
Virus load and virus shedding of SARS-CoV-2 and their impact on patient outcomes
2020-04-07 02:13:00PeiFenChenXiaXiaYuYiPengLiuDiRenMinShenBingShengHuangJunLingGaoZhengYangHuangMingWuWeiYanWangLiChenXiaShiZhaoQingWangYingXiaLiuLeiLiuYongLiu
World Journal of Clinical Cases 2020年24期
Pei-Fen Chen, Xia-Xia Yu, Yi-Peng Liu, Di Ren, Min Shen, Bing-Sheng Huang, Jun-Ling Gao, Zheng-Yang Huang, Ming Wu, Wei-Yan Wang, Li Chen, Xia Shi, Zhao-Qing Wang, Ying-Xia Liu, Lei Liu, Yong Liu
Pei-Fen Chen, Yi-Peng Liu, Department of Respiratory Diseases, Shenzhen Key Laboratory of Pathogen and Immunity, National Clinical Research Center for Infectious Disease, State Key Discipline of Infectious Diseases, Shenzhen Third People’s Hospital, The Second Hospital Affiliated to Southern University of Science and Technology, Shenzhen 518114, Guangdong Province, China
Pei-Fen Chen, Department of Infectious Diseases, Linzhi People’s Hospital, Linzhi 860000,Tibet Autonomous Region, China
Xia-Xia Yu, Zheng-Yang Huang, School of Biomedical Engineering, Health Science Center,Shenzhen University, Shenzhen 518060, Guangdong Province, China
Di Ren, Expert Panel of Shenzhen 2019-nCoV Pneumonia, The Second People’s Hospital of Shenzhen, Shenzhen 518035, Guangdong Province, China
Min Shen, Wei-Yan Wang, Li Chen, Xia Shi, Zhao-Qing Wang, Ying-Xia Liu, Lei Liu, Shenzhen Key Laboratory of Pathogen and Immunity, National Clinical Research Center for Infectious Disease, State Key Discipline of Infectious Diseases, Shenzhen Third People’s Hospital, The Second Hospital Affiliated to Southern University of Science and Technology, Shenzhen 518114, Guangdong Province, China
Bing-Sheng Huang, Medical AI Laboratory, School of Biomedical Engineering, Health Science Centre, Shenzhen University, Shenzhen 518060, Guangdong Province, China
Jun-Ling Gao, Buddhism and Science Research Laboratory, Centre of Buddhist Studies, The University of Hong Kong, Pokfulam, Hong Kong 999077, China
Ming Wu, ICU, The Second People's Hospital of Shenzhen, Shenzhen 518035, Guangdong Province, China
Yong Liu, Expert Panel of Shenzhen 2019-nCoV Pneumonia, Shenzhen Hospital, Southern Medical University, Shenzhen 518000, Guangdong Province, China
Abstract BACKGROUND Understanding a virus shedding patterns in body fluids/secretions is important to determine the samples to be used for diagnosis and to formulate infection control measures.AIM To investigate the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)shedding patterns and its risk factors.METHODS All laboratory-confirmed coronavirus disease 2019 patients with complete medical records admitted to the Shenzhen Third People’s Hospital from January 28, 2020 to March 8, 2020 were included. Among 145 patients (54.5% males;median age, 46.1 years), three (2.1%) died. The bronco-alveolar lavage fluid(BALF) had the highest virus load compared with the other samples. The viral load peaked at admission (3.3 × 108 copies) and sharply decreased 10 d after admission.RESULTS The viral load was associated with prolonged intensive care unit (ICU) duration.Patients in the ICU had significantly longer shedding time compared to those in the wards (P < 0.0001). Age > 60 years [hazard ratio (HR) = 0.6; 95% confidence interval (CI): 0.4-0.9] was an independent risk factor for SARS-CoV-2 shedding,while chloroquine (HR = 22.8; 95%CI: 2.3-224.6) was a protective factor.CONCLUSION BALF had the highest SARS-CoV-2 load. Elderly patients had higher virus loads,which was associated with a prolonged ICU stay. Chloroquine was associated with shorter shedding duration and increased the chance of viral negativity.
Key Words: COVID-19; Virus shedding; Viral load; Patient outcome; China; Infectious disease
lNTRODUCTlON
The coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a novel coronavirus that is closely related to SARS-CoV, which caused an outbreak in 2003[1]. The outbreak of COVID-19 was first reported in December 2019 in Wuhan, China[2,3]. Such outbreak can cause emotional distress and anxiety[4], which can occur even in people not at high risk of getting sick,in the face of a virus that the common people are unfamiliar with[4]. The common signs of COVID-19 include fever, cough, and shortness of breath[5]. While a significant proportion of patients develop neurological manifestations, especially olfactory and gustatory dysfunction[6,7]. There is no specific treatment, but supportive care is necessary in severe and critical cases[5,8]. Acute respiratory distress syndrome and sepsis were reported in 100% of the patients with confirmed COVID-19 who died[9].
The factors dictating the severity of illness and outcome among patients with COVID-19 are still not well defined. Observational studies reported that the median duration of viral shedding was 20.0 d (IQR: 17.0-24.0) among survivors[10,11]. In some other coronavirus respiratory illnesses, the higher virus load and longer shedding duration were related to a worse outcome[12-14]. The longest observed duration of viral shedding in survivors was 37 d[11]. The viral shedding duration among patients with COVID-19 has been reported to be associated with age and comorbidities[2,9].Prolonged Middle East respiratory syndrome (MERS) viral shedding in the respiratory tract was associated with severe outcomes in patients with MERS[15,16]. In addition,studies suggested that patients with MERS-CoV requiring intensive care unit (ICU)admission had a higher viral load than the patients not requiring ICU admission[17].Nevertheless, whether the virus load and shedding duration of SARS-CoV-2 are associated with the severity of illness is still unknown.
