
Neoadjuvant chemoradiation changes podoplanin expression in esophageal cancer patients
2020-07-10 07:10UteWarneckeEberzPatrickPlumViolaSchweinsbergUtaDrebberChristianeBrunsDoloresllerArnulflscherElfriedeBollschweiler
World Journal of Gastroenterology 2020年23期
Ute Warnecke-Eberz, Patrick Plum, Viola Schweinsberg, Uta Drebber, Christiane J Bruns, Dolores T Müller,Arnulf H Hölscher, Elfriede Bollschweiler
Abstract
Key words: Esophageal cancer; Response prediction; Prognosis; D2-40;Posttranscriptional regulation; miRNA-363
INTRODUCTION
Esophageal squamous cell- (ESCC) and adenocarcinoma (EAC) are common malignancies worldwide[1]. EAC is the most rapidly increasing cancer in the Western world, thus ESCC no longer represents the most prevalent histological subtype[2].These two tumor types differ in risk factors and biological characteristics[3,4].
The poor prognosis of patients with locally advanced cancer encouraged the assessment of neoadjuvant treatment strategies to improve patients’ survival[5]. Since only responders, 40% to 50% of all patients profit by better survival, after going through the burden of chemoradiation, we urgently need markers predicting response prior to therapy[6,7]. The molecular predictive factors previously identified,failed translation to clinical application[8-10]. There is an additional need for markers indicating tumor progression and prognosis. Putative markers include growth-factor receptors, enzymes of angiogenesis, tumor suppressor genes, cell cycle regulators,enzymes involved in DNA repair, apoptosis and in degradation of extracellular matrix[11-13]. In addition to predictive and prognostic markers, novel targets for therapy are imperative for the future approach of a tailored multimodality treatment and its surveillance.
Podoplanin is a mucin-type transmembrane glycoprotein, thought to be one of the cancer stem cell markers for squamous-cell carcinoma in several tumor entities,including esophageal cancer[14]. Podoplanin has been identified as a platelet aggregation-inducing factor and a specific marker for lymphatic vessels[15,16]. It has been shown to stimulate invasion and migration of tumor cells and was correlated to lymph node metastasis, disease stage, lymphatic and vascular invasion, recurrence and poor prognosis[17].
MicroRNAs are small non-coding RNAs that act post-transcriptionally as master regulators for a variety of mRNA targets by sequence homology[18,19]. miR-363 has been reported to be deregulated in several tumors and has been associated with podoplanin expression[20]. Knowledge about regulation of podoplanin expression in esophageal cancer is scarse. The mechanism of re-expression of podoplanin in tumor cells of ESCC still has to be elucidated.
The aim of the present study was to determine expression of podoplanin protein in esophageal cancer patients with regard to a potential benefit for personalization of neoadjuvant treatment of esophageal carcinoma. We evaluated its predictive impact for therapy response and prognosis and a potential association of post-transcriptional regulation by miR-363 as one mechanism of deregulation of podoplanin expression in cancer.
MATERIALS AND METHODS
Patients, demographic data, and neoadjuvant therapy regime
One hundred and ninety-five patients with advanced esophageal cancer (clinical T2-3,Nx, M0) who received transthoracic esophagectomy are characterized in Table 1.Matching endoscopic biopsies and resection tissue were available for 56 primary surgery ESCC patients. Paraffin-embedded tissue for RNA extraction and quantification of miR-363 expression in addition to podoplanin protein were available for 29 ESCC patients and 19 EAC patients who received primary surgery.
Endoscopic biopsies were obtained during routine staging esophagogastroduodenoscopy prior to therapy. None of the patients had received prior radio- and /or chemotherapy. One hundred and six patients of the study population with an advanced tumor stage (cT3, Nx, M0) received preoperative chemoradiation. Briefly,cisplatin (20 mg/m2per day) was administered as a short-term infusion on days 1-5 and 5-fluorouracil (5-FU) (1000mg/m2per day) as a continuous infusion over 24 h on days 1-5. Radiation was delivered in daily fractions of 1.8 Gy to a total dose of 40 Gy using a multiple field technique. Standardized trans-thoracicen blocesophagectomy with 2-field lymphadenectomy was performed 4-5 wk after completion of chemoradiation.
Informed consent was obtained from each patient and the scientific protocol was approved by the local ethics committee.
Histopathologic response classification
The degree of histomorphologic regression of the primary tumor was classified into four categories (Cologne Regression Scale): Grade 1, complete response; Grade 2,nearly complete response with less than 10% vital residual tumor cells (VRTCs)classified as major response; Grade 3, 10% to 50% VRTCs; and Grade 4, more than 50% VRTCs, categorized as minor histomorphologic response[21]. Classification has been performed by experienced staff pathologists.
