
Clinical characteristics of pulmonary cryptococcosis coexisting with lung adenocarcinoma: Three case reports
2020-04-07 02:13GuiXianZhengHaiJuanTangZhiPingHuangHuiLingPanHanYiWeiJingBai
World Journal of Clinical Cases 2020年24期
Gui-Xian Zheng, Hai-Juan Tang, Zhi-Ping Huang, Hui-Ling Pan, Han-Yi Wei, Jing Bai
Gui-Xian Zheng, Hai-Juan Tang, Zhi-Ping Huang, Hui-Ling Pan, Han-Yi Wei, Jing Bai, Department of Respiratory Medicine, The First Affiliated Hospital of Guangxi Medical University, Nanning 530021, Guangxi Zhuang Autonomous Region, China
Abstract BACKGROUND Pulmonary cryptococcosis (PC) is an invasive fungal disease caused mainly by Cryptococcus (C.) neoformans or C. gattii. It may be present in immunocompetent or immunocompromised patients. The radiographic features of PC vary, and the most common computed tomography manifestation is the presence of solitary or multiple pulmonary nodules or masses distributed in the outer zone of the lung field. The appearance of nodular or mass-like PC on computed tomography scans resembles that of primary or metastatic lung cancers, and differential diagnosis is sometimes difficult. The coexistence of PC and malignant tumors is rarely observed.CASE SUMMARY This paper reports three cases of PC combined with lung adenocarcinoma diagnosed by video-assisted thoracic surgery lung biopsy, which were successfully managed by early diagnosis and treatment.CONCLUSION The present case report might serve as a reminder not to neglect PC coexisting with adenocarcinoma. Early diagnosis and treatment lead to a better prognosis.
Key Words: Adenocarcinoma; Coexistence; Computed tomography; Pulmonary cryptococcosis; Respiratory medicine; Case report
INTRODUCTION
Pulmonary cryptococcosis (PC) is a fungal infection that results from the inhalation of spores fromCryptococcus neoformans[1]. The infection usually occurs in immunocompromised patients, especially in those with T-lymphocytopenia[2]. The multiple nodular shadows that manifest, particularly in the peripheral lung, can sometimes be confused with malignant tumors and metastatic cancer based on nonspecific symptoms and radiological findings. Many case reports have focused on the misdiagnosis of PC as a malignant tumor[3]. This study aimed to describe three cases of multiple nodules with imaging findings, which were eventually diagnosed by thoracoscopy as PC coexisting with lung adenocarcinoma. After treatment, they all had a better prognosis. The coexistence of PC and malignant tumor was presented only in a few reports[4-9], and it is often easily misdiagnosed. Delayed treatment of malignant tumor results in a higher pathologic stage and poorer prognosis.
CASE PRESENTATION
Chief complaints
Case 1:A 69-year-old man presented with cough accompanied by chest discomfort for 2 mo, with no significant sputum and no fever, chest pain, wheezing, or weight loss.
Cases 2 and 3:A 54-year-old man (case 2) and a 46-year-old woman (case 3) had no chief complaints.
History of present illness
Case 1 presented to our hospital in August 2017 for cough accompanied by chest discomfort for 2 mo. He denied other discomfort. Cases 2 and 3 had no clinical symptoms. They were admitted to our hospital for abnormal findings on annual screening chest radiography.
History of past illness
Case 1 had a history of smoking. Case 3 had a history of systemic lupus erythematosus and chronic viral hepatitis B, and was administered oral telbivudine, hydroxychloroquine, and methylprednisolone sodium succinate regularly. These three patients denied having a history of exposure to pigeon droppings or pets.
Personal and family history
All the three cases had not traveled recently and their family history was unremarkable.
Physical examination
There were no physical findings to note.
