
Pancreatic necrosis and severity are independent risk factors for pancreatic endocrine insufficiency after acute pancreatitis: A long-term follow-up study
2020-07-10 07:08BingJunYuNianShuangLiWenHuaHeCongHeJianHuaWanYinZhuNongHuaLu
World Journal of Gastroenterology 2020年23期
Bing-Jun Yu, Nian-Shuang Li, Wen-Hua He, Cong He, Jian-Hua Wan, Yin Zhu, Nong-Hua Lu
Abstract
Key words: Acute pancreatitis; Pancreatic necrosis; Diabetes; Pancreatic necrosis;Pancreatic necrosis debridement; Endocrine function
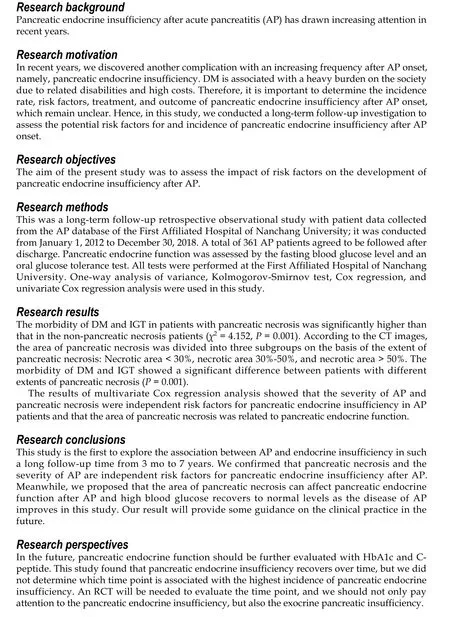
INTRODUCTION
Acute pancreatitis (AP) is an acute inflammation of the pancreas and the most common type of pancreatic disease. The incidence of AP has increased by at least 20%over the past 10 years[1]. Complications such as organ failure, systemic inflammatory response syndrome, and pancreatic necrosis, which are characterized by a high fatality rate, often occur after AP onset, especially in severe AP (SAP) patients.However, in recent years, we discovered another complication with an increasing frequency after AP onset, namely, pancreatic endocrine insufficiency, which is defined as post-pancreatitis diabetes mellitus (PPDM) or type 3c DM[2,3]. DM is associated with a heavy burden on the society due to related disabilities and high costs[2]. Therefore, it is important to determine the incidence rate, risk factors,treatment, and outcome of pancreatic endocrine insufficiency after AP onset, which remain unclear. The most controversial aspect is the risk factors for pancreatic endocrine insufficiency after AP. Previously published studies on risk factors for pancreatic endocrine insufficiency after AP showed conflicting results. In 2013, a study from New Zealand reported that hyperglycemia, obesity, and age were risk factors for pancreatic endocrine insufficiency after AP, but the severity of AP had a minimal effect[1]. However, another study[4]suggested that the severity of AP was a risk factor for DM after AP. Hence, in this study, we conducted a long-term follow-up investigation to assess the potential risk factors for and incidence of pancreatic endocrine insufficiency after AP onset.
MATERIALS AND METHODS
Patients and assessments
This was a long-term follow-up retrospective observational study with patient data collected from the AP database of the First Affiliated Hospital of Nanchang University; it was conducted from January 1, 2012 to December 30, 2018. A total of 361 AP patients agreed to be followed after discharge from the First Affiliated Hospital of Nanchang University in China. The diagnosis of pancreatic endocrine insufficiency in AP patients was performed at least 3 mo after discharge. Our study was approved by the ethics committee of our hospital (database approval number: 2011001).
Patients younger than 18 years or older than 80 years old were excluded from the study, as were those with the following conditions: (1) Diagnosed with DM before the onset of AP; (2) History of impaired glucose tolerance (IGT) or impaired fasting glucose (IFG) before the onset of AP; (3) Pancreatic insufficiency caused by other diseases, including cystic fibrosis, chronic pancreatitis (CP), pancreatic cancer, and Crohn’s disease, a history of gastrointestinal surgery, chronic kidney diseases, and liver diseases; (4) Recurrent pancreatitis or pre-AP portal hypertension; (5) Pregnant or lactating; (6) Malignant disease; and (7) Admission more than 48 h after the onset of AP. Patient demographics and clinical data, including age, sex, body mass index(BMI), etiology, complications, the severity of AP during hospitalization, treatment with minimally invasive or operative necrosectomy (ON), and death, were collected.Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were calculated based on patient data.