Data on viral load and shedding in the respiratory tract are limited, and risk factors for viral shedding have yet to be fully clarified. COVID-19 has proven to be highly infectious and is transmitted person-to-person[5]. Respiratory droplets were suspected to be the main route of transmission for SARS-CoV[12]and SARS-CoV-2[5]. Aerosols and fomite are possible transmission routes since SARS-CoV-2 survives for 0.8-6.8 h on different surfaces[18]. It is of great epidemic significance to understand the virus shedding patterns in different body fluids and secretions to determine which samples are the most suitable for diagnosis, and how to formulate appropriate infection control measures and isolation duration. Most importantly, virus shedding could be used as a reliable marker to scrutinize the effectiveness of antiviral drugs.
This study aimed to examine the distribution of COVID-19 virus in the tissues of the patients and the shedding pattern of COVID-19 virus in the respiratory secretions and to investigate potential factors associated with viral load and shedding and patient outcomes.
MATERlALS AND METHODS
Viral loads and cycle threshold value for SARS-CoV-2 virus
A cycle threshold value (Ct value) < 37 was defined as a positive test, and a Ct value of≥ 40 was defined as a negative test. A medium load, defined as a Ct value ≥ 37 but <40, required retesting. By regression analysis of the standard curves provided by the manufacture (Shanghai Jienuo Co., Ltd., Shanghai, China) (Supplementary Figure 1),the following equations of the standard curve (plot of Ct values against the log of the standard sample amount) were determined for SARS-CoV-2 (R² = 0.995): Ct = -3.39 ×log(copies) + 40.52.
Data collection
The following data were extracted from the medical records: Demographics (age, sex,body mass index, history of Hubei contact, and smoking), symptoms (at admission and in the ICU), comorbidities (hypertension, diabetes, heart diseases, and chronic obstructive pulmonary disease), laboratory findings at admission (temperature, white blood cells, platelets, lymphocytes, interleukin (IL)-6, serum creatinine, respiratory tract viral load, and PaO2/FiO2), severity scores [Acute Physiology And Chronic Health Evaluation II (APACHEII), Sequential Organ Failure Assessment (SOFA), and Glasgow Coma Scale (GCS)], therapy, outcomes (viral shedding, ICU stay, hospital stay, death, and discharge).
Statistical analysis
Continuous variables are presented as mean values with 95% confidence intervals (CI).The means for continuous variables were compared using the independentttest when the data were normally distributed (Kolmogorov-Smirnov test); otherwise, the Mann-WhitneyU-test was used. Data with non-Gaussian distribution from repeated measures were compared using the generalized linear mixed model. The proportions for categorical variables were compared using theχ-square test, while the Fisher’s exact test was used when the data were limited. Multivariable regression analysis or time-dependent Cox regression was conducted to assess the relative influence of virus shedding on ICU admission and hospital duration.Pvalues ≤ 0.05 were considered statistically significant. All analyses were performed using R (http://www.Rproject.org) and EmpowerStats software (www.empowerstats.com, X&Y solutions,Inc. Boston, MA, United States).
RESULTS
Data collection and patients
All consecutive patients with confirmed COVID-19 admitted to the Shenzhen Third People’s Hospital from January 28, 2020 to March 8, 2020, were screened for eligibility.The Shenzhen Third People’s Hospital is the only designated infectious disease hospital responsible for the treatments of COVID-19 in Shenzhen, China. This retrospective study was approved by the Institutional Review Board of Shenzhen Third People’s Hospital. Informed written consent was obtained from all subjects prior to the study.
All patients with COVID-19 included in this study were diagnosed according to World Health Organization interim guidance[19]. The hospitalized patients with more than one positive nucleic acid test for SARS-CoV-2 virus at least one day apart and with complete medical records were included in the analysis. To investigate the possible transmission capacity, the specimens were obtained from a variety of sources,including sputum, nasopharyngeal swabs, blood, endotracheal aspirate, saliva, and eye discharges.
Characteristics of the specimens
The study initially screened 1461 patients, and 111 were excluded for missing virological records (Figure 1). Among those 1350 patients with COVID-19, 7404 virological tests were performed. Of 6959 (94.0%) nasopharyngeal swab specimens,41.6% were positive for COVID-19. Among 144 (1.9%) blood samples, 14.6% showed positive results. Among 213 (2.9%) bronchoalveolar lavage fluid (BALF) specimens,56.3% were positive. Among 47 (0.6%) saliva samples, 29.8% were positive. Among 38(0.5%) eye discharge samples, 15.8% were positive. In addition, two cerebrospinal fluid(CSF, 0.03%) samples were available, and both were negative. One (0.01%) anus swab sample was negative for COVID-19 (Supplementary Table 1).
Characteristics of the patients
The patients with incomplete medical records were excluded, and 145 patients with full inpatient records were included (Figure 1). Among them, 79 (54.28%) were males,and the mean age was 46.1 (95%CI: 42.6-49.9) years. Of these patients, 107 (73.8%) were admitted to the isolation wards, and 38 (26.2%) were admitted and transferred to the ICU. The median duration from the first symptoms to hospital admission was 4.6 d(95%CI: 4.1-5.1 d) (Table 1). Hypertension [26 (17.9%)], cardiovascular disease [18(12.4%)], and diabetes [11 (7.6%)] were the most common comorbidities. During the first 3 d after admission, 142 were treated with interferon, 16 (11.0%) received no antiretrovirals (ARV), while 84 (57.9%) received one ARV, 38 (26.2%) received two ARVs, and seven (4.8%) received three ARVs.