Laboratory examinations
Case 1:Laboratory data, including the results of routine blood tests, C-reactive protein levels, and erythrocyte sedimentation rates, were all normal. Blood fungal examinations (Candida antigen, Aspergillus DNA,Cryptococcus neoformansantigen,and beta-D-glucan) were all negative. An enzyme-linked immunosorbent assay test for human immunodeficiency virus (HIV) was negative. Total lymphocyte, CD4, and CD8 counts and serum complement and immunoglobulin levels were normal. Triple sputum smears for the acid-fast bacilli test and fungus were negative. Tumor markers in blood, including carcinoembryonic antigen (CEA), cancer antigen 125 (CA125),CA199, neuron-specific enolase, squamous cell carcinoma, and cytokeratin 19, were all normal.
Case 2:Laboratory data, including routine blood tests and blood tumor markers (CEA and CA125), were all normal.
Case 3:Laboratory data were normal for routine blood tests, the tumor marker CEA was normal, and the CA125 level increased by 50.91 U/mL (normal value 0-35 U/mL).
Imaging examinations
Case 1:Computed tomography (CT) of his chest showed multiple nodules in both lungs (Figure 1A and B).
Case 2:Chest CT revealed a ground-glass nodule in the posterior segment of the right upper lobe apex (Figure 1C and D) and multiple nodules in the left upper lobe with a maximum diameter of 7 mm. Neither hilar nor mediastinal lymphadenopathy was noted. The lesions did not change after 1 year of follow-up.
Case 3:A CT scan of her chest showed two nodules in the right lower lobe, one in the dorsal segment and the other in the outer basal segment (Figure 1E and F).
FINAL DIAGNOSIS
Case 1
Preoperative diagnosis was lung cancer with intrapulmonary metastasis. Finally, the patient underwent surgery. Partial resection of the left upper lobe was performed using video-assisted thoracoscopy. The histologic examination after resection revealed primary lung adenocarcinoma (Figure 2A). Additionally, partial resection of the right lower lobe using video-assisted thoracoscopy showed PC (Figure 2B), with positive periodic acid-Schiff (PAS) (Figure 2C) staining and PAS diastase (D-PAS) (Figure 2D)staining.
Case 2
Cryptococcosis was diagnosed by histologic examination of the left upper lobe.Histologic finding of the right upper lobectomy reveled alveolar cell carcinoma.
Case 3
Alveolar cell carcinoma in the dorsal segment of the lower lobe of her right lung and cryptococcosis in the outer basal segment of the lower lobe of her right lung were diagnosed by lung biopsy under video-assisted thoracoscopy.
TREATMENT
Case 1
Partial resection of the left upper lobe and the right lower lobe was performed using video-assisted thoracoscopy. The patient received fluconazole (200 mg daily) for 6 mo after the surgery.
Case 2
Cryptococcosis was diagnosed by wedge resection under video-assisted thoracoscopy of the left upper lobe. But 1-mo fluconazole (200 mg/d) as an antifungal therapy did not reduce the size of masses. We performed a right upper lobectomy. The patient received 6 mo of treatment with fluconazole (200 mg daily) postoperatively.