Immunohistochemistry
Podoplanin protein was detected by mouse anti-human D2-40 monoclonal antibody(DakoCytomation,Hamburg, Germany) raised against 40 kDa O-linked sialoglycoprotein. Paraffin embedded endoscopic biopsies and surgical specimens have been analyzed. Five µm sections were cut and deparaffinized according to standard histological techniques. A high sensitivity immunohistochemical staining was performed applying Dako EnVision System (DakoCytomation, Hamburg,) following the manufacturer’s instructions. In brief, sections were covered with citrate buffer (pH 6.0) for antigen retrieval. Endogenous peroxidase was blocked by 0.3% hydrogen peroxide for 20 min. Sections were covered by 100 μL mouse monoclonal D2-40 primary antibody (D2-40 mouse monoclonal antibody, Lot.Nr:10066658;DakoCytomation, Hamburg) at a dilution of 1:100 and incubated at 4°C overnight.The nuclei have been counterstained with hematoxylin. The staining procedure without a primary antibody was used as a negative control. For quantification of podoplanin expresson a scoring system was applied by a pathologist. Score 1: 0-5%tumor cells stained by D2-40 mab; Score 2: 6%-35% of tumor cells stained; Score 3:36%-65%; Score 4: > 65%.
miRNA isolation from paraffin-embedded tissue
Paraffin embedded resection specimen of EAC and ESCC have been selected from the Institute of Pathology, University Hospital of Cologne, Germany. Tissues were fixedin 10% buffered formalin prior to embedding in paraffin. Histological sections of 5-μm thickness were cut from each tissue block using a microtome. About 60 μm tissues per patient have been applied for total RNA extraction after macrodissection of the tumor area and purified by miRNeasy FFPE kit (Qiagen, Hilden), according to the protocol of the manufacturer. Samples have been lysed by Proteinase-K and treated with DNase-I. Concentrated RNA was purified using RNeasy MinElute spin columns and eluted by 12 μL of nuclease-free H2O.
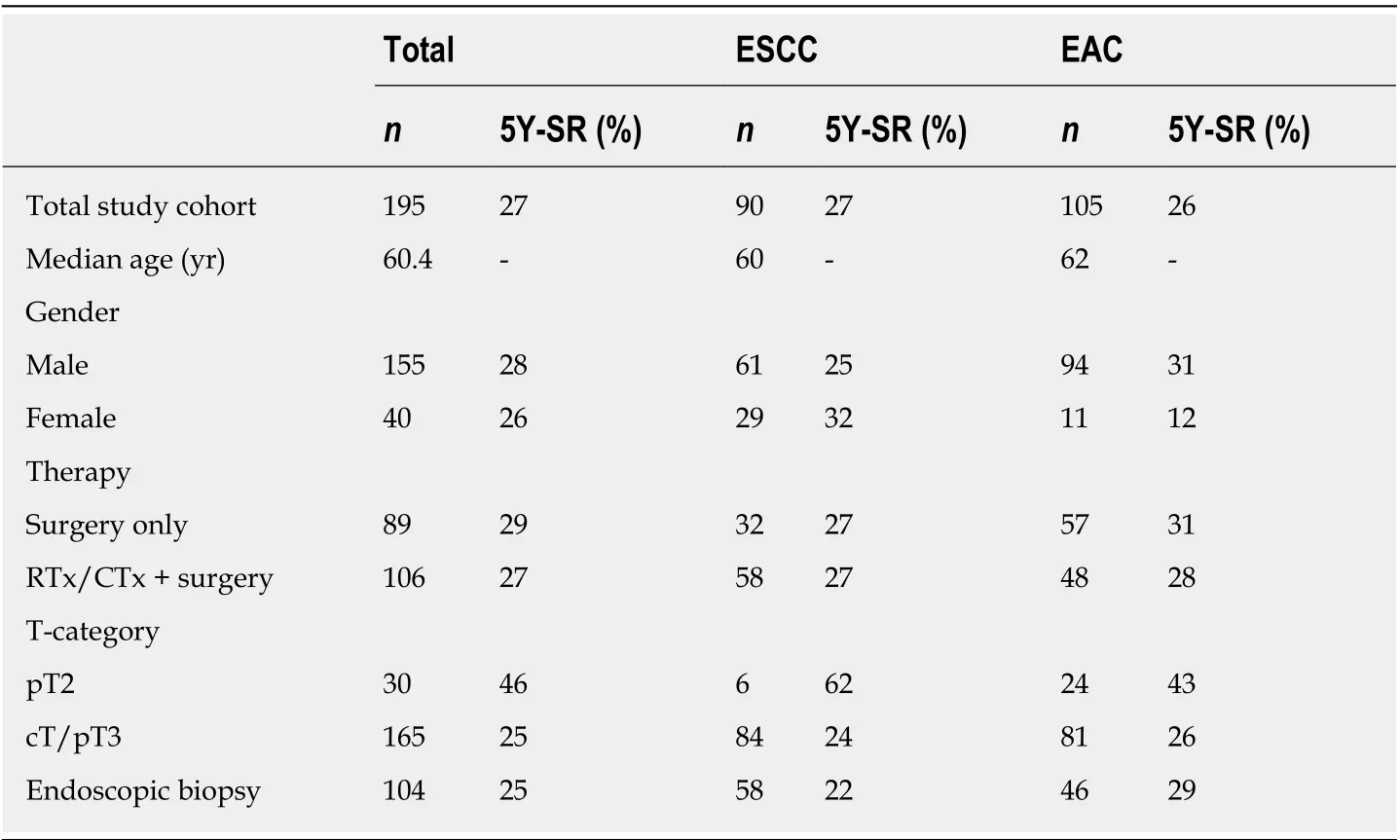
Table 1 Demographics, therapy and prognosis of esophageal cancer patients
miRNA reverse transcription and real-time PCR quantification
Reverse transcription of miR-363 from total RNA was performed using miR-363 specific reverse primer Assay-ID hsa-miR-363 001271 and TaqMan MicroRNA reverse transcription kit, Thermo Fisher Scientific, Darmstadt.
