
Liver-directed therapies for liver metastases from neuroendocrine neoplasms: Can laser ablation play any role?
2020-07-10 07:08SergioSartoriLaraBianchiFrancescaDiVecePaolaTombesi
World Journal of Gastroenterology 2020年23期
Sergio Sartori, Lara Bianchi, Francesca Di Vece, Paola Tombesi
Abstract Aggressive cytoreduction can prolong survival in patients with unresectable liver metastases (LM) from neuroendocrine neoplasms (NEN), and minimally invasive, liver-directed therapies are gaining increasing interest. Catheter-based treatments are used in disseminated disease, whereas ablation techniques are usually indicated when the number of LM is limited. Although radiofrequency ablation (RFA) is by far the most used ablative technique, the goal of this opinion review is to explore the potential role of laser ablation (LA) in the treatment of LM from NEN. LA uses thinner needles than RFA, and this is an advantage when the tumors are in at-risk locations. Moreover, the multi-fiber technique enables the use of one to four laser fibers at once, and each fiber provides an almost spherical thermal lesion of 12-15 mm in diameter. Such a characteristic enables to tailor the size of each thermal lesion to the size of each tumor, sparing the liver parenchyma more than any other liver-directed therapy, and allowing for repeated treatments with low risk of liver failure. A recent retrospective study reporting the largest series of LM treated with LA documents both safety and effectiveness of LA, that can play a useful role in the multimodality approach to LM from NEN.
Key words: Neuroendocrine neoplasms; Liver metastases; Liver-directed therapies;Ablation techniques; Laser ablation; Radiofrequency ablation
INTRODUCTION
Neuroendocrine neoplasms (NEN) encompass a heterogeneous group of neoplasms with variable biological behavior, and wide range of aggressiveness[1-3]. The incidence of NEN is increasing, and to date it is about 5.86/100000 per year[4]. NEN include both functioning tumors, which may secrete different peptide hormones, and nonfunctioning tumors. From a histologic and prognostic perspective, NEN are currently divided into low-grade indolent tumors and high-grade aggressive carcinomas[5].However, histologically low-grade tumors may sometimes have aggressive behavior[6]. Twelve percent to 22% of patients with NEN have liver metastases (LM) at presentation[6], and 40% of patients will develop LM during the course of their disease[7]. LM are unanimously considered to significantly reduce 5-year survival rates, that range from 24% to 40%[7-10]. The overall prognosis of patients with NEN differs widely according to the extent of disease, histological grade and site of the primary tumor. The 5-year survival rate can range from 60% to 90% in patients with localized NEN following surgery, whereas it barely reaches 40% in patients with distant metastases[2-4,6,7]. Treatment decision making is usually based on the clinical status of the patient, local availability of different therapeutic options, histological characteristics of the tumor, and tumor burden. Therefore, it requires a tailored approach that should be shared by a multidisciplinary team including at least medical and radiation oncologists, surgeon, pathologist, endocrinologist, and interventional radiologist. The primary treatment goal should be curative, and radical surgical resection is considered the only curative option, but it can be offered to a minority of patients[7,11-13]. Indeed, LM are often present at diagnosis, or occur during the disease,also in slow-growing tumors[8]. Moreover, LM have a high rate of recurrence after surgical resection, reaching up to 70%-94% at 5 years[7,12-15]. Chemotherapy is poorly effective, especially in well-differentiated tumors[13,16,17]. Systemic treatments, such as somatostatin analogues, targeted therapies, and peptide receptor radionuclide therapy, have been demonstrated to be effective in disease stabilization, but they have a limited role in obtaining significant radiological response[8,13,18]. In the setting of advanced NEN and indolent disease, or disease stabilized by systemic treatments, an aggressive cytoreduction with liver-directed therapies can achieve objective radiological response, prolonged survival, and hormonal symptom control[7,13,15-17,19].Surgical resection is worldwide considered the first option to treat LM, but de-bulking interventions can be offered to a very limited number of patients[7,9,13]. Recently, the threshold of liver de-bulking has been lowered from 90% to 70% of tumor burden to increase the number of eligible patients, while still achieving good survival rates[20,21].However, eligible patients remain under the threshold of 25% even with these expanded criteria[7,14,20,21].