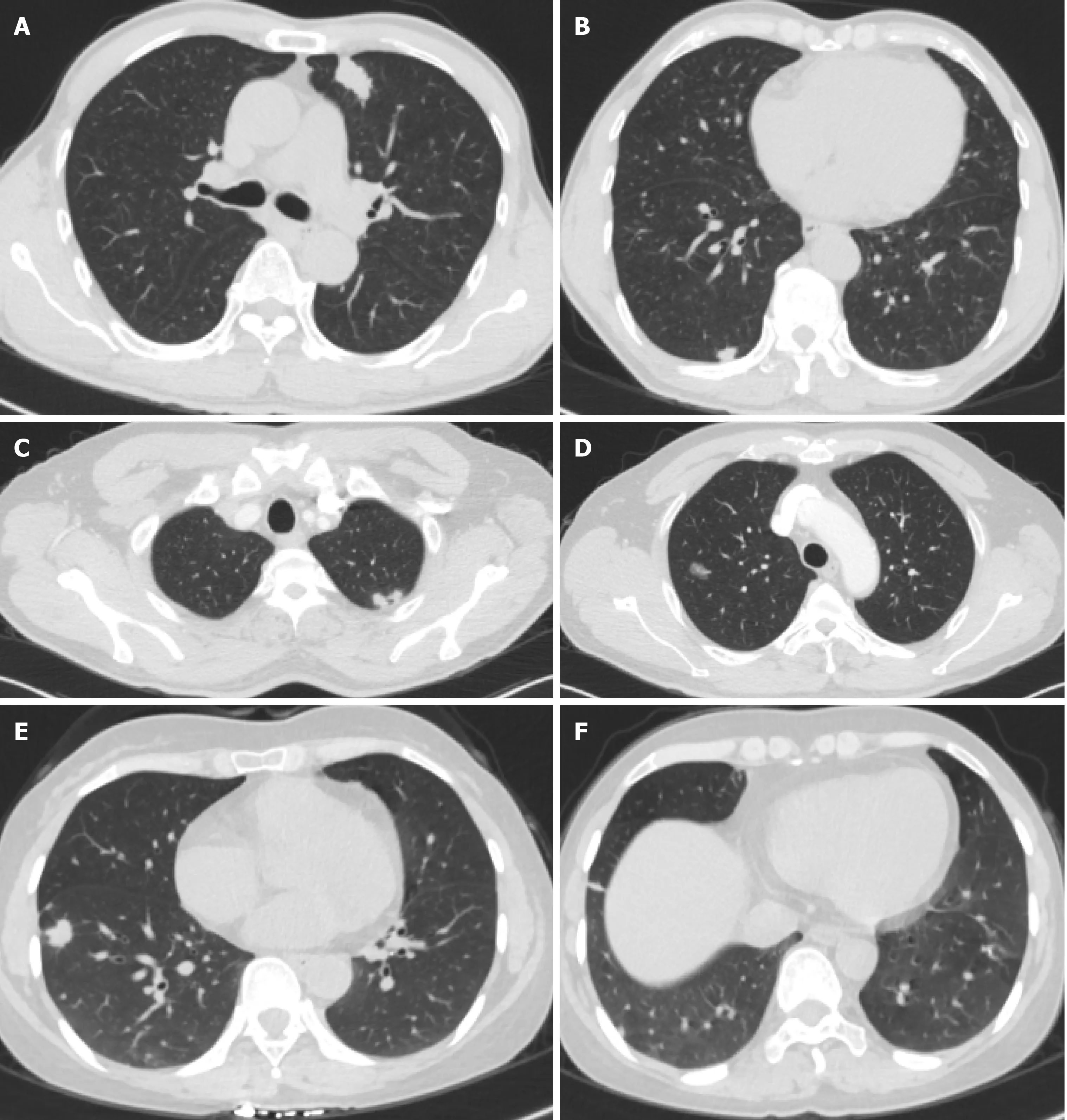
Figure 1 Computed tomography images. A and B: Case 1 with multiple nodules in both lungs. C and D: Case 2 with a ground-glass nodule in the posterior segment of the right upper lobe apex. E and F: Case 3 with two nodules in the right lower lobe, one in the dorsal segment and the other in the outer basal segment.
Case 3
The patient took fluconazole (200 mg daily) as an antifungal therapy for 6 mo.
OUTCOME AND FOLLOW-UP
There was no evidence of recurrence at 2 years postoperatively and after fluconazole treatment in these three cases.
DISCUSSION
PC coexisting with pulmonary carcinoma is rare, with only one case each reported in Japan, China, South Korea, and other countries in East Asia[4-9]. The aforementioned three cases had multiple lung nodules, and the patients were ultimately diagnosed with PC coexisting with adenocarcinoma by lung tissue biopsy. The cases highlighted the possibility of duality in the diagnosis of multiple pulmonary nodules based on the CT examination. They point to the possibility of the coexistence of PC and adenocarcinoma and indicate that the pathological results of one lesion cannot represent the characteristics of all lesions. In such cases, close follow-up and biopsy of multiple lesions may be required.