Quantification has been performed by TaqMan7900HT real-time PCR system Thermo Fisher Scientific, Darmstadt, RNU6 was used as a calibrator. The 15 μL RTreaction included 5 μL RNA, 3 μL reverse primer, 1 μL MultiScribe™ Reverse Transcriptase, 0.15 μL dNTP mixture, 0.19 μL RNase inhibitor, 1.5 μL RT-buffer, 4.16 μL nuclease-free H2O: 2 min 50 °C, 10 min 95 °C, 15 s 95 °C, and 1 min 60°C. TaqMan PCR analysis provided relative quantification of miR-363 expression related to expression of snoU6 as an endogenous control.
Statistical analysis
Fisher's exact test or Chi-Square test have been used to evaluate the correlation between scored podoplanin expression and histological tumor category (ESCCvsEAC). Significance of correlation between podoplanin expression and clinicopathological characteristics (pTNM-category), or different therapies was determined. Categorial data of paired samples has been compared by McNemer test.Survival curves based on post-therapeutic popdoplanin-expression in ESCC have been estimated according to Kaplan-Meier and compared with the Log-Rank test.
TaqMan PCR analysis provided relative quantification of miR-363 expression/expression of reference RNA snoU6. Receiver operating characteristic curve analysis has been used to define an optimal cut-off value for miR-363 in relation to podoplanin expression. Statistical calculations of prognosis were performed using MedCalc Statistical Software version 17.9.6 (MedCalc Software bvba, Ostend, Belgium);http://www.medcalc.org; 2017. Other statistical analyses were carried out using SPSS version 25 (Chicago, IL, United States).
RESULTS
Podoplanin expression in ESCC and EAC patients
Podoplanin staining of resected specimen derived from patients without preoperative chemoradiation revealed 56 of 57 EAC patients (98%) with none or nearly no protein expression (0-5%). 16 of 32 ESCC patients (50%) have been identified to express score 1 0-5% detectable protein. Comparision of podoplanin expression between ESCC and EAC,P< 0.001 is depicted in Table 2.
Different expression levels of podoplanin have been stained in EAC and ESCC patients in both, resected tissues of patients with primary surgery and endoscopic biopsies. One hundred and four endoscopic biopsies of 46 EAC and 58 ESCC patients confirmed podoplanin expression in ESCC, and its absence in EAC. Fourtyfour/fourty-six EAC patients (96%) were scored for expression of 0-5% protein compared to 36 of 58 ESCC patients (63%),P= 0.002, Table 2.
Podoplanin, a marker for tumor progression?
Podoplanin expression in resected tissues of 32 ESCC patients without chemoradiation did not show any significant relation to pT-category (P= 0.085,P=0.051 for pT2 to pT4) or lymph node metastases (P= 0.457), however, results are limited by the small number of patients in the subgroups (Table 3).
Podoplanin expression and prognosis
We analyzed a potential association of podoplanin expression and survival of ESCCpatients without preoperative chemotherapy. Patients with a stronger podoplanin protein expression > 5% [high podoplanin expression (HPE)] had a worse prognosis compared to the patient group with low expression (P= 0.013), Figure 1.
Sixteen patients showing a lower podoplanin expression of 0-5%, had a better survival rate of 34% than the patient group with HPE, resulting in a five-year survival of 12%.
Chemoradiation changes podoplanin protein expression
Fifty-eight ESCC and 48 EAC patients received preoperative chemoradiation therapy due to an advanced tumor stage (cT3NxM0).
Only one of these 48 EAC patients expressed HPE in resection specimen, 47 patients showed none or low expression. Staining of 57 primary surgery EAC patients provided the same result of absence of podoplanin, Table 2.
Seven of 58 ESCC patients expressed HPE in resected tissue after chemoradiation,51 patients had a lower expression < 5%. We compared the protein expression of this group of 58 ESCC patients who received chemoradiation to the non-pretreated primary surgery group of 32 ESCC patients. Podoplanin expression has been identified to be significantly lower in resected specimen of neoadjuvantly pre-treated patients compared to patients receiving only surgery,P< 0.001 (Table 4).
To confirm the different podoplanin expression levels between neoadjuvantly treated and non-pretreated primary surgery patient groups, we compared the protein expression in endoscopic biopsies with the expression after CTx/RTx of the individual matching resected tissue specimen of 56 ESCC patients.
Thirty-five pretreatment biopsies did not express podoplanin 0-5%, score 1. Thirtyfour of 35 neoadjuvantly treated patients (97%) did not express podoplanin in resected tissues. Twenty-one patients showed a higher podoplanin expression of > 5%(Score 2-4) in their biopsies before chemoradiation. In resection specimen of 16 of these 21 patients (76%) podoplanin was not detectable after neoadjuvant treatment.The matching resected specimen of these patients showed a decreased podoplanin expression after CTx/RTx,P< 0.001, examples in Figure 2, survey in Table 5.
Impact of podoplanin expression for prediction of response to neoadjuvant chemoradiation
There was no significant difference detectable in podoplanin expression between 35 minor and 23 majors responders among 58 ESCC patients (P= 0.879). Thirty-one of 35 minors responders showed a score 1, 4 of 35 Score 2 and 3 (> 5% podoplanin expression). Twenty-one of 23 majors responders showed Score 1, 2 of 23 Score 2.