The next day the whole family was busy cooking and straightening up the house for Christmas Day, wrapping last-minute presents and trying hard not to burst with excitement. But even with all the activity and eagerness, a flurry of new straws piled up in the crib, and by nightfall it was overflowing. At different times while passing by, each member of the family, big and small, would pause and look at the wonderful pile for a moment, then smile before going on. It was almost time for the tiny crib to be used. But was it soft enough? One straw might still make a difference.
In 92 (63.5%) patients, viral negativization took longer than 2 wk. These patients were older (50.3vs39.6 years) and were more likely to have hypertension and heart diseases compared with patients who achieved viral negativization in less than 2 wk(Table 1). In addition, they had lower platelet and higher IL-6 and serum creatinine levels. Their conditions were more severe, with higher SOFA and APACHEII scores.
Virus load in different sample types
The mean viral load at admission for the 145 patients was 1.16 × 104copies/mL (26.7 ±4.4 in Ct values), but it could reach 11.7 in Ct value (3.3 × 108copies/mL). The mean viral load in the respiratory tract was 4.9 × 103copies/mL. The median viral load in nasopharyngeal swab samples was 1.32 × 104copies/mL (26.6 ± 4.4 in Ct value); from sputum samples, it was 2.9 × 102copies/mL (32.2 in Ct value); from BALF it was 5.7 ×104copies/mL (24.5 ± 3.6 in Ct value); and from blood samples, it was 4.2 × 103copies/mL (28.2 ± 7.4 in Ct value) (Supplementary Figure 1). The BALF had the highest virus load compared with the other samples.
Association between virus load and disease severity