Minimally invasive, liver-directed therapies can be used either as a primary approach in patients who are not surgical candidates, or as an adjunct to surgery and/or systemic therapies in a multimodality approach[8,13,18]. Although their impact on overall survival is still debated, liver-directed therapies have been proven to be safe and effective in both local disease control and symptom control[7-10,18]. Ablation techniques are usually indicated in patients with a limited number of small LM,whereas catheter-based treatments are mostly used in patients with disseminated and progressive disease.
CATHETER-BASED TREATMENTS
The rationale for transarterial embolization (TAE) is based on the observation that LM from NEN frequently show preferential arterial blood supply and arterial hypervascularity. The arterial occlusion induces ischemia and necrosis of the tumors,which can be enhanced by intra-arterial administration of bland chemotherapeutic agents [transarterial chemoembolization (TACE), or chemotherapeutic drugs eluting beads (DEB-TACE)], or yttrium-90 microspheres [transarterial radioembolization(TARE)]. Many studies reported that these treatments are effective in reducing tumor growth, and in controlling both hormone-related symptoms and tumor size-related symptoms[22-25]. Moreover, these procedures can be repeatedly performed until satisfactory disease control is achieved, or in case of recurrence. The 5-year overall survival rates from several studies using TACE were 50%-83%, with similar results reported for TAE (40%-67%)[8,18,22,25]. The clinical side-effects of the procedures include fever, leukocytosis, abdominal pain and elevated liver enzyme levels. More severe complications include pleural effusion, bowel ischemia, hepatic infarction, liver abscess; radiation-induced liver disease was also reported in < 2% of patients treated with TARE[23,25]. However, the occurrence of severe side-effects is quite uncommon.Interestingly, in a study by Hoet al[8]survival was not adversely affected by the presence of unresected primary tumor, a clinical response was observed in 78% of symptomatic patients, and the mean progression-free survival time was 18.5 mo including also patients with extrahepatic disease. Based on these results, the authors suggested that the presence of extrahepatic metastases or unresected primary tumor should not limit the use of TAE and TACE. In another more recent study, clinical response was observed in 95% of the patients treated with various hepatic intraarterial therapies[26]. Data about TARE in the treatment of LM from NEN are still limited, but response rates of 70%-90% have been reported[27]. TARE preferentially delivers a high dose of radiation to the tumor, while sparing much of the normal liver.Some authors reported that TARE can treat the most tumor burden with the least side effects[18]. In particular, large and bulky tumor burden with relatively well-preserved liver function may represent the best target form TARE. In patients with both a large lesion in the right lobe of the liver, and smaller lesions in the left lobe, a combined approach with TARE for the dominant right lobe metastasis, and TACE for the small lesions in the left lobe, has been proposed to obtain better results with lower risk of complications[18]. Moreover, a recent systematic review of literature suggested that TARE can also be effective for patients who previously underwent unsuccessful TAE or TACE[28]. However, although TARE seems to offer the advantage of minimal side effects in the early post-treatment period, data on long-term toxicity including radiation-induced liver disease are still quite limited[28,29]. Furthermore, a propensity score analysis suggested significant survival benefits for patients treated with TACE as compared to DEB-TACE and TARE[29]. Consequently, waiting for further and conclusive safety data on long-term tolerability of TARE, at present TACE should be considered the primary intra-arterial option for patients with multiple, unresectable LM from NEN, reserving TARE to patients with contraindications to TACE, or nonresponders to TACE[29].