Expression of miR-363 and podoplanin
To examine a potential role of miR-363 for post-transcriptional control of podoplanin up-regulation in ESCC, miR-363 expression has been quantified and compared to the expression level of podoplanin protein in resected tissues of 29 ESCC and 19 EAC patients - all patients without neoadjuvant therapy. There was no significant difference in miR-363 expression between EACn= 19 and ESCCn= 29 patient groups. miR-363 expression was not associated to histological tumor types. Median miRNA-363 expression was 8.4 (min-max: 1.05-303) in ESCC and 7.07 (min-max: 1.7-42.5) in EAC patients.
The association between miR-363 and podoplanin expression in the study group of ESCC patients without neoadjuvant treatment is shown as boxplots, Figure 3. An upregulated podoplanin expression has been detected to be associated with a lower miR-363 expression. Subgrouping of ESCC patients by podoplanin expression of 0-5% and HPE resulted in a trend of a correlation between expression of miR-363 and podoplanin protein: 0-5%n= 14: median miR-363 12.7 (min-max: 3.0-303), > 5%:n=15: median miR-363 6.1 (min-max: 1.05-131).
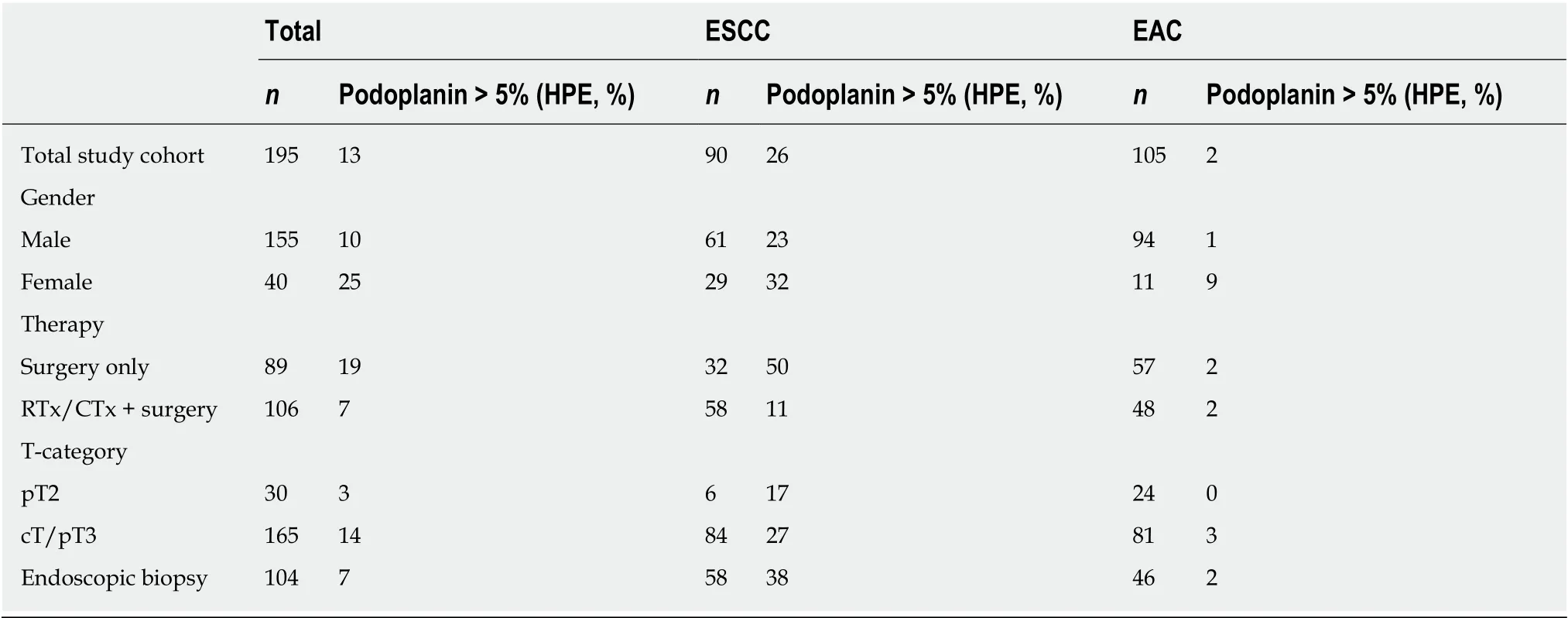
Table 2 Podoplanin expression in esophageal cancer squamous cell carcinoma of the esophagus vs adenocarcinoma of the esophagus
Patients with lower miR-363 expression had a worse prognosis compared to those with higher miR-363 expression. We identified a prognostic relevant cut-off value for miR-363. Patients without distant metastases with miR-363 expression < 7 (n= 10) had a significantly worse prognosis than patients with miR expression ≥ 7 (n= 16),P=0.049. (Figure 4). Based on this cut-off value for miR-363 expression of 7, the lower miR-363 expression (miR-363 < 7:n= 9) was associated with HPE (n= 15). Six of these 15 non-pretreated ESCC patients showed miR-363 expression ≥ 7 in resected tissue specimen. miR-363 expression ≥ 7 (n= 12) was associated with a low podoplanin expression of 0-5%n= 14, (P= 0.011). Only two of these 12 patients with low podoplanin expression expressed miR-363 < 7.