The patients in the ICU had higher virus loads than those in wards. The average Ctvalues were 2.0 × 104copies/mL (25.9 ± 4.0 in Ct value) and 6.8 × 103copies/mL (27.5 ±4.7 in Ct value) for 38 patients in the ICU and for 107 patients in wards, respectively.The Ct values for patients with longer ICU stay (≥ 7 d) were significantly lower than those with shorter ICU stay (< 7 d,P= 0.02) (Figure 2A). Of those patients who survived, the Ct values were significantly higher compared with those who died (P<0.0001) (Figure 2B). In addition, patients with mechanical ventilation had lower Ct values at admission compared to those without mechanical ventilation (P= 0.004)(Figure 2C). Moreover, patients with IL-6 > 30 μg/L had higher Ct values compared to those with IL-6 < 30 ug/L (P= 0.05) (Figure 2D). The average Ct values did not significantly differ in terms of comorbidities, sex, and Hubei contact (allP> 0.05).
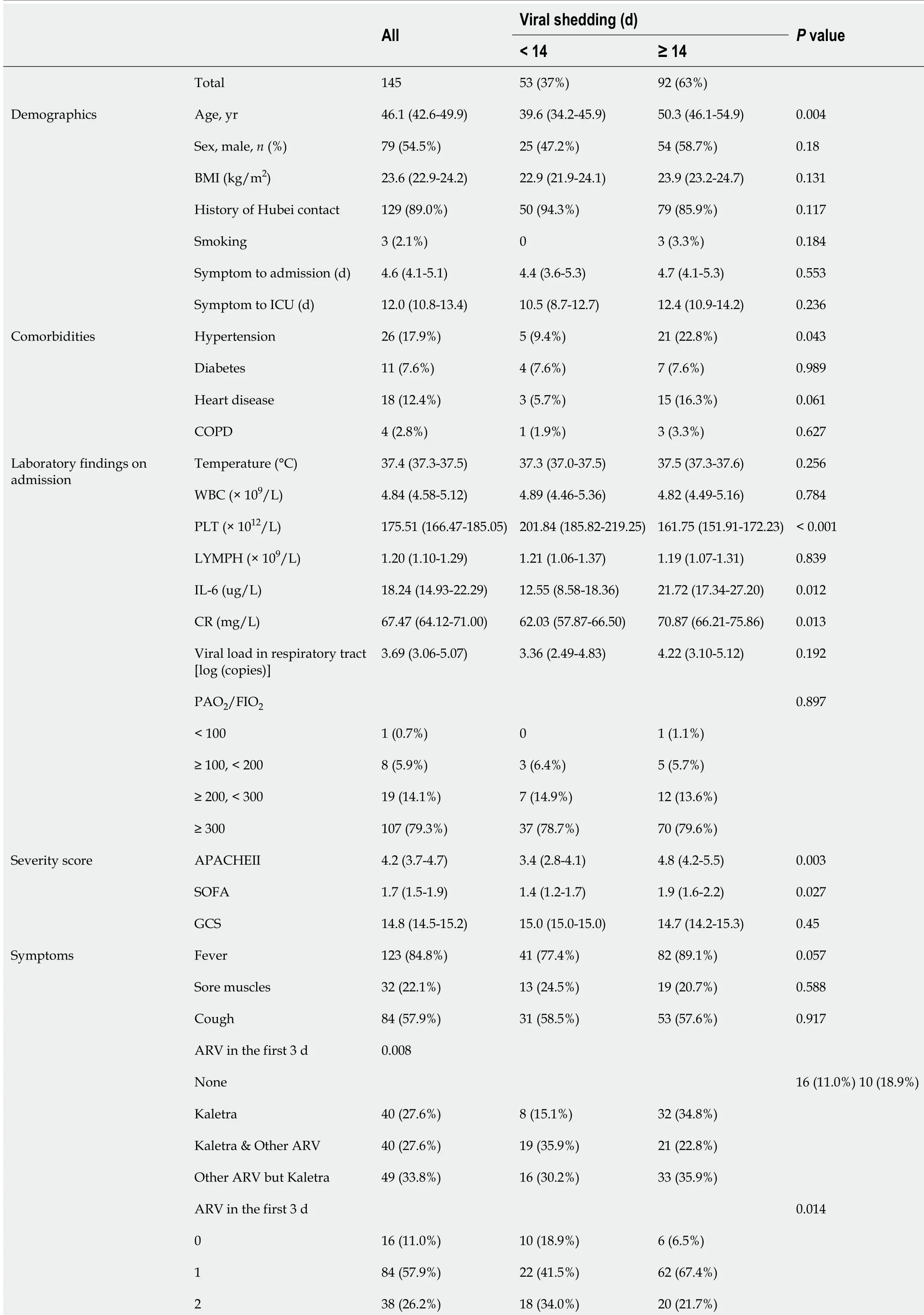
Table 1 Characteristics and outcomes of the patients
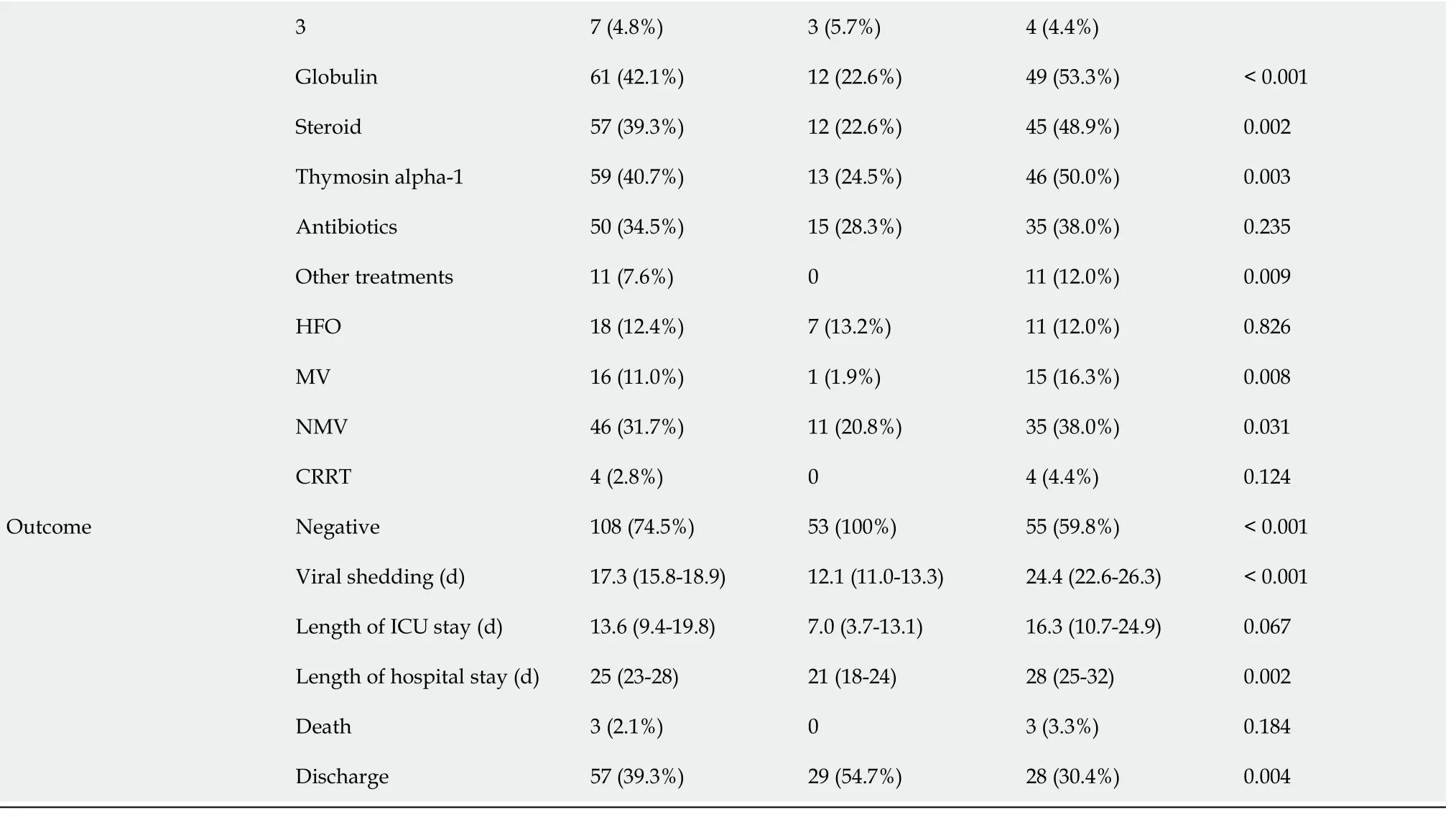
Continuous variables were described by mean values with 95% confidence intervals, while categorical variables were presented using percentages. BMI:Body mass index; ICU: Intensive care unit; WBC: White blood count; PLT: Platelet; LYMPH: Lymphocyte; IL-6: Interleukin 6; CR: Serum creatinine;APACHEII: Acute Physiology And Chronic Health Evaluation II; SOFA: The Sequential Organ Failure Assessment; GCS: Glasgow Coma Scale; COPD:Chronic obstructive pulmonary disease; ARV: Antiretroviral therapy; HFO: High flow oxygen; MV: Mechanic ventilation; NMV: Non-invasive ventilation;CRRT: Continuous Renal Replacement Therapy.