ABLATION TECHNIQUES
Ablation techniques have gained increasing interest either when used alone or in association with resection in presence of a relatively low number of small LM. For tumors ≤ 4 cm in diameter and up to 7-8 in number, thermal ablation used alone or in a multimodality approach can achieve 5-year survival rates ranging from 54% to 84%[7,10,13,20,30-32]. Although surgical resection is the aggressive approach of choice,morbidity and mortality rates are still 30% and 1%-2%, respectively[7,13]. Moreover,repeated treatments are frequently needed during the course of the disease, because 5-year recurrence rates after all liver-directed interventions are very high, ranging from 80% to 95% with a median time to recurrence of 21 mo[7,12,14,15,20]. Therefore, the therapeutic decision making should be aimed at choosing a treatment that is not only effective, but also parenchymal-sparing as much as possible[7,15]. Ablation techniques deliver thermal energy, either cooling or heating the tissues. Similar to the treatment of LM from other tumors, radiofrequency ablation (RFA) is by far the most used technique to ablate LM from NEN, with 5-year survival rates up to 53% also when it is used alone[10,31-40]. Conversely, until the very last years the experiences with cryoablation, microwave ablation and laser ablation in the treatment of LM from NEN are quite sporadic and limited to case reports or small series[41-44]. However, laser ablation (LA) presents some technical characteristics that may make it an interesting alternative to RFA. LA uses laser devices that convert electrical into light energy,which determines tissue heating and cellular death by coagulative necrosis. Light is delivered via 300-μm flexible bare tip fibers that are introduced into the tumor through 21-gauge needles. The diameter of the needles is considerably thinner than that of RFA electrodes, and this characteristic can represent an advantage when the tumors are in at-risk locations[33,34]. Indeed, LA has recently been reported to be safe and effective in the treatment of small renal tumors in patients at increased bleeding risk[45], and in tumors located in the portacaval space[46]. Furthermore, the multi-fiber technique enables the use of one to four fibers at once, and each fiber provides an almost spherical thermal lesion of 12-15 mm in diameter[47,48]. By also using, when necessary, the pull-back technique, it is possible to achieve ablation areas from one to 4-5 cm in diameter. Therefore, LA can enable to treat tumors ranging from 5-6 mm to 3 cm in diameter obtaining an acceptable safety margin[47,48]. LM from NEN are variable in size, and frequently require repeated treatments because they are often multiple, and recurrence rates are very high[7,12,14,15,20]. In such settings, the need of sparing the normal liver parenchyma is mandatory. The possibility of placing from one to four laser fibers into the tumors enables to tailor the size of each thermal lesion to the size of each nodule, sparing the liver parenchyma more than any other liverdirected therapy, and allowing for multiple and repeated treatments over time with low risk of liver failure[33,34,44,47,48]. A total of twenty-eight LM have been reported to be successfully ablated in a patient with insulin-secreting NEN, and the patient was still alive and disease-free, with normal liver function, at the time the case-report was published[49]. Furthermore, a pilot study reported interesting results in the treatment of large LM from NEN by using LA followed by TACE. Complete response was obtained in lesions of 6.4 cm and 7 cm in diameter, and partial response with an estimated volume of ablated tumor tissue of approximately 80% was obtained in a lesion of 12 cm in diameter[50]. Although the number of large lesions treated was quite low, these results suggest that LA combined with TACE might be used to reduce the tumor burden in presence of large, non-surgical LM. In another prior study, the combined treatment was also reported to obtain good results by using TACE as a first procedure to downsizing the initial tumor burden as much as possible, and successively treating any residual vital tissue by LA[51].
IS THERE ANY ROLE FOR LASER ABLATION IN THE TREATMENT OF LM FROM NEN?