DISCUSSION
The histologically different tumor types EAC and ESCC depend on different risk factors, show biologically different characteristics, and respond with different rates to chemoradiotherapy[3,4]. Podoplanin expression is one example for the biological diversity between these most frequent histological subtypes of esophageal cancer. Our study confirms data of none to nearly no expression of the transmembrane protein podoplanin in EAC patients, and its expression in ESCC patients[22]. The oncofetal protein podoplanin has been described to be re-expressed in squamous cell carcinoma of other tumor entities, as well[23-25].
The most important result of our study is the change of podoplanin expression during neoadjuvant chemoradiation. This is a novel finding.
Our study has demonstrated a change of podoplanin protein expression after neoadjuvant treatment in resected tissue compared to pretreatment biopsies of the same individual patients. The comparison of resection specimen of a patient cohort neoadjuvantly pretreated with an only surgery study cohort provided the same result of lower podoplanin expression associated with chemoradiation.
The present study also revealed that podoplanin expression in pretreatment biopsies is not predictive for therapy response to chemoradiation. A low expression level did not seem to have the consequence of a major response, neither did a high podoplanin level with therapy resistance or minor response. Therefore, the thesis that podoplanin is expressed specifically by a differentiated tumor cell population with a stem cell like phenotype conferring therapy resistance as described by Lynam-Lennonet al[26]does not seem to be the fact for ESCC. There was no significant difference in podoplanin expression between 35 minor and 23 majors responding ESCC patients.Due to the changed podoplanin expression after neoadjuvant treatment this proteinmight rather be a target for therapy than a response predictive marker.
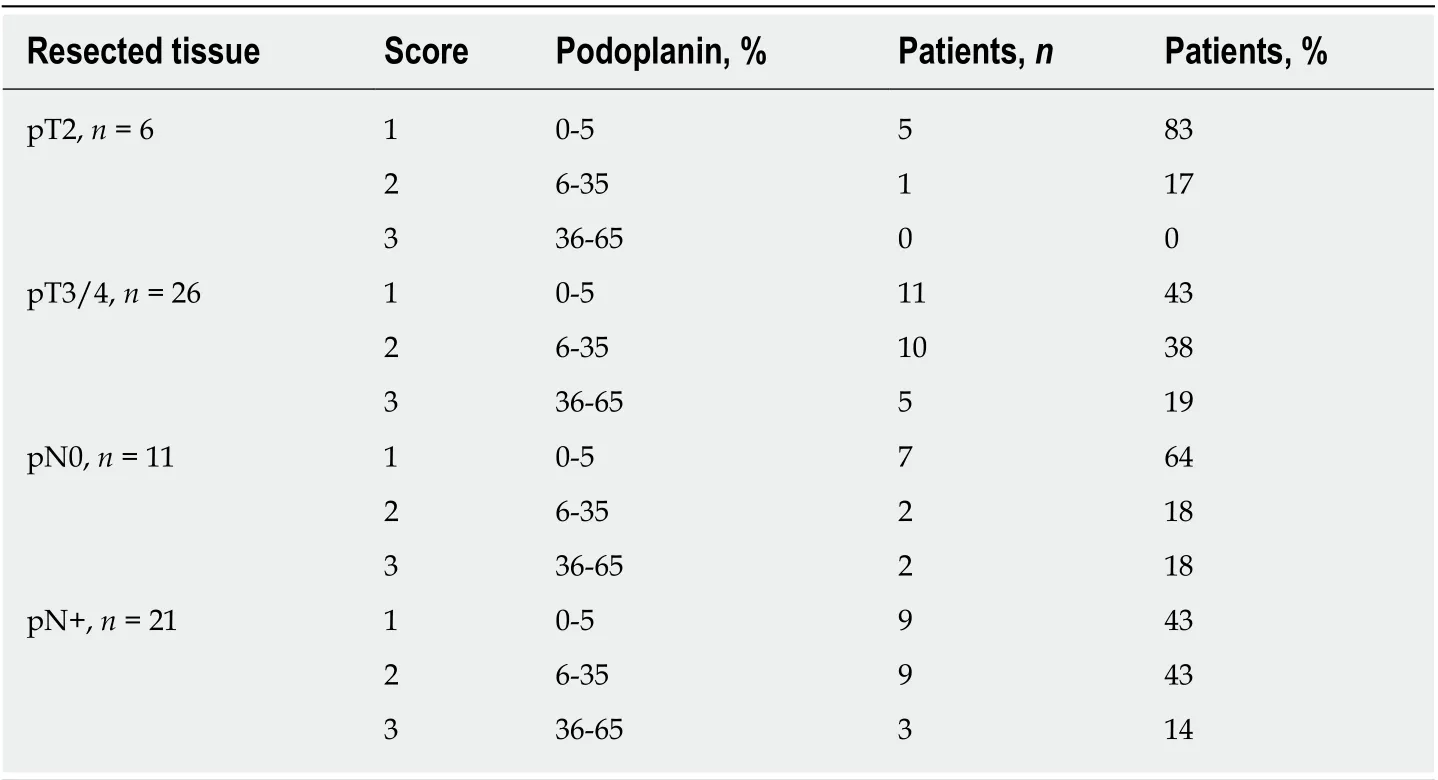
Table 3 Podoplanin expression and tumor progression
Upregulation of podoplanin expression was associated with ESCC. A reason for high podoplanin expression in squamous cell carcinoma in contrast to adenocarcinoma might be that podoplanin is expressed in some adult normal cells like lung alveolar cells, glomerular podocytes, as well as in basal epithelium of cervix and esophagus. ESCC develops from squamous epithelial cells, whereas in EAC these cells are replaced by columnar intestinal-type mucosa. EAC develops from Barrett esophagus[27].
