
Recurrent thrombosis in the lower extremities after thrombectomy in a patient with polycythemia vera: A case report
2020-04-07 02:13BuPingJiangGuoBingChengQiangHuJiaWenWuXiaoYangLiShengLiaoSenYanWuWeiLu
World Journal of Clinical Cases 2020年24期
Bu-Ping Jiang, Guo-Bing Cheng, Qiang Hu, Jia-Wen Wu, Xiao-Yang Li, Sheng Liao, Sen-Yan Wu, Wei Lu
Bu-Ping Jiang, Guo-Bing Cheng, Qiang Hu, Jia-Wen Wu, Xiao-Yang Li, Sheng Liao, Sen-Yan Wu,Wei Lu, Department of Vascular Surgery, People’s Hospital of Quzhou, Quzhou 324000,Zhejiang Province, China
Abstract BACKGROUND Acute arterial embolism of the extremities is a surgical emergency. Atrial fibrillation is the major etiology of acute arterial embolism of the extremities.Emergency femoral artery thrombectomy can successfully treat this issue.However, polycythemia vera (PV) may sometimes explain this medical emergency. Recurrent thrombosis in the lower extremities after thrombectomy can be found in patients with PV, and reoperation is needed for this condition.CASE SUMMARY A 68-year-old man in China suffered from sudden pain in the left lower extremity for 14 h. The examination in the emergency department showed a diagnosis of acute arterial embolism of the extremities combined with PV. The patient’s complaint disappeared after repeat emergency thrombectomy.CONCLUSION Patients with acute arterial embolism of the extremities should be treated carefully, especially those who have recurrent thrombosis after emergency thrombectomy. Clinicians should be aware of PV, a rare cause of acute arterial embolism of the extremities. The combination of thrombectomy, phlebotomy, and antiplatelet and anticoagulant drugs may be a suitable therapeutic regimen for these patients.
Key Words: Thrombosis; Thrombectomy; Polycythemia vera; Case report
INTRODUCTION
Acute arterial embolism of the extremities is an emergent condition in the department of vascular surgery. Atrial fibrillation is the major etiology of acute arterial embolism of the extremities. Emergency femoral artery thrombectomy is the first-choice treatment. However, polycythemia vera (PV), a kind of myeloproliferative disease,may sometimes explain this medical emergency[1]. Recurrent thrombosis in the lower extremities after thrombectomy can be found in patients with PV. In this situation,reoperation is required. Here, we report an elderly man with PV who recovered from recurrent thrombosis in the lower extremities after thrombectomy. Related cases are seldomly described in the literature.
CASE PRESENTATION
Chief complaints
A 68-year-old man in China suffered from sudden pain in the left lower extremity for 14 h.
History of present illness
This patient presented a history of thrombectomy of the left femoral artery 17 years ago. Since then, his treatment has comprised an irregular course of cilostazol and beraprost sodium. He had no history of other vascular diseases, such as aortic aneurysm.
History of past illness
In addition, he had a history of hypertension for 7 years. During this period, he had taken irbesartan 150 mg and amlodipine besylate tablets 5 mg once a day. His blood pressure control status was unknown. He had no history of diabetes mellitus or coronary heart disease. This patient acknowledged smoking and drinking for 40 years but no drug allergies or blood transfusions.
Personal and family history
His family members had no records of vascular diseases.
Physical examination
The vital signs at emergency admission showed a normal temperature, heart rate, and breathing rate, but he had a blood pressure of 173/93 mmHg. The patient looked acutely ill. The numerical rating scale (NRS) score was one. Physical examination revealed accessible bilateral femoral artery pulsation and unavailable pulsation of the dorsal artery of the left foot and left posterior tibial artery. The skin temperature of the left lower extremity was cold.
Laboratory examinations
Relevant laboratory tests showed a hemoglobin level of 187 g/L, an erythrocyte count of 5.63 × 1012/L, a platelet count of 223 × 109/L, and a hematocrit value of 0.560.