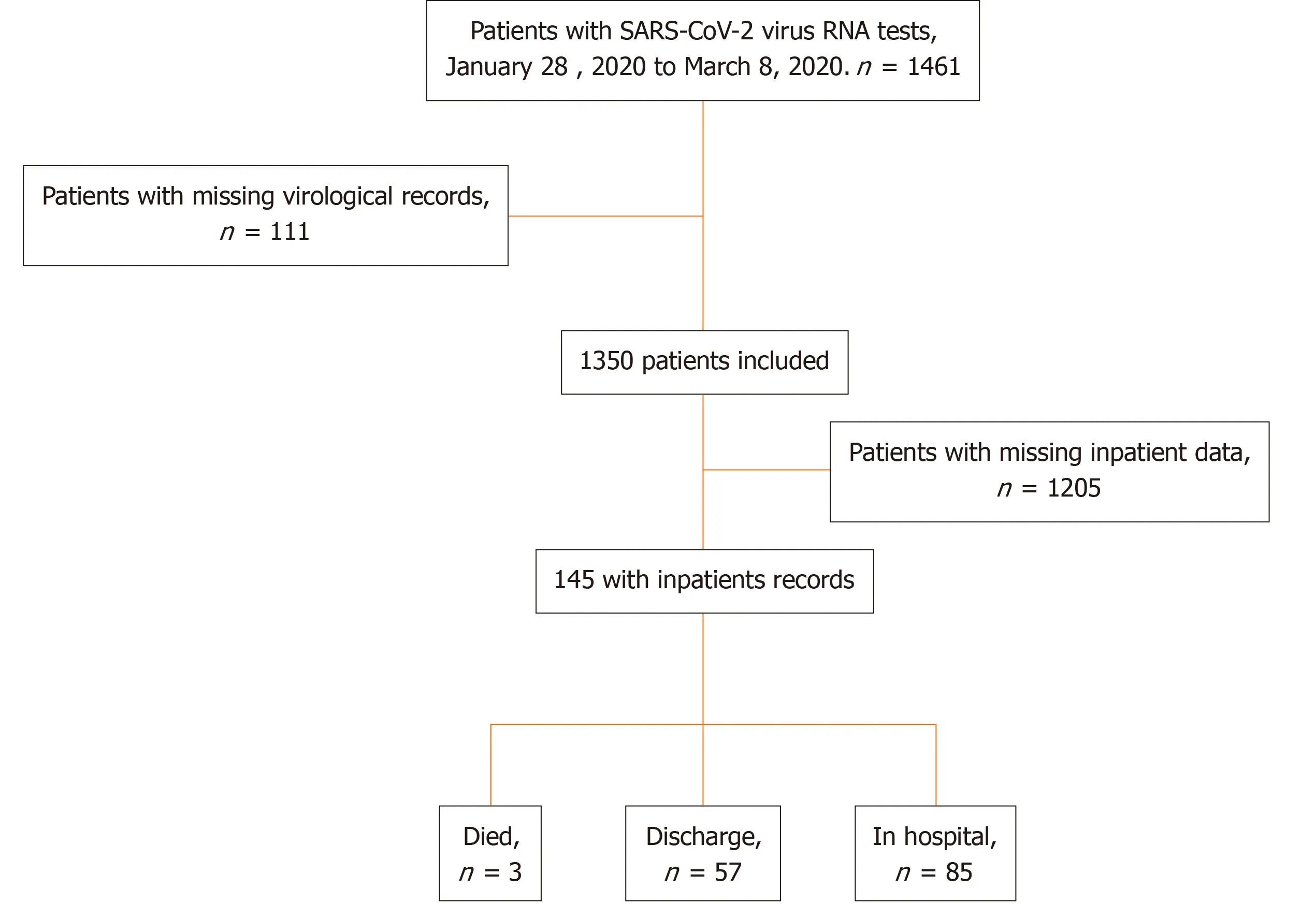
Figure 1 Patient flowchart. SARS-Cov-2: Severe acute respiratory syndrome coronavirus 2.
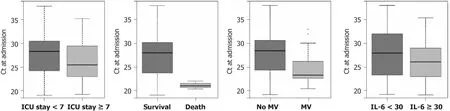
Figure 2 Box plot showing the cycle threshold value differences at the day of hospital admission. A: Duration of intensive care unit stay (< 7 vs ≥7 d) (one-sided t test, P = 0.02); B: Vital status (death or not) (one-sided t test, P < 0.0001); C: Procedures (mechanical ventilation needed or not) (one-sided t test, P= 0.009); D: Results at admission (interleukin 6) (one-sided t test, P = 0.05). Ct: Cycle threshold; MV: Mechanic ventilation; IL-6; Interleukin 6; ICU: Intensive care unit.
Duration of SARS-CoV-2 viral shedding
The average duration of SARS-CoV-2 viral shedding was 17.3 d (95%CI: 15.8-18.9 d).For the ward patients, the average duration of SARS-CoV-2 viral shedding was 12.1 d(95%CI: 11.0-13.3 d), while for the ICU patients, it was 24.4 d (95%CI: 22.6-26.3 d) (P<0.0001). Patients with lower first positive Ct values tended to have longer viral shedding time (P= 0.0176).
Smooth curves were fitted for Ct value and the illness onset to hospital admission(Figure 3A). Virus load peaked at admission and sharply decreased within 10 d after admission, after which it gradually dropped until reaching a low level or negativization. Moreover, the results also indicated the longer the time from symptom to hospital admission, the longer was the duration of viral shedding (Figure 3C). We further compared the proportion of patients who tested positive for SARS-CoV-2 RNA over time after admission, and significant differences were seen in the duration of viral shedding for the elderly population (Figure 3B), patients with PaO2/FiO2< 100(Figure 3D), and chloroquine prescribed within 3 d after admission (Figure 3E).