Additionally, we were able to demonstrate high expression of podoplanin to be a marker for worse prognosis in accordance with data reviewed by Wanget al[22].Therefore, there may be a therapeutic effect by inhibiting this target. Monoclonal antibodies against podoplanin have already been produced for a potential targetbased therapy[28-30].
The biological function of podoplanin does support this therapeutic option.Podoplanin is a mucin-like transmembrane glycoprotein associated with cancer cell invasion and migration[31]and has been identified as a marker for early infiltrative carcinoma[27]. Podoplanin has been suggested to be involved in lymphangiogenesis,since podoplanin deficient mice had dilated malfunctioning lymphatic vessels and lymphedema[32]. The most studied physiological role of podoplanin is its ability to bind and activate the C-type lectin receptor (CLEC) that is highly expressed by platelets and immunocompetent cells[33,34]. Podoplanin has been identified as a key factor in tumor-induced platelet aggregation enhancing metastasis by secreting growth factors and forming tumor emboli in the microvasculature, reviewed by Hisadaet al[35]. Therefore, the podoplanin-mediated platelet aggregation might be an effective target for anti-tumor therapies. Platelet aggregation-inducing domains have been detected[15]. Aggregated platelets are coating tumor cells during their transit through the bloodstream, are mediating adherence to vascular endothelium, evasion from immune molecules and facilitate growth at metastatic sites. Podoplanin elicits platelet aggregation as the ligand of CLEC-2[36,37]. The strong upregulation of podoplanin expression supports its potential role as a therapeutic target reviewed by Takemotoet al[38]. An anti-human podoplanin antibody (NZ-1) inhibiting podoplanininduced platelet aggregation, abrogated experimental metastasis has already been formed, however with strong toxic side effects. A further novel chimeric humanized anti-human podoplanin antibody inhibiting podoplanin-induced platelet aggregation has been developed as a potential novel anticancer agent[39]. Since there is toxicity due to interferences with endogenous podoplanin in other cell types like type I lung alveolar cells, kidney podocytes, choroid plexus epithelium, a less interfering antigen has been developed[40]. However, the knowledge about the function of podoplanin in these organs is scarce.
Podoplanin has been reported to be involved in tumor progression[41]correlating with lymph node metastasis[42-46]. We were unable to demonstrate a significant association of podoplanin expression and T-category by staining of resection tissue of primary surgery patients, although a trend of a non-significant increase of podoplanin expression in T3 category compared to T2 has been observed. The lack of association between podoplanin expression and lymph node metastases might be due to the small number of patients in this subgroup, a weakness of our study.
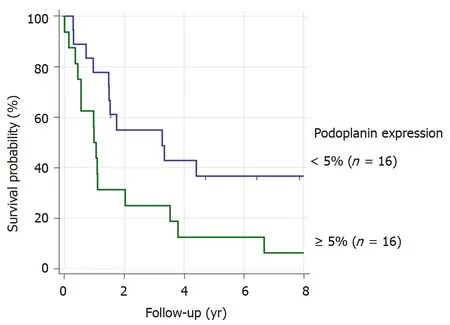
Figure 1 Podoplanin expression and prognosis of squamous cell carcinoma of the esophagus patients.Podoplanin expression in resected specimen of non-pretreated squamous cell carcinoma of the esophagus patients.
Despite this limitation we were able to detect an association of podoplanin expression with prognosis. Our data complements that of Tanakaet al[17]reporting on increased podoplanin expression as a predictor of mortality. Therefore, podoplanin could be applied as a prognostic marker for identification of patients with high risk for tumor progression.
Podoplanin represents an oncofetal antigen not expressed in most adult cells and re-expressed in squamous cell carcinoma. The transcriptional regulation of podoplanin expression has been reviewed by Astaritaet al[47]. Podoplanin transcription is regulated by AP-1 transcription factor comprised of Fos and Jun proteins. PTEN expression, a negative regulator of PI3K-AKT-AP-1 pathway, has inversely been correlated with podoplanin expression. The podoplanin promoter is heavily methylated keeping it repressed. Upregulation during malignant conditions seems to depend on the activity of Fos and Jun (AP-1) transcription factors. miRNAs are a major tool of posttranscriptional regulation. As a kind of master regulator these small molecules inhibit protein expression binding or degrading mRNAs[25].Circulating microRNAs have been associated with unfavorable response to neoadjuvant chemoradiotherapy[48]. A potential impact of post-transcriptional regulation of podoplanin protein expression by miR-363 has been described for head and neck squamous cell carcinoma[20]. Anti-proliferative properties have also been reported for miR-363[44], in gastric cancer[49]. We correlated miR-363 quantification with podoplanin protein expression and identified a cut-off value associated with a significant correlation. Patients with high miR-363 expression and down-regulated podoplanin expression had a better prognosis. This association and the potential role of miR-363 for up-regulation of podoplanin expression in ESCC also is a novel finding.