Imaging examinations
Emergency double lower extremity vascular ultrasound revealed acute occlusion of the left superficial femoral artery and left posterior tibial artery (Figure 1A and B).
FINAL DIAGNOSIS
In this case, according to the patient’s complaint, physical examination, laboratory tests, and ultrasonography results, the diagnosis of acute arterial embolism of the lower extremities was obviously clear. For the differential diagnosis, acute arterial thrombosis of the lower extremities should be taken into account. A study pointed out that a history of previous arterial embolism and a normal peripheral pulse on the contralateral extremity can often be found in people with acute arterial embolism of the extremities, while those with acute arterial thrombosis of the lower extremities often have a history of intermittent claudication[2].
TREATMENT
Taking limb survival into consideration, an emergency operation was performed on February 29, 2020. We used local anesthesia around the left inguinal area. A 15-cmlong thrombus was removed by 3F and 4F catheters for thrombectomy (Figure 2A). On the first day after the operation, a routine blood test revealed a high hemoglobin of 178 g/L, an erythrocyte count of 5.39 × 1012/L, a platelet count of 232 × 109/L, and a hematocrit value of 0.535. Therefore, we invited the Department of Hematology for consultation. They suggested phlebotomy therapy, bone marrow puncture, and detection of related genes by bone marrow extraction and hematopoiesis. The results were positive for aJAK2 V617Fmutation. On March 6, 2020, this patient complained of pain in the left lower extremity with a NRS value of 3. An emergency double lower extremity vascular ultrasound was performed, showing occlusion of the left superficial femoral artery and posterior tibial artery (Figure 1C and D). Therefore, an urgent operation was carried out for the same purpose on March 6, 2020. A 10 cm long thrombus was completely removed (Figure 2B). On the first day after reoperation,routine blood tests revealed that hemoglobin was 168 g/L, erythrocyte was 5.03 × 1012/L, platelets were 193 × 109/L, and hematocrit was 0.500. On March 8, 2020, to avoid further emboli in the lower extremities, phlebotomy therapy was carried out. A total of 300 mL blood was released from his body. A routine blood test taken immediately was as follows: Hemoglobin 151 g/L, erythrocyte 4.59 × 1012/L, platelets 238 × 109/L, and hematocrit 0.450.
OUTCOME AND FOLLOW-UP
When he was discharged on March 20, 2020, his hemoglobin was 138 g/L, erythrocyte was 4.28 × 1012/L, platelet was 322 × 109/L, and hematocrit was 0.420, and both legs were warm. Two months later, he returned to our hospital for re-examination and presented a hemoglobin level of 143 g/L, an erythrocyte level of 4.77 × 1012/L, and a platelet level of 350 × 109/L with a hematocrit of 0.439 (Table 1). He temporarily refused, however, further examination of ultrasound and computed tomography angiography of lower extremity arteries. Until now, he took a regular course of 100 mg of aspirin and 10 mg of rivaroxaban every day, and no hemorrhage events happened during this course.
DISCUSSION
Generally, acute arterial embolism of the lower extremity is a common vascularsurgical condition. Atrial fibrillation is often believed to give rise to this complication[3]. Once diagnosed, surgery should be performed as soon as possible if the patient’s condition allows. When surgeons encounter these patients, emergency surgery must be carried out immediately within 6-8 h to rescue limbs on the verge of necrosis. A study revealed that patients may still benefit from surgery if the ischemia time of the extremities is no longer than 24 h[4]. However, recurrent arterial embolism caused by PV, a myeloproliferative disease, is rarely reported.

Table 1 A timeline of our patient
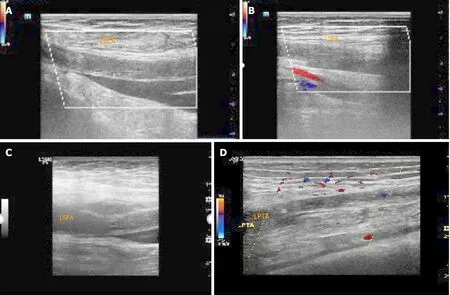
Figure 1 Ultrasonographic findings. A: Acute occlusion of the middle and upper segments of the left superficial femoral artery (LSFA); B: Formation of lateral branches in the lower segment of the LSFA; C: Second acute occlusion of the LSFA; D: Acute occlusion of the left posterior tibial artery. LPTA: Left posterior tibial artery; LSFA: Left superficial femoral artery.