The diagnosis of AP was based on the 2012 revised Atlanta classification criteria[5].AP severity was classified into mild AP (MAP), moderate-severe AP (MSAP), and severe AP (SAP)[5]. Additionally, the etiologies of AP were classified into biliary[6],alcoholic[7,8], hypertriglyceridemic[7,8], and other types[8]. Organ failure was determined using the modified Marshall scoring system[5]. Pancreatic necrosis was indicated on contrast-enhanced computed tomography by diffuse enlargement of the pancreatic or peripancreatic volume, blurred edges, mild enhancement of the edema area after enhanced scanning, and no enhancement of necrotic areas. The mortality rate refers to death during hospitalization. The specific definition is shown in Supplementary Table 1.
Pancreatic function evaluation and data collection
Pancreatic endocrine function was assessed by the fasting blood glucose level and an oral glucose tolerance test (OGTT). All tests were performed at the First Affiliated Hospital of Nanchang University. We defined diabetes or IGT as pancreatic endocrine insufficiency or dysglycemia. DM and IGT were based on the diagnostic criteria for diabetes. The definition is shown in Supplementary Table 1. Symptoms such as abdominal pain and diarrhea, diet, exercise, and medication were assessed and recorded[2].
Statistical analysis
One-way analysis of variance was used to compare continuous variables, and the Kolmogorov-Smirnov test was employed to assess the normal distribution of the variables. Logarithmic transformation was adopted for variables that did not show a normal distribution. Subsequently, for analysis of the relationships between the values of possible risk factors and impaired pancreatic endocrine function, Cox regression was performed. Odds ratios (ORs) with 95% confidence intervals (CIs)were calculated.P< 0.05 indicated a significant difference. Univariate Cox regression analysis was performed to explore potential confounders. Subsequently, variables with aPvalue below 0.05 in univariate analysis were selected for multivariable Cox regression to identify the independent predictors. Statistical analyses were performed using SPSS 24.0 for Windows.
RESULTS
Baseline characteristics of the patients
A total of 4533 patients with AP were admitted to the First Affiliated Hospital of Nanchang University from 2012 to 2018, and 361 patients were ultimately enrolled in the study after the exclusion criteria were applied (Figure 1). The population included 201 (55.7%) males and 160 (44.3%) females. The mean age was 48.63 ± 13.36 years. The mean BMI was 23.62 ± 4.36. The shortest and longest follow-up times after AP were 3 mo and 7 years, respectively, with a mean ± SD follow-up time of 24.04 ± 23.67 mo.Seventy (46.7%) patients who were followed for 3 mo to 1 year, 42 (28.0%) who were followed for 1 year to 3 years, and 38 (25.3%) who were followed for 3 years to 7 years experienced dysglycemia. A total of 115 (31.9%) patients had SAP, 47 (13%) had MAP,and the remaining 199 (55.1%) had MSAP. The causes of disease included biliary causes (166, 46%), hyperlipidemia (130, 36%), alcohol (52, 14.4%), and other causes (13,3.6%). There were 137 (38.0%) AP patients with organ failure. Pancreatic necrosis was present in 152 (42.1%) patients, and debridement of necrosis was performed in 95(26.3%). A history of smoking and drinking was reported by 81 (22.4%) patients among all AP patients. The detailed data on patient conditions are listed in Table 1 and 2 and Supplemental Tables 2 and 3.