This is the first study showing a significant down-regulation of podoplanin protein expression during neoadjuvant chemoradiation in patients with ESCC. Podoplanin as well as its post-transcriptional regulator miR-363 might be important targets for a tailored therapy of locally advanced ESCC, as well as markers for prognosis.
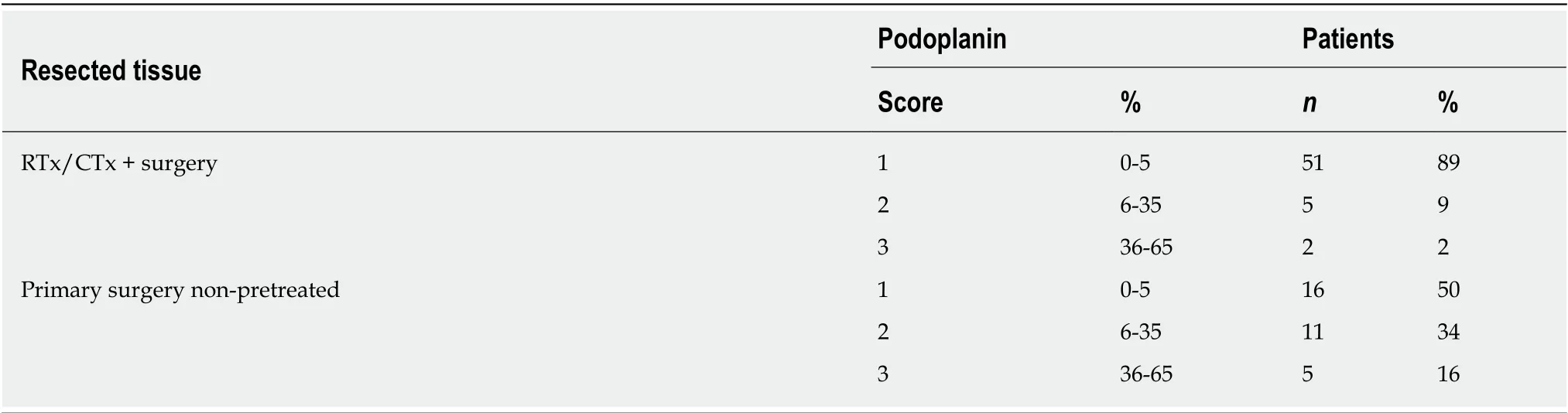
Table 4 Expression of podoplanin protein differs between tissues resected from neoadjuvantly treated and non-pretreated direct surgery squamous cell carcinoma of the esophagus patients
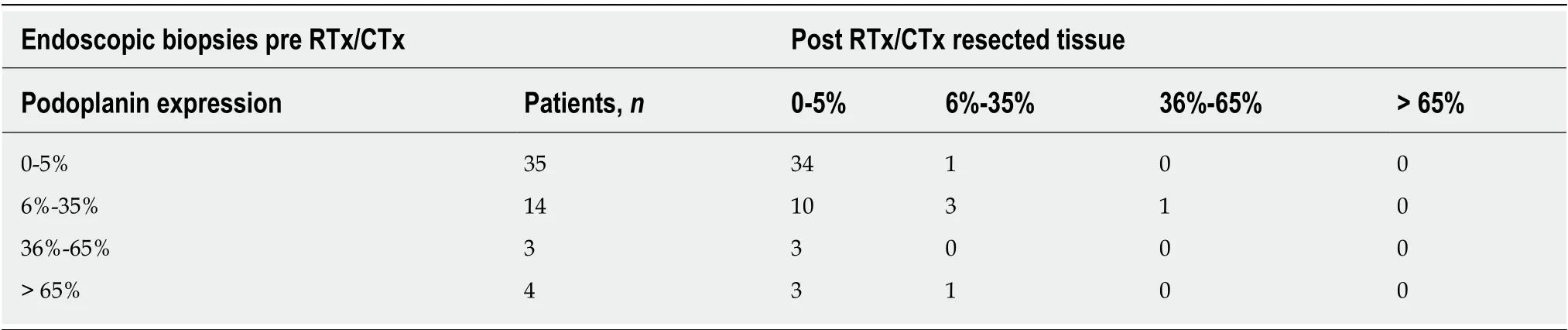
Table 5 Podoplanin expression pre- and post-neoadjuvant chemoradiaton
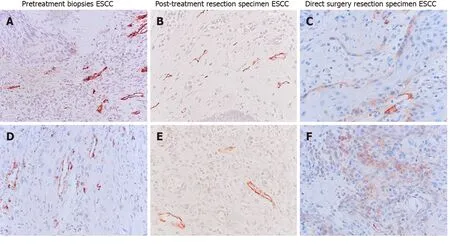
Figure 2 Podoplanin expression pre- and post-neoadjuvant treatment. A and D: Pre-treatment biopsies of two patients with podoplanin expression of scores: 3(A) and 2 (D); B and E: Matching resection specimen of the same squamous cell carcinoma of the esophagus (ESCC) patients after chemoradiation, Scores: 1 (B), 2(E); C and F: Resection specimen of two ESCC patients without neoadjuvant treatment, scores: 2 (C), 3 (F), at T-category 3; 40 ×. Score 1: 0-5% tumor cells stained by D2-40 mab, score 2: 6%-35%, score 3: 36%-65%. ESCC: Squamous cell carcinoma of the esophagus.