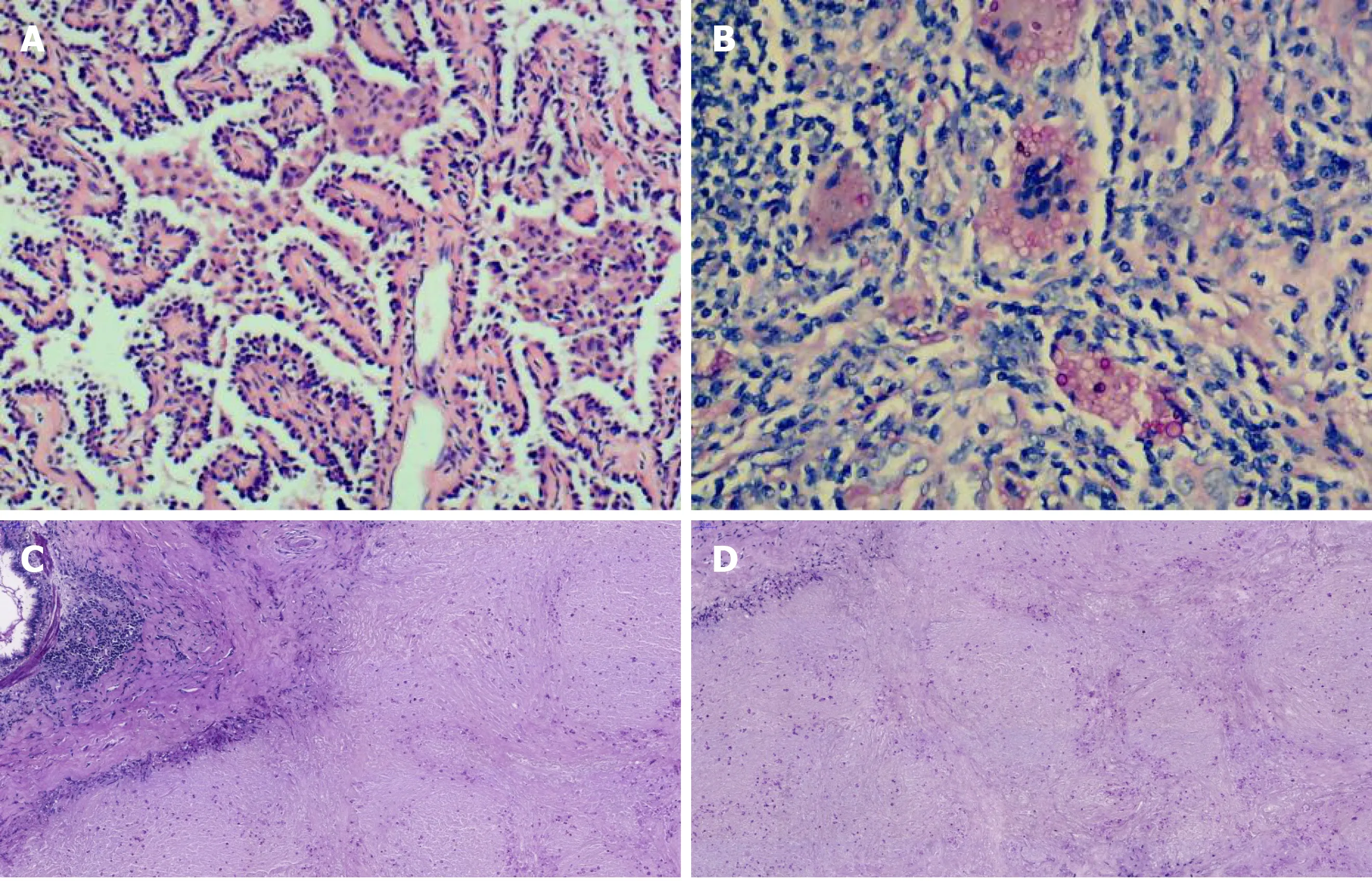
Figure 2 Histologic examination images. A: Histopathological examination of case 1 showed that the adenocarcinoma was arranged along the alveolar septum in a papillary pattern [hematoxylin-eosin (HE) staining, original magnification × 100]; B: The yeast form of Cryptococcus neoformans was observed throughout the granulation tissue, with macrophage phagocytosis (HE staining, original magnification × 200); C: Periodic acid-Schiff (PAS) staining; D: PAS diastase staining.