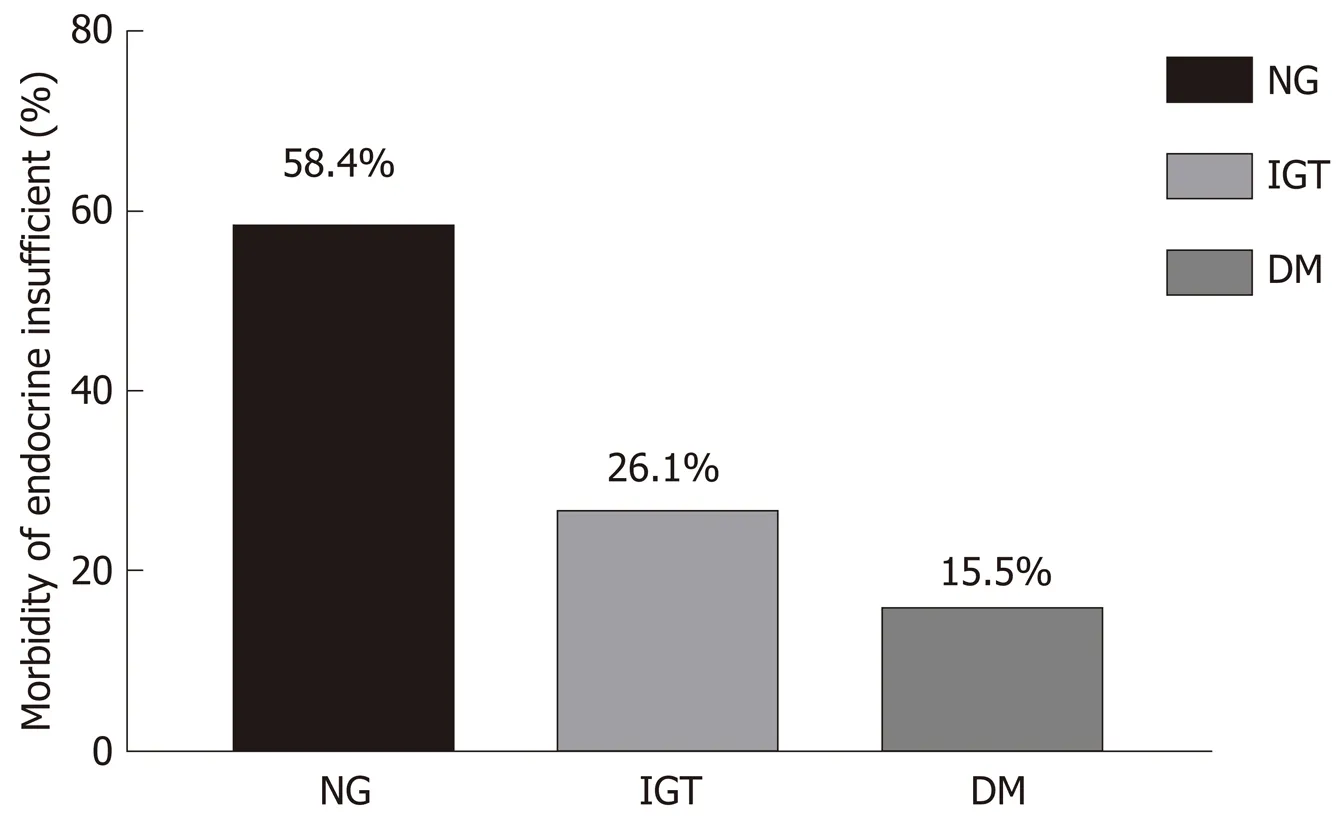
Morbidity of pancreatic endocrine insufficiency
One hundred and fifty patients were diagnosed with dysglycemia. Ninety-four(26.1%) patients were diagnosed with IGT, 56 (15.5%) were diagnosed with DM, and 211 (58.4%) had normal glucose levels (as indicated in Table 1 and Figure 2).