Risk factors for prolonged viral shedding
All available data from 145 patients were incorporated in a time-dependent Cox proportional hazards model. Chloroquine was positively correlated with virus shedding, increasing the possibility of viral shedding. Age > 60 years was negatively correlated with viral shedding and could potentially decrease the chance of viral shedding and was thus associated with longer shedding duration. Age > 60 years[hazard ratio (HR) = 0.6; 95%CI: 0.4-0.9] was an independent risk factor for SARS-CoV-2 shedding, while chloroquine (HR = 22.8; 95%CI: 2.3-224.6) was a protective factor(Table 2); immunoglobulin, antibiotics, steroid, PaO2/FiO2ratio, and the neutrophillymphocyte ratio were not independently associated with virus shedding (Table 2).Viral shedding was associated with longer ICU duration, but not with hospital stay and in-hospital mortality (Table 3).
DlSCUSSlON
SARS-CoV-2 was detected in samples from eye discharge, blood, saliva, nose swab,and BALF. Although the SARS-CoV-2 virus is mainly distributed in the respiratory system, it can also be found in the digestive tract, blood, and eye discharge, which may contribute to the high contagious capacity of the virus[20]. In the present study, SARSCoV-2 was detected in the nasopharyngeal swab, blood, BALF, saliva, and eye discharge. It was not found in the CSF and anus swab, but these two sample typeswere too few to draw a conclusion.
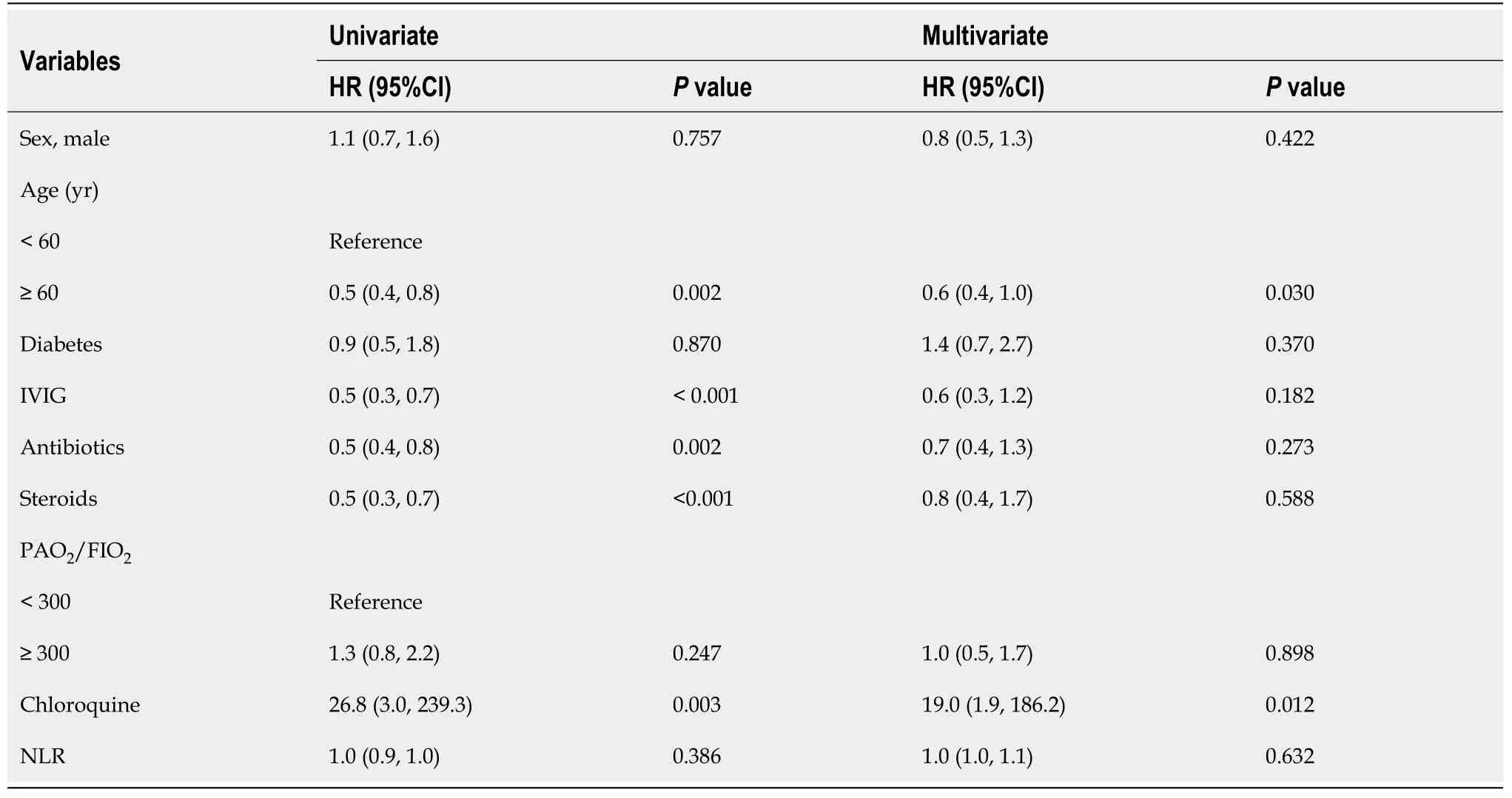
Table 2 Univariate and multivariate regression analyses of the risk factors for viral shedding

Table 3 lmpact of severe acute respiratory syndrome coronavirus 2 viral shedding on outcomes
The shedding pattern of SARS-CoV-2 RNA demonstrated that the virus load increased sharply before admission and dropped dramatically thereafter. Based on the samples collected from 145 patients, the mean virus load at admission was 1.16 × 104copies/mL, which is basically similar to SARS[12], instead of 1000 times higher, as reported[21], and the highest viral load was 3.3 × 108copies/mL according to the previous research[21]. Moreover, the present study suggested that the viral load peaked at admission, decreased right after the start of treatment, decreased sharply within 10 d after admission, and dropped gradually until reaching a quite low level or negativization. In addition, the mean duration of SARS-CoV-2 viral shedding was much longer in ICU patients compared to those in the wards (21.8vs.14.8 d). The shedding duration of SARS-CoV-2 RNA was reported to be considerably longer than that of MERS and SARS[15,22]. Moreover, the duration of virus shedding was influenced by the time between the onset of illness and admission, where a later admission was associated with longer virus shedding, higher ICU admission, and lower survival probability. Those data suggest that the early detection and clinical intervention would help shorten the viral shedding duration, lower the risk of ICU admission, and increase the survival probability.