A very recent retrospective study reinforces the potential role of LA in the treatment of small LM from NEN, reporting the largest series of LM that were ablated by using this technique[52]. Twenty-one patients with a total of 189 LM with median long-axis diameter of 19 mm underwent ultrasound (US)-guided LA in 41 ablation sessions.Patients and tumors characteristics are detailed in Table 1. LA was performed by using the multifiber technique and the pull-back technique, as described elsewhere[52].After the end of the procedure, contrast-enhanced US (CEUS) was performed, and ablation was judged complete when no enhancing focus was observed in the treated tumor. When some enhancing foci were identified, the treatment was completed under CEUS guidance. The outcomes of the treatment were defined according to the recommendations of the International Working Group on the Image-guided Tumor Ablation[53]. Complications were classified according to the Cardiovascular and Interventional Society of Europe classification system for complications reporting[54]:Just one grade 4 (0.53%) and three grade 1 complications were observed.
One-month contrast-enhanced computed tomography showed complete ablation of all LM, and technical efficacy was 100%. Local tumor progression occurred in 10/189 LM; all of them were successfully ablated, and primary and secondary efficacy rate were 94.7% and 100%, respectively. After a median follow-up (FU) of 39 mo (range 12-99 mo, mean 45.4 ± 24), 10 patients were still alive 10 to 99 mo after LA, and 6 of them were disease-free; seven patients died owing to disease progression, whereas 4 patients died owing to causes other than NEN. All of them were disease-free at the time of death. 1-, 2-, 3-, and 5-year survival rates were 95%, 86%, 66%, and 40%,respectively. Overall survival resulted significantly higher for patients with Ki-67 expression ≤ 7% than for those with Ki-67 > 7%[52]. These results compared well with those previously reported for RFA, as well as 1-, 2-, and 3-year survival rates[10,31,35,38-40].When the data of the study were censored, the median FU was not long enough to enable to adequately evaluate 5-year survival, especially considering that four alive and disease-free subjects had a FU shorter than 3 years. Nevertheless, 1-, 2-, and 3-year survival rates were similar to those of RFA, and primary and secondary efficacy rates were even better than RFA. Therefore, it is not too big a leap to infer that also the long-term outcome might result comparable to that of RFA after an adequately long FU. Based on their results, the authors concluded that LA is a safe and effective alternative to RFA, in particular when multiple LM variable in size have to be treated and blood vessels have to be passed through to reach the lesions[52].