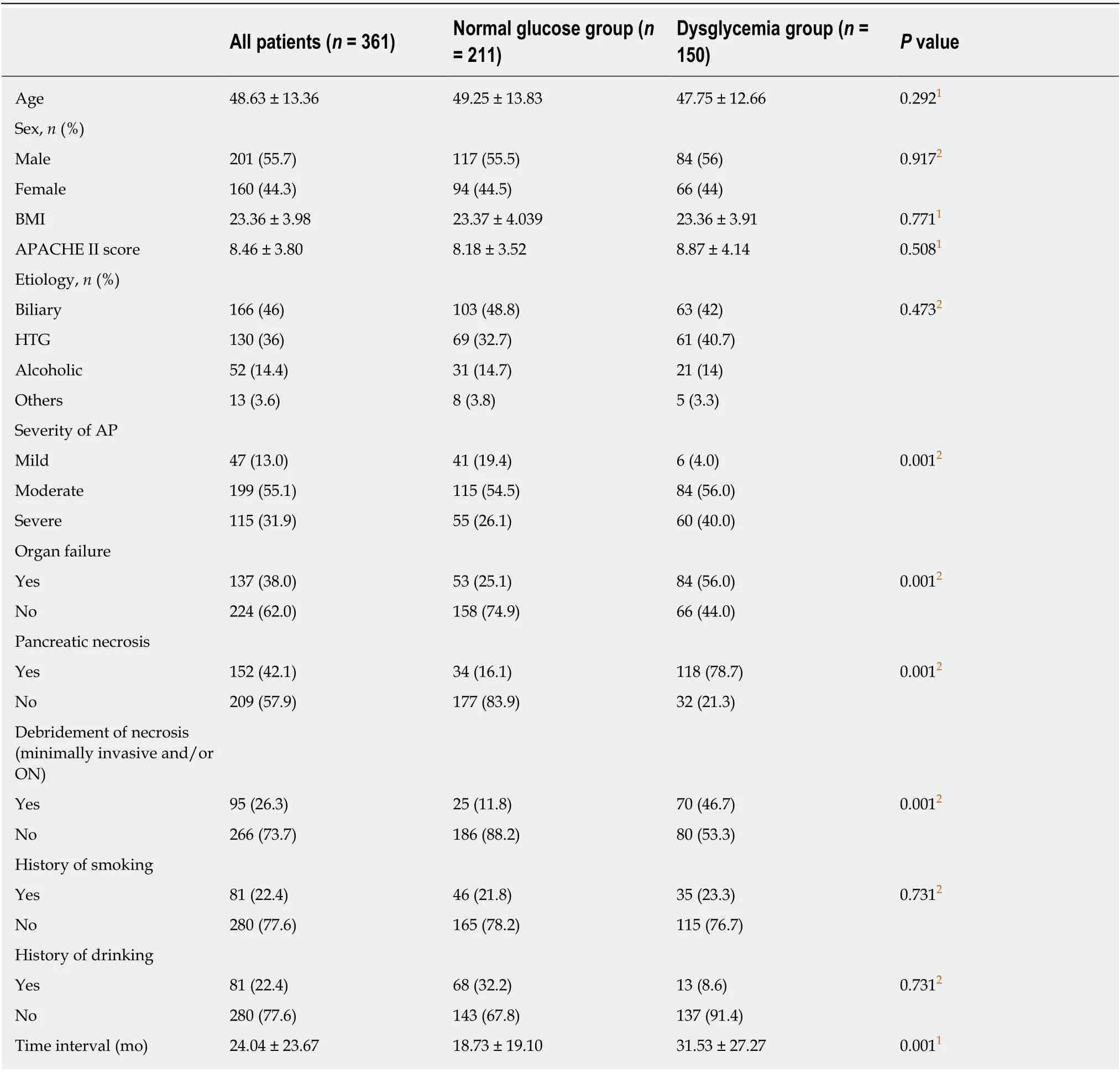
Table 1 Baseline clinical characteristics of enrolled acute pancreatitis patients
Impact of the severity of AP on pancreatic endocrine function
According to the 2012 Atlanta criteria, all AP patients were divided into MAP, MSAP,and SAP groups. Six (4%) MAP, 84 (56.0%) MSAP, and 60 (40.0%) SAP patients experienced IGT and DM, as listed in Table 1. Univariate and multivariate Cox regression analyses of severity in AP patients were performed, which revealed that there was a significant difference between the normal glucose group and the dysglycemia group (MSAP,χ2= 3.489,P= 0.004; SAP,χ2= 2.529,P= 0.039), as listed in Table 3.
Impact of etiology and organ failure on pancreatic endocrine function in AP patients
Biliary factors, HTG, and alcohol are common causes of AP worldwide. In this study,63 (42%) biliary AP patients and 61 (40.7%) HTG-AP patients experienced IGT and DM. The incidence of alcohol abuse was 14% and the incidence of other types was 3.3%, as listed in Table 1. There was no difference in the two groups regarding the etiology of AP (P> 0.05).
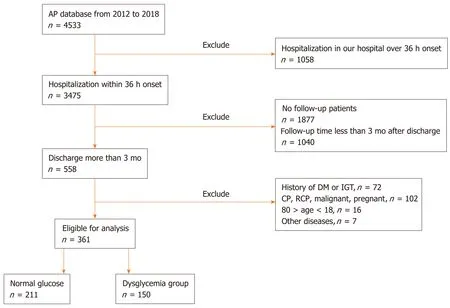
Figure 1 Study flowchart. AP: Acute pancreatitis; DM: Diabetes mellitus; IGT: Impaired glucose tolerance; CP: Chronic pancreatitis; RCP: Recurrent pancreatitis.