PV is a typical kind of hematological system disease. Epidemiology shows that the morbidity of PV ranges from 1 to 40 persons per million people. The age at diagnosis is often older than 60 years[5]. Arterial embolism can be an initial symptom of PV[6]. These emboli can appear anywhere in the body, such as the brain, eyes, mesenteric vessels,and extremities. The most common site in the extremities is the common femoral artery[7]. Inpatient examination often reveals increased blood viscosity and a relevant mutant gene namedJAK2 V617F. From our point of view, this situation was very likely caused by the thickened blood, which is in accordance with Virchow’s triad. The National Comprehensive Cancer Network guidelines recommend phlebotomy as treatment for PV[8]. One study pointed out that the target hematocrit is less than 0.450 for phlebotomy in patients with PV[9]. Our treatment achieved this goal very well(Figure 3).

Figure 2 Thrombectomy photos. A: A 15-cm long thrombus was removed during the first thrombectomy; B: A 10-cm long thrombus was removed during the second thrombectomy.
This case is special in several aspects. First, acute arterial embolism of the extremities caused by PV is uncommon. Second, recurrent thrombosis in the lower extremities after thrombectomy in a patient with PV is seldom and rare. Notably, our center’s repeated thrombectomy procedure proved to be successful. Finally, in future clinical work, patients diagnosed with recurrent acute arterial embolism of the lower extremity should be vigilant against PV. If possible, routine consultations of the hematology department are necessary. Once diagnosed, the regular use of antiplatelet drugs, such as aspirin, is also important in patients with PV[10].
The limitations in this case were as follows: We did not invited the Department of Hematology for consultation before operation, and phlebotomy therapy was ignored during operation. We must avoid the same mistakes in our future clinical work.
CONCLUSION
Patients with acute arterial embolism of the extremities should be treated carefully,especially those who have recurrent thrombosis after emergency thrombectomy.Clinicians should be aware of PV, a rare cause of acute arterial embolism of the extremities. The combination of thrombectomy, phlebotomy, and antiplatelet and anticoagulant drugs may be a suitable therapeutic regimen for these patients.
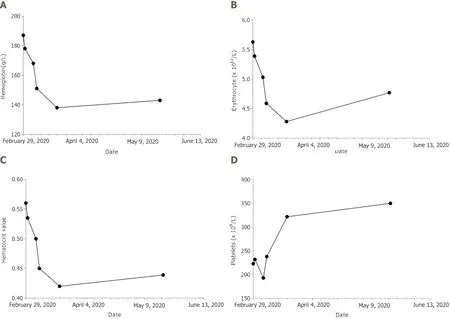
Figure 3 Change trends of relevant hematological indices during the perioperative period. A: Hemoglobin; B: Erythrocyte; C: Hematocrit value; D:Platelets.
ACKNOWLEDGEMENTS
We thank the colleagues, the platform, and the nursing team in our center.
 World Journal of Clinical Cases2020年24期
World Journal of Clinical Cases2020年24期
- World Journal of Clinical Cases的其它文章
- Role of gut microbiome in regulating the effectiveness of metformin in reducing colorectal cancer in type 2 diabetes
- lmpact factors of lymph node retrieval on survival in locally advanced rectal cancer with neoadjuvant therapy
- Three-year follow-up of Coats disease treated with conbercept and 532-nm laser photocoagulation
- Virus load and virus shedding of SARS-CoV-2 and their impact on patient outcomes
- Risk factors for de novo hepatitis B during solid cancer treatment
- Cause analysis and reoperation effect of failure and recurrence after epiblepharon correction in children