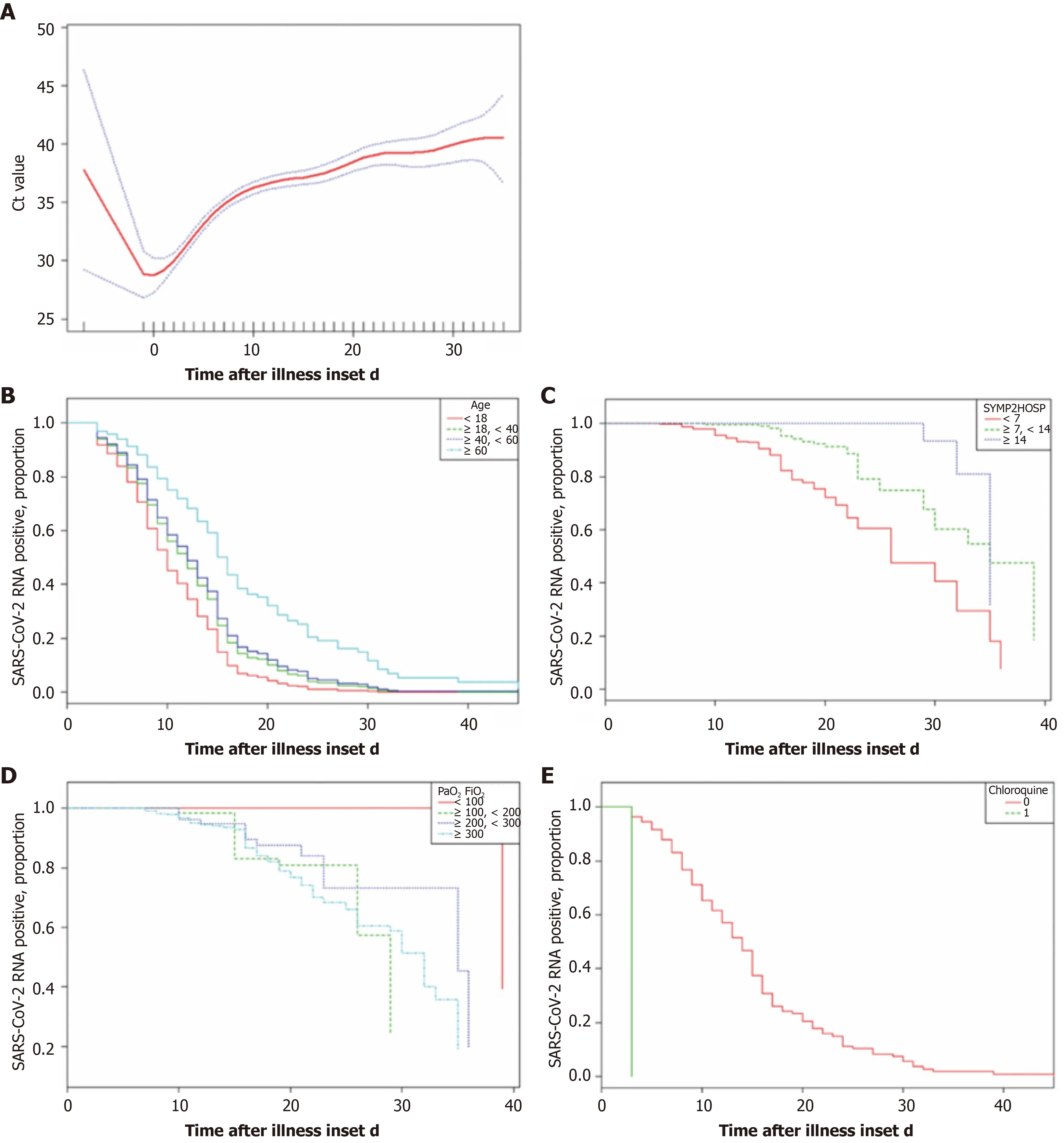
Figure 3 Factors associated with the duration of viral shedding. A: Changes in cycle threshold values during hospitalization using generalized additive models (F: 46.54, P < 0.0001, adjusted for sex and age); B: From symptom onset to hospital admission (χ2: 85.31, P < 0.0001); C: Cumulative proportions of patients with symptom onset to admission < 7 d, 7-14 d, and > 14 d (χ2 = 76.58, P < 0.001); D: Cumulative proportions of patients with PaO2/FiO2 < 100, 100-200, > 200 (χ2 =53.74, P < 0.0001) at admission; E: Cumulative proportion of patients with chloroquine or without (P < 0.0001). Ct: Cycle threshold; SARS-Cov-2: Severe acute respiratory syndrome coronavirus 2.