We found that 84 (56.0%) patients with AP and organ failure developed IGT and DM and 66 (44.0%) AP patients with organ failure did not. There were no differences between the normal glucose group and the dysglycemia group among AP patients with organ failure (P> 0.05), as listed in Table 1 and 3.
Impact of pancreatic necrosis and debridement of necrosis on pancreatic endocrine function in AP patients
Pancreatic necrosis is a complication in AP patients and debridement of necrosis, such as percutaneous catheter drainage (PCD) and/or ON, can be used to treat this complication. According to their CT images, the patients were divided into pancreatic necrosis and non-pancreatic necrosis groups, and the morbidity of DM and IGT in patients with pancreatic necrosis was significantly higher than that in the nonpancreatic necrosis patients (χ2= 4.152,P= 0.001). According to their CT images, the cases were divided into four subgroups: The head of the pancreas, the body of the pancreas, the tail of the pancreas, and the whole pancreas necrosis groups. The morbidity of DM and IGT showed no significant difference among the four subgroups, as listed in Table 2 and 3. According to the CT images, the area of pancreatic necrosis was also divided into three subgroups on the basis of the extent of pancreatic necrosis: Necrotic area < 30%, necrotic area 30%-50%, and necrotic area >50%. The morbidity of DM and IGT showed a significant difference between patients with different extents of pancreatic necrosis (P= 0.001), as listed in Table 2 and 3.
Debridement of necrosis in AP patients was performed in 70 (46.7%) patients in the normal glucose group and 25 (11.8%) patients in the dysglycemia group. Next,univariate and multivariate Cox regression analyses were used, which revealed that there was no difference between the two groups classified by debridement of necrosis in AP patients (χ2= 0.683,P= 0.054). The detailed data are listed in Table 1 and 3.
Risk factors for pancreatic endocrine insufficiency analyzed by univariate and multivariate Cox regression analyses in AP patients
Factors such as age, sex, APACHE II score, etiology, severity of AP, organ failure,pancreatic necrosis, debridement of necrosis (PCD and/or ON), and history of smoking and drinking were included in the univariate and multivariate Cox regression analyses according to the abovementioned results and clinical characteristics. The results of multivariate Cox regression analysis showed that the severity of AP and pancreatic necrosis were independent risk factors for pancreatic endocrine insufficiency in AP patients and that the area of pancreatic necrosis was related to pancreatic endocrine function. The detailed data are listed in Table 2.
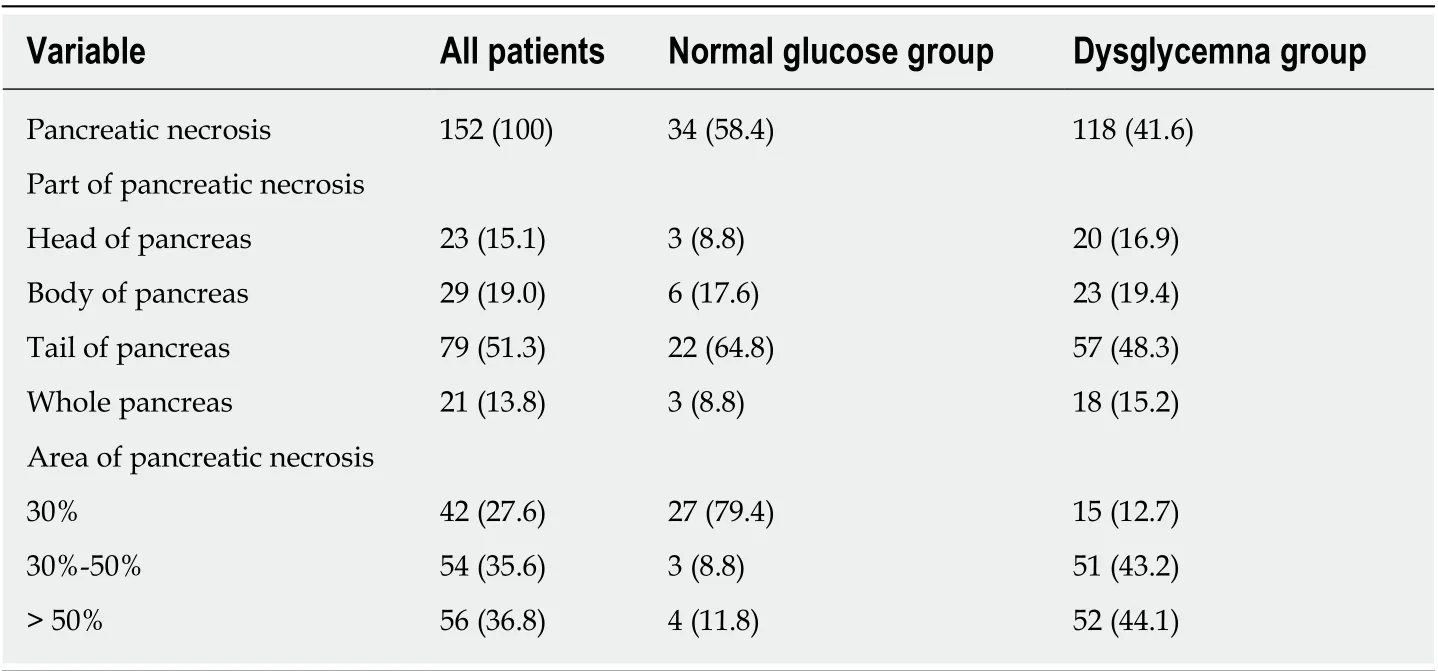
Table 2 Clinical characteristics of pancreatic necrosis, n (%)
DISCUSSION
