility is denial in infertile women's view.Loss of womanhood, loss of socioeconomic security, lack of pregnancy experience, labor and delivery, lactation and parenthood, loss of eternity through child, and loss of support by gods or ancestors or their punishment are the major concerns of these African infertile women in Batswana in this study.In their view, self-protection (self-preservation) is a personal strategy aimed at protecting oneself to prevent or reduce the damage imposed by others due to infertility.The strategy includes seeking a deeper meaning (greater belief in God), attending the feelings(succumbing to feelings, crying, depression, etc.), working on it(consultation and talking to others to find a solution to the problem),jeopardizing/correspondence (giving permission to or encouraging for remarriage), greater engagement (seeking treatment), escaping the problem (self-business, leaving treatment due to failure and burnout), and adopting a child[25].The findings by Mogobe are greatly consistent with our results; however, it seems that they have emphasized loss of womanhood, pregnancy experience, labor and delivery, lactation, and parenthood (indicating feeling of insecurity in personal identity) more than familial identity.Although Mogobe highlights fear of expulsion by espouse (that indicated in our study insecurity in familial identity), the strategies focus more on selfprotection as an individual rather than on family[25].The reason for greater emphasis in foreign studies on feeling of insecurity in personal identity while our study emphasizes familial identity can be attributed to the sociocultural structure of the community and Iranian families, the great importance of maintaining the family foundation in Iran, and hatred of Iranian women for polygamous men.
Nurses as the major elements of any healthcare system that are in direct contact with patients and those who have used IVF methods or tend to use them are required to get familiar with these methods so that they can convey information to the patients and clients.They should even be ready to donate eggs themselves for humanistic purposes if necessary or support their close relatives who want to do so[26-27].Since nurses interact with and care for recipients of donated oocytes and their families, it is mandatory for them to participate in research in this field.They can facilitate women's training in the motives for egg donation, donor selection, and betrayal issues.They ought to be specifically the voice of egg recipients and their offspring[4].
The theory developed in this study is a middle range theory that can serve as a basis for developing care guidelines or a prescription model for helping clients that receive eggs to protect their personal and familial identity.In this way, the clients' suitable strategies are reinforced and the inappropriate strategies are modified and corrected.Zandi et al[22]achieved a grounded theory in their previous study on mothers that used surrogacy.They used their findings in another independent study[28]to develop a care model for clients of surrogacy.On the whole, our results demonstrated that although clients of donated eggs reached good results, their whole process of motherhood was full of challenges and serious individual and also familial threats that need deep, holistic, and purposeful interventions.All care-providers and policy-makers ought to be aware of the participants' experiences and use them in planning, developing,and providing practical evidence-based guidelines in the field of ART and IVF technologies to provide consultation and support for clients in coping challenges.Given that this study aimed at obtaining data for discovering and determining the theoretical security of egg recipient mothers (not approval and generalization of a specific theory), the researchers faced no specific limitations.
In conclusion, this study found that the egg donation method is associated with feeling of insecurity in personal and familial identity formed in certain contexts of sociocultural constraints and is influenced by it.The clients' response to identity insecurity is protection of personal and familial identity in a conscious and multilateral manner.The negative effect of difficulties and anxiety of treatment and failure in enjoying supportive resources may influence adopting protective strategies and can be associated with positive consequences such as perception of relative tranquility or negative consequences like continued identity threat and temporary or permanent leaving of treatment.Development and implementation of theoretical guidelines on the basis of our findings and using the related opinions can also serve as effective strategies in optimal care provision.It is recommended that future studies should focus on development of care models for these clients on the basis of the results of this study to provide care with a greater emphasis on psychological support and empowerment of these clients in coping contextual conditions.Next, they should deal with evaluation of the efficacy of the developed model and the context-based programs instead of the theoretical plans of extra-professional theories.Considering the leaving of treatment by clients and their experience of difficult stressful treatment, and repeated failed treatments, the overlooked groups of clients ought to be given special attention.Mass media should inform the public about the suitable culture of behaving the infertile subpopulation and also about IVF and ART technologies available.
Conflict of interest statement
The authors report no conflict of interest.
 Asian Pacific Journal of Reproduction2020年4期
Asian Pacific Journal of Reproduction2020年4期
- Asian Pacific Journal of Reproduction的其它文章
- Prospects of diagnostic and prognostic biomarkers of pyometra in canine
- Hemodynamic changes in arterial flow velocities throughout the first six months of pregnancy in buffalo heifers by Doppler ultrasonography
- Seasonal changes in sperm parameters, testicular histology and circulating levels of reproductive hormones in the male African straw-colored fruit bat (Eidolon helvum)
- Genistein improves the vaginal epithelium thickness in a rat model of vaginal atrophy through modulation of hormone and heat shock protein 70 levels
- Food insecurity and other possible factors contributing to low birth weight: A case control study in Addis Ababa, Ethiopia
- Effects of nitric oxide on reproductive organs and related physiological processes