This study suggested that senior age was an independent risk factor for virus shedding. Previous research suggested that advanced age is associated with prolonged illness and poor outcomes in patients hospitalized with COVID-19[23-25]. The present study further demonstrated that the elderly had higher initial viral loads in contrast to younger patients. A higher viral load may reflect a disability of the immune system to contain viral proliferation, thus contributing to the prolonged viral shedding period.Another independent risk factor was the use of chloroquine within 3 d after admission. The interim conclusions from the published literature is that there is no current evidence of use of chloroquine for treatment of COVID-19. Chloroquine should be restricted to clinical trials with strict vigilance and follow-up[26]. The results in the present study indicated that chloroquine could greatly increase the probability of viral negativity by 19.0 times while shortening the virus shedding duration. This finding is consistent with previous publications[5,27]. Nevertheless, due to the limitation of observational studies, randomized clinical trials are necessary before any definitive conclusions on the effectiveness of chloroquine can be reached.
The effectiveness of several clinical treatments was also examined. Contrary to the intuitive experience, the present study suggests that immunomodulation, such as thymosin and intravenous immunoglobulin (IVIG), had no impact on the pattern of virus shedding. This effect has been explored in other researches, and the studies for IVIG were inconclusive due to potential confounding effects of patient comorbidities,stage of illness, or effect of other treatments[28,29]. Our findings suggest that immunomodulation treatment might not reduce the shedding duration after adjusting for the confounding factors. Similar findings were observed about the effect of antivirus treatment. Kaletra, a combination of lopinavir and ritonavir for human immunodeficiency virus treatment, has shown efficacy in a case report in China[25], but after adjusting for the confounding factors, it was not superior to ribavirin plus interferon. It is also true for the other antiviral drugs. Thus, any wide administration of this antiviral treatment (AVT) should be carefully evaluated by randomized clinical trials.
This study has some limitations. First, due to the retrospective study design, not all comorbidities were well documented in all patients. Therefore, their role might be underestimated in identifying the risk factors for virus shedding. Second, the patients received AVT empirically, which greatly varied in the selection of antiviral drugs and duration, thus making it extremely challenging to evaluate the role of antiviral drugs.Third, the estimated duration of viral shedding was limited by the frequency of respiratory specimen collection, lack of quantitative viral RNA detection, and a relatively low positive rate of SARS-CoV-2 RNA detection in throat swabs. Fourth, by excluding patients still in hospital as of March 8, 2020, and the low mortality in our group, the impact of virus shedding on mortality might be underestimated. Finally,the interpretation of our findings is limited by the sample size. Nevertheless, by including all adult patients in the designated hospitals in Shenzhen admitted for COVID-19, we believe that our study population is representative of the cases diagnosed and treated in a large city outside Wuhan.
CONCLUSlON
The present study is the first to examine the patterns of SARS-CoV-2 virus shedding and its risk factors. The results strongly suggest that SARS-CoV-2 was identified in a wide range of samples, including the respiratory tract, blood, and eye discharge. In addition, the data suggested that earlier hospitalization might help reduce the virusshedding period and ICU stay. Regarding clinical therapy, the analysis did not confirm the effectiveness of immunomodulation or AVT, but chloroquine could have the potential to shorten the duration and increase the possibility of shedding, although with limited power due to the small sample size. The findings of this retrospective study have important implications for the clinical treatment and policy making with regard to reducing the damage of the current pandemic caused by SARS-CoV-2.
ARTlCLE HlGHLlGHTS
Research background
The outbreak of coronavirus disease 2019 (COVID-19) cause emotional distress and anxiety worldwide. However, the factors for the severity of illness and its outcomes still remain unclear.
Research motivation
The goal of this study was to characterize the viral shedding patterns and risk factors in hospitalized patients with COVID-19.
Research objectives
The study aimed to identify the characteristics of viral load and shedding, the risk factors affecting the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)virus clearance and to evaluate the effect of prolonged viral shedding on the outcome of the patients.
Research methods
This was a retrospective study on all laboratory-confirmed COVID-19 patients with complete medical records admitted to the Shenzhen Third People’s Hospital from January 1, 2020 to March 8, 2020. A total of 7404 virological tests in 1350 patients were analyzed to identify the pattern of virus load in different samples. Furthermore, 145 patients with full inpatient records were statistically analyzed to reveal the risk factors associated with the viral shedding and ICU admission by multivariate cox regression.
Research results
SARS-CoV-2 virus was identified in a wide range of samples, including eye discharge.Earlier hospitalization might help reduce the virus-shedding period and intensive care unit (ICU) stay. Chloroquine is associated with the shortened shedding duration.
Research conclusions
Among various samples the SARS-CoV-2 virus, bronchoalveolar lavage fluid had the highest SARS-CoV-2 load. Elderly patients had higher virus loads, which was associated with a prolonged ICU stay. Chloroquine was associated with a shorter shedding duration and increased the chance of viral negativity.
Research perspectives
The findings about the virus shedding patterns and its risk factors suggested that early hospitalization has the potential to reduce the virus shedding time and the ICU stay.Also, the confirmation of effectiveness of immunomodulation and chloroquine might help in clinical treatment and policy making.
ACKNOWLEDGEMENTS
We sincerely thank Mr. Wang CY from Shanghai Jienuo Company, for providing the standard curve (plot of Ct value against the log of the standard sample amount).
 World Journal of Clinical Cases2020年24期
World Journal of Clinical Cases2020年24期
- World Journal of Clinical Cases的其它文章
- Primary duodenal tuberculosis misdiagnosed as tumor by imaging examination: A case report
- Successful endovascular treatment with long-term antibiotic therapy for infectious pseudoaneurysm due to Klebsiella pneumoniae: A case report
- Idiopathic adulthood ductopenia with elevated transaminase only: A case report
- Takotsubo cardiomyopathy associated with bronchoscopic operation: A case report
- Extracorporeal shock wave therapy treatment of painful hematoma in the calf: A case report
- Rare case of drain-site hernia after laparoscopic surgery and a novel strategy of prevention: A case report