As an inflammatory response caused by the activation of pancreatic enzymes, AP can lead to dyspepsia, edema, bleeding, and necrosis of the pancreas. Increasing number of patients will develop pancreatic endocrine insufficiency after AP onset, which has attracted more attention recently. The traditional view is that transient high blood glucose after AP is related to pancreatic microcirculation disorder, acute stress, and excessive secretion of catecholamine, which cause carbohydrate metabolism disorder.Some previous studies have shown that high blood glucose recovers to normal levels soon as the disease improves. This opinion is similar to our finding that patients who were followed for 3 mo to 1 year after discharge experienced dysglycemia more frequently than patients who were followed for 1 year to 7 years after discharge. We speculated that the recovery of pancreatic function is associated with beta cell regeneration over time[5,9-11]. However, another study reported that patients could not fully recover from hyperglycemia and that hyperglycemia could occur again after a short recovery time[12,13], even leading to the development of DM and the need for lifelong treatment with drugs or insulin, but they could not confirm whether this effect resulted from the disease or the natural course[14]. Hence, larger sample sizes and higher-quality research should be used to verify this disputed opinion.
Regarding the incidence of pancreatic endocrine insufficiency after AP, Symersky[15]found that 32% of MAP patients and 42% of SAP patients developed pancreatic endocrine insufficiency and showed that a higher risk of glucose metabolism disorder often occurs in patients who received pancreas surgery. Another review reported that the occurrence of DM after AP was 23%, which was significantly higher than that in ordinary people (4%-9%)[1]. However, in our study, we found that DM and IGT occurred in 15.5% and 26.1% of all enrolled AP patients, respectively. Based on those studies, the incidence of pancreatic endocrine insufficiency after AP is heterogeneous[16-19], and we speculate that this is due to differences in inclusion criteria, diagnostic methods for DM (OGTT, HbA1c, or C-peptide), and follow-up times. Therefore, the incidence of pancreatic endocrine insufficiency in AP patients is still controversial and needs further investigation.
It is difficult to distinguish type 2 DM from AP-induced DM in clinical practice. The WHO and American DM Association consider diabetes caused by pancreatic injury to be T3c DM. In fact, 80% of T3c DM patients have had CP. AP, pancreatic cancer, and pancreatic surgery are the other common causes of T3c DM[2,20-22]. Research on the pathomechanism of T3c DM has mostly focused on CP rather than AP. Thus, the pathomechanism of T3c DM after AP onset is not well defined. Some studies speculated that this may occur for the following reasons. First, the pancreatic islets are damaged by pancreatic necrosis or pancreatic fibrosis after AP, which inhibits the secretion of insulin from pancreatic β-cells[23,24]. Second, α-cells in the pancreas release hyperglycemia-related factors that destroy the pancreatic tissue[23,24]. Therefore, we should pay more attention to the changes in blood glucose after AP.