The clinical symptoms of the aforementioned cases were nonspecific, including mainly cough and sputum; cases might also be asymptomatic. The results of routine blood tests and tumor marker CEA for these cases were normal. Serum cryptococcal antigen detection tests by latex agglutination were performed in one case, with negative results. The PC nodules in these cases were located in the field of the lung,adjacent to or involving the pleura; single or multiple nodules with a diameter of less than 1 cm were predominant. The CT findings of lung cancer consisted of a solitary nodule shadow accompanied by a variety of CT tumor-like signs, such as lobulation signs, burr signs, pleura depression signs, and focal ground-glass opacity. In one case(case 3), lung cancer and cryptococcus nodules were located in the same lung lobe. In the remaining two cases, the lung cryptococcosis nodules and lung cancer nodules were not on the same side of the lung lobe. Nodular or mass-type PC is easily misdiagnosed as lung cancer or metastatic cancer. Notably, the differences in imaging findings between the two diseases may help in identification: PC nodules predominantly occur adjacently to the pleura, have different shapes and sizes, and are limited to a single lung lobe; pulmonary metastatic tumors that usually present with variable in sizes and shapes with smooth edges frequently occur in the lower lungs. In most reported cases, the pathological type of lung cancer was pulmonary adenocarcinoma, which was similar to that in patients in this study. Cryptococcus may prefer residing in the peripheral lung, and therefore it is difficult to obtain a definitive diagnosis for multiple pulmonary nodules in the peripheral lung on chest CT.Attention should be paid to the characteristics of the nodule, and thoracoscopic surgery should be performed in time so that patients can be diagnosed and treated as early as possible. A definite diagnosis for the patients in this study took less time. The nodules with different etiology have characteristic imaging manifestations, and pathology is the key to diagnosis.
Cryptococcal infections affect a variety of hosts, including those who have severely compromised immune systems and those who have “normal” immune systems.However, they are occasionally found in immunocompetent hosts and are more likely to occur in immunosuppressed patients, such as those undergoing organ transplant or long-term glucocorticoid therapy and those with hematological malignancies, diabetes,and liver cirrhosis, among others. In China, PC is the third most common pulmonary fungal infection; most patients with PC in China have no underlying disease[10]. The patients in the present study denied any history of contact with birds or polluted environment and had not traveled recently. When and where these patients became infected with spores was not known. Haradaet al[4]suggested that the coexistence of the two lesions was coincidental. However, Robinsonet al[7]proposed that lung cancer caused immunosuppression and secondary cryptococcal infection. The relationship between lung cancer and PC should be further explored.
CONCLUSION
The present study provided many interesting insights into the differential diagnosis of multiple pulmonary nodules. Resection of the lesion should be performed under medically permissive conditions to obtain a definitive diagnosis for pulmonary nodules suspected as malignancy.
 World Journal of Clinical Cases2020年24期
World Journal of Clinical Cases2020年24期
- World Journal of Clinical Cases的其它文章
- Role of gut microbiome in regulating the effectiveness of metformin in reducing colorectal cancer in type 2 diabetes
- lmpact factors of lymph node retrieval on survival in locally advanced rectal cancer with neoadjuvant therapy
- Three-year follow-up of Coats disease treated with conbercept and 532-nm laser photocoagulation
- Virus load and virus shedding of SARS-CoV-2 and their impact on patient outcomes
- Risk factors for de novo hepatitis B during solid cancer treatment
- Cause analysis and reoperation effect of failure and recurrence after epiblepharon correction in children