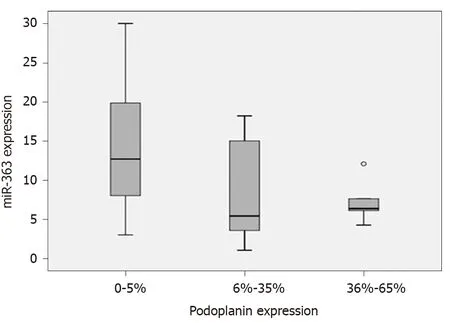
Figure 3 miR-363 and podoplanin expression for 29 non-pretreated squamous cell carcinoma of the esophagus patients. Relative miR-363 expression compared to immunohistochemically stained podoplanin protein expression in resected tissue specimen.
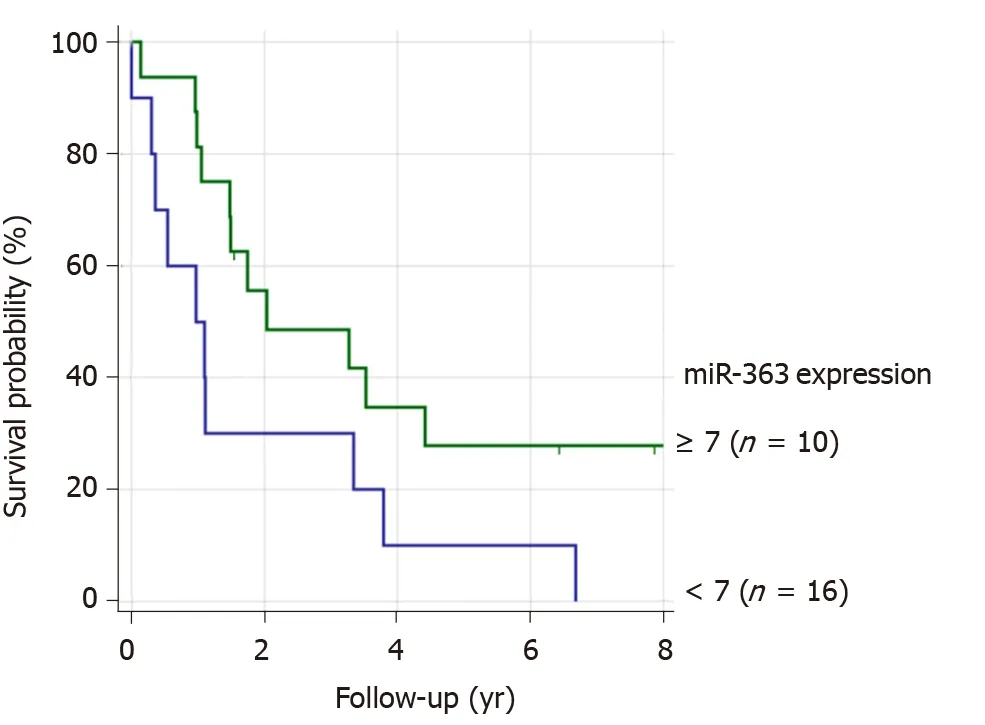
Figure 4 miR-363 expression and prognosis of 26 squamous cell carcinoma of the esophagus patients. Subgrouping by relative miR-363 expression < 7 and ≥7.
ARTICLE HIGHLIGHTS
We confirmed high podoplanin expression (HPE) in ESCC patients and its absence in EAC. We detected lower podoplanin expression in resection-specimen of 58 ESCC patients after neoadjuvant (RTx/CTx) treatment, only 11% with HPE of > 5%, compared to 32 non-pretreated primary surgery patients with 50% HPE,P= 0.0001. This novel finding of a lower podoplanin expression in the pretreated patient cohort was confirmed by the comparison of corresponding surgical specimens after neoadjuvant treatment with the individual matching pretherapeutic biopsies of 56 patients,P< 0.001. Podoplanin, however, is no predictive marker for response to neoadjuvant chemoradiation. Due to the small number of cT1-T2 patients we were only able to show a trend of association with podoplanin protein expression. We were able to demonstrate a prognostic impact of podoplanin, as well as for miR-336, a posttranscriptional regulator of this protein.
Research conclusions
Direct surgery ESCC patients with a low podoplanin expression have a better prognosis.Chemoradiation results in reduction of expression of podoplanin protein in patients with ESCC.Podoplanin expression seems to be, among others, controlled by miR-363.
Research perspectives
The decrease of podoplanin expression might become a therapeutic option.
ACKNOWLEDGEMENTS
We thank Michaela Heitmann, Susanne Neiss and Anke Wienand-Dorweiler for their excellent technical assistance.
 World Journal of Gastroenterology2020年23期
World Journal of Gastroenterology2020年23期
- World Journal of Gastroenterology的其它文章
- Liver-directed therapies for liver metastases from neuroendocrine neoplasms: Can laser ablation play any role?
- Potential of the ellagic acid-derived gut microbiota metabolite - Urolithin A in gastrointestinal protection
- Endosonographic diagnosis of advanced neoplasia in intraductal papillary mucinous neoplasms
- Medications in type-2 diabetics and their association with liver fibrosis
- Pancreatic necrosis and severity are independent risk factors for pancreatic endocrine insufficiency after acute pancreatitis: A long-term follow-up study
- Impact of a national basic skills in colonoscopy course on trainee performance: An interrupted time series analysis