Some researchers considered pancreatic endocrine insufficiency to be related to recurrent attacks of AP, alcohol abuse, sex, and age but not to the severity of AP[1,18,25].Another study suggested that pancreatic endocrine insufficiency after AP was determined primarily by the severity of AP[16]. In our study, we found that the morbidity of pancreatic endocrine insufficiency in the MSAP and SAP groups was higher than that in the MAP group, which indicated that the severity of AP is correlated with pancreatic endocrine insufficiency. We hypothesized that theheterogeneity in those studies is partly due to the proportion of SAP cases; other causes may involve the occurrence and extent of pancreatic necrosis, which reflect the local circumstances of the pancreas.
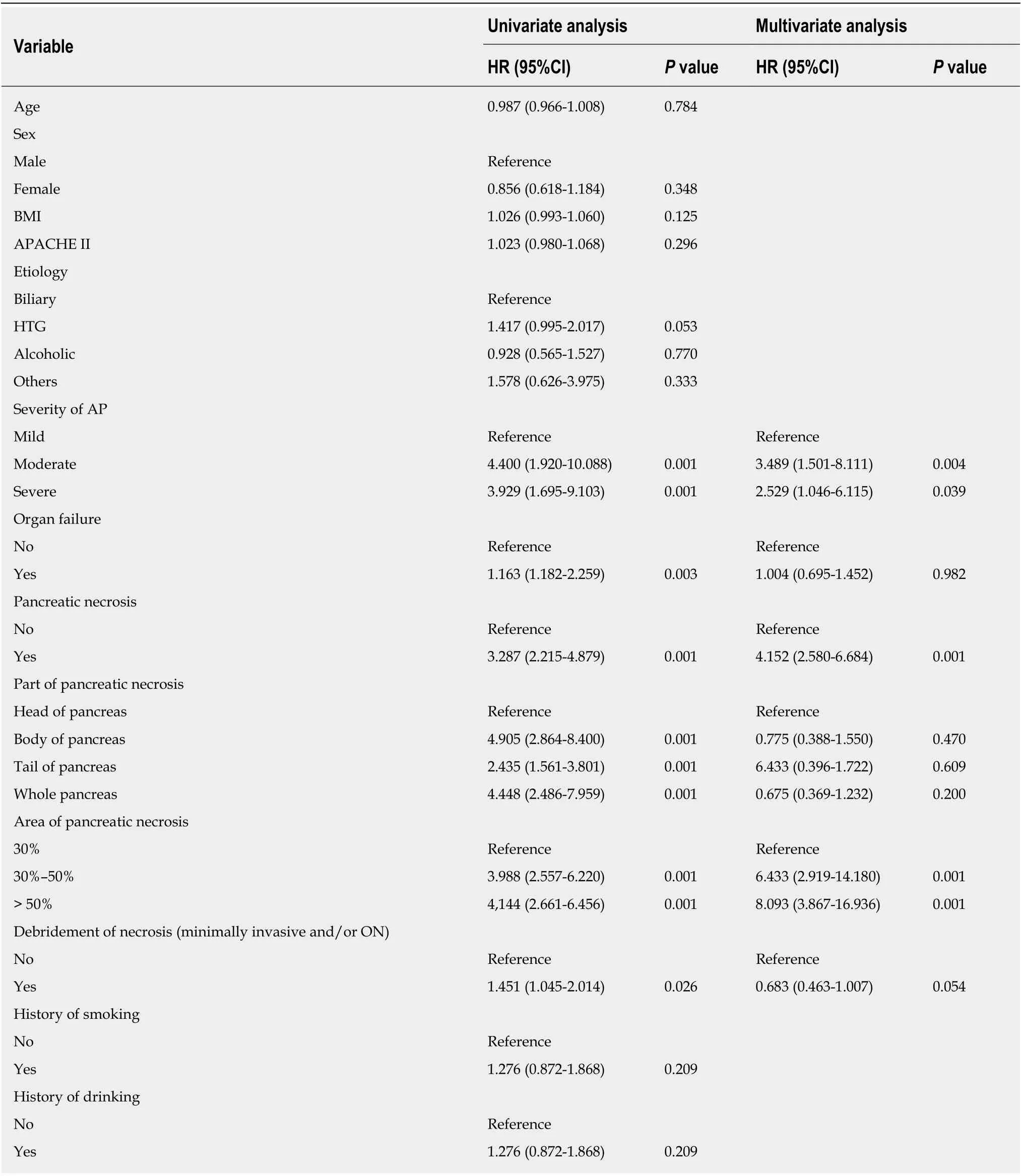
Table 3 Univariate and multivariate Cox regression analyses of prognostic factors for pancreatic endocrine insufficiency after acute pancreatitis onset
Pancreatic necrosis, which is an important marker for disease severity, was found to be an independent risk factor for pancreatic endocrine insufficiency in the Cox logistic regression analysis. Large-scale pancreatic necrosis could lead to a great decline in β-cells in the pancreas and insulin secretion[26-29]. Many studies[30,31]have reported that a large extent of pancreatic necrosis in AP patients is associated with a higher risk of pancreatic endocrine insufficiency, which is similar to our study.Patients with an area of pancreatic necrosis greater than 30% (> 50% group and 30%-50% group) developed pancreatic endocrine insufficiency more easily than patients with an area of pancreatic necrosis < 30%, which indicates that the higher the degree of pancreatic necrosis, the higher the rate of pancreatic endocrine insufficiency. In addition, different locations of pancreatic necrosis, such as the head, body, tail, and whole pancreas, did not affect pancreatic endocrine insufficiency, which was evidenced in this study and a previous study by Luet al[19]. In summary, we found that the severity of AP and pancreatic necrosis may be risk factors for pancreatic endocrine insufficiency.
Debridement of necrosis, such as PCD and/or ON treatment, is usually used to treat pancreatic necrosis to relieve symptoms in AP patients[16]. Chandrasekaranet al[32]assessed the outcomes in operative and nonoperative SAP patients and found that patients undergoing necrosectomy had a higher incidence of pancreatic endocrine insufficiency [61.9% in the operative group and 28.5% in the nonoperative group (P<0.05)]. Another study reported[19]that PCD is a protective factor against insufficient endocrine function in AP patients[31,33]. However, in our study, we found that the debridement of necrosis in AP patients was not related to pancreatic endocrine insufficiency. At present, whether the debridement of necrosis affects pancreatic endocrine insufficiency is still unclear, and we hope that more research will be done to verify whether debridement of necrosis is a risk factor for pancreatic endocrine insufficiency after AP onset.