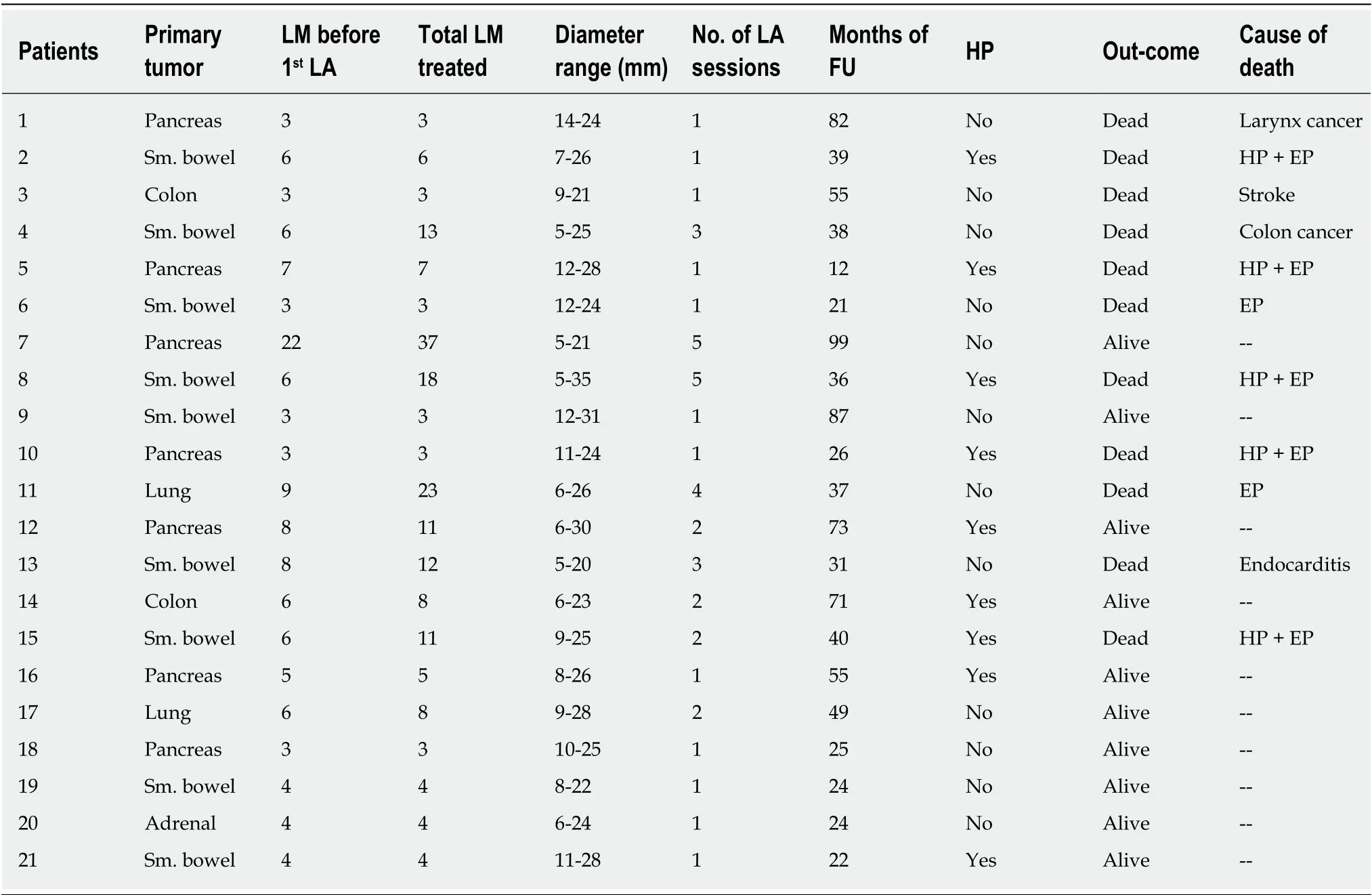
Table 1 Main characteristics of patients and tumors of the study (modified from Sartori et al[52])
CONCLUSION
Although this study was retrospective and enrolled a relatively low number of patients, in our opinion it provides interesting information and suggests that a further weapon can be added to the armory of the liver-directed therapies. The relative rarity of NEN and their heterogeneity make quite hard to plan prospective studies enrolling a sufficiently high number of patients: Indeed, and all the trials published in literature on the ablation therapies of LM from NEN are retrospective[9,10,30,31,35-40,42-44].Furthermore, the study reports the largest series of LM that underwent LA, and only two trials evaluating the efficacy of RFA used alone involved larger series of LM from NEN[31,38]. The role played by each single liver-directed therapy in the long-term outcome of patients with advanced NEN can not be reliably assessed, as they often undergo sequential and multimodality therapies[6]. Nevertheless, the results of the study were very promising. LA, used alone or in combination with surgery, catheterbased treatments, and systemic therapies, should be taken into account in the multimodality tailored approach to the patients with LM from NEN. However,further studies involving larger series of patients followed for a longer time are needed to better evaluate the long-term efficacy of this liver-directed therapy.
 World Journal of Gastroenterology2020年23期
World Journal of Gastroenterology2020年23期
- World Journal of Gastroenterology的其它文章
- Potential of the ellagic acid-derived gut microbiota metabolite - Urolithin A in gastrointestinal protection
- Endosonographic diagnosis of advanced neoplasia in intraductal papillary mucinous neoplasms
- Medications in type-2 diabetics and their association with liver fibrosis
- Pancreatic necrosis and severity are independent risk factors for pancreatic endocrine insufficiency after acute pancreatitis: A long-term follow-up study
- Impact of a national basic skills in colonoscopy course on trainee performance: An interrupted time series analysis
- Sodium glucose co-transporter 2 inhibition reduces succinate levels in diabetic mice