Previous studies revealed that gender, age, history of smoking, alcohol abuse, and hypertriglyceridemia were risk factors that contributed to pancreatic endocrine insufficiency after AP onset[17-19,23,34]. However, the results of our study showed that gender, age, history of smoking and drinking, and etiology did not affect pancreatic endocrine function, which may be related to the small sample size of this study.Therefore, future research should focus on the influence of the above risk factors on pancreatic endocrine function after AP.
Strengths and limitations
Our study is the first to explore the association between AP and endocrine insufficiency with such a long follow-up time. We included patients who were followed for a long time, from 3 mo to 7 years. Our study included more AP patients than any previous study. This study not only assessed the effect of pancreatic necrosis on pancreatic endocrine function but also evaluated the effect of the area and location of pancreatic necrosis on pancreatic endocrine function. In this study, only the OGTT and fasting glucose were used to detect blood glucose. Pancreatic endocrine function should be further evaluated with HbA1c and C-peptide. This study found that pancreatic endocrine insufficiency recovers over time, but we did not determine which time point was associated with the highest incidence of pancreatic endocrine insufficiency.
In conclusion, pancreatic necrosis and the severity of AP are independent risk factors for pancreatic endocrine insufficiency after AP. The area of pancreatic necrosis can affect pancreatic endocrine function after AP.
ARTICLE HIGHLIGHTS
ACKNOWLEDGEMENTS
The authors would like to thank Professor Jian-Cheng Wang for help with the study.
 World Journal of Gastroenterology2020年23期
World Journal of Gastroenterology2020年23期
- World Journal of Gastroenterology的其它文章
- Liver-directed therapies for liver metastases from neuroendocrine neoplasms: Can laser ablation play any role?
- Potential of the ellagic acid-derived gut microbiota metabolite - Urolithin A in gastrointestinal protection
- Endosonographic diagnosis of advanced neoplasia in intraductal papillary mucinous neoplasms
- Medications in type-2 diabetics and their association with liver fibrosis
- Impact of a national basic skills in colonoscopy course on trainee performance: An interrupted time series analysis
- Sodium glucose co-transporter 2 inhibition reduces succinate levels in diabetic mice