
Network pharmacology-based approach to investigate the mechanisms of Yiyi Fuzi Baijiang Powder in the treatment of malignant tumors
2018-11-13 02:06ShangJinSongRenJieXuLiJuanXiuXuanLiuXiaoQiangYue
Traditional Medicine Research 2018年6期
Shang-Jin Song , Ren-Jie Xu , Li-Juan Xiu , Xuan Liu *, Xiao-Qiang Yue *
1 Changzheng Hospital, Naval Military Medical University, Shanghai, China.
Backgrou nd
Network pharmacology was first proposed by Professor Andrew Hopkins [1]. It is a relatively new bioinformatics research method based on the theory of system biology,using high-throughput data analysis, virtual computing,and network database retrieval, building biological information networks, and analyzing network topology to explore the complex nonlinear network relationship between target and disease [2]. This method abandons the traditional thinking of "one disease, one target, one drug"and constructs a multi-level "drug-target-disease"network structure based on the concept of "multi-drugs and multi-targets" to achieve the goal of predicting drug targets as a whole [3]. This approach coincides with the overall concept of traditional Chinese medicine (TCM)and syndrome differentiation, and provides a new avenue for the study of Chinese medicinal compounds [4, 5].
The use of Yiyi Fuzi Baijiang powder (YFBP) was first recorded in Shanghan lun, compiled by the Chinese physician, Zhang Zhongjing, which was published in the Eastern Han Dynasty of China (3 century A.D.). It is mainly composed of Yi Yi Ren (Semen Coicis,YYR), Fu Zi (Rhizoma Typhonii, FZ), and Bai Jiang Cao (Herba Patriniae, BJC). Of these, YYR eliminates phlegm and relieves pain; FZ activates meridians to reduce pain, and BJC promotes blood circulation and has detoxifying effects. This prescription was used to treat Changyong by Zhang Zhongjing. In TCM theory, Changyong is a disease characterized by inflammation and pain, similar to the clinical manifestations of chronic appendicitis,appendiceal abscess, abdominal abscess, Crohn's disease,and ulcerative colitis in Western medicine [6-8]. However,its mechanism of action has not yet been elucidated.Therefore, this study aims to explore the main components, targets, and signaling pathways using network pharmacology to provide a basis for further experiments.
Materials and methods
Screening of major chemical components of YFBP
The chemical constituents of YYR, FZ, and BJC were collected from TCM Systems Pharmacology Database(TCMSP) (http://ibts.hkbu.edu.hk/LSP/tcmsp.php) [9],TCM Integrated Database (TCMID) (http://www.megabionet.org/tcmid) [10], and TCM Database@Taiwan [11].
Screening of effective chemical components
Traditional Chinese medicine formulae exert pharmacological effects on metabolic processes such as absorption, distribution, metabolism, and excretion,usually via oral administration. Oral bioavailability (OB)refers to the relative amount and rate of drug absorbed into systemic blood circulation after oral administration and is one of the most important parameters in pharmacokinetics. Compounds with OB ≥ 30% are considered to be effectively absorbed by the human body[12]. The drug-like index (DL), established to analyze the structural features or/and physiochemical properties of drug candidates by comparing them to existing drugs from the DrugBank (https://www.drugbank.ca/) database[13], has been widely used to filter out compounds. A DL< 0.18 indicates that the test compound is not suitable as a medicine [14]. These two parameters are important for screening the effective compounds [15]. In this study,compounds with OB ≥ 30%, and DL ≥ 0.18 were selected as active compounds for further investigation [9].
Target and disease prediction
The targets of effective active compounds were collected from DrugBank, TCMSP, and TCMID. Compounds without a corresponding target or duplicate targets were eliminated. The relevant diseases for the corresponding targets from TCMSP were predicted and classified according to the International Classification of Diseases Code.
Network construction and analysis
To achieve a systematic understanding of the complex relationships among compounds, targets, and diseases,compound-target-diseases networks were constructed and analyzed in Cytoscape 3.5.1 (https://cytoscape.org/) [16].In the output results, nodes with different colors represent active ingredients, targets, and diseases. The potential target and the effector compound (s) are connected by edges; similarly, if a target protein regulates a disease, the two are also connected by edges. In this way, effective components, targets, and related diseases are linked. Two important network topology parameters [17], Degree and Betweenness Centrality were analyzed using the Network Analyzer plug-in in the Cytoscape software to evaluate the core chemical components, core targets, and core diseases associated with YFBP.
Biological functions and pathway analysis of targets
We transformed the selected targets to corresponding gene names by UniProt (http://www.uniprot.org/) [15]database. Gene ontology (GO) biological process enrichment analysis and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis of target genes were analyzed using the Database for Annotation, Visualization and Integrated Discovery(DAVID). P < 0.05, corrected by Bonferroni method,indicated statistical significance.
The selected target was searched in the UniProt [18]database to identify the corresponding gene name and number. To find the most significant enrichment of biological annotations, the target genes were analyzed via gene ontology and KEGG pathway analysis using the bioinformatics annotation database DAVID(https://david.ncifcrf.gov/) [19]. Items with P < 0.01 after correction with Bonferroni method were considered to be significantly enriched [20, 21].
Results
Compounds of YFBP
As of April 2018, a total of 294 compounds were identified from YFBP, including 81 compounds from YYR, 130 compounds from FZ, and 93 compounds from BJC through TCMSP, TCM Database@ Taiwan TCMID,and literature search, after removing the duplications.Among them, 43 compounds with OB ≥ 30% and DL ≥0.18 were selected as effective active compounds. After removing 19 compounds without a target, a total of 24 effective chemical compounds including 6 compounds from YY, 8 compounds from FZ, and 13 compounds from BJC were selected for further investigation. Of these,stigmasterol is common to YY and BJC, and β-sitosterol was common to all the three drugs (Table 1).
Compounds-targets netw ork construction and analysis
The 24 selected effective chemical components were searched in DrugBank, TCMSP, and TCMID databases,and 133 corresponding targets were obtained after ruling out repetitive targets. The obtained target proteins and chemical constituents were imported into the Cytoscape software to construct the component-target network diagram of YFBP (Figure 1). There are 249 sides in this network, presenting the interactions between components and targets. A total of 157 nodes including 24 compounds and 133 targets were obtained after deletion of duplicates(Figure 2). The average degree of 24 compounds was 19.79. Of these, 8 compounds showed a degree > 19.79.The average degree of 133 targets was 3.57, and 42 targets had degrees > 3.57. Estrogen receptor, androgen receptor, and prostaglandin G/H synthetase 2 were regulated by 18, 18, and 15 compounds, respectively, in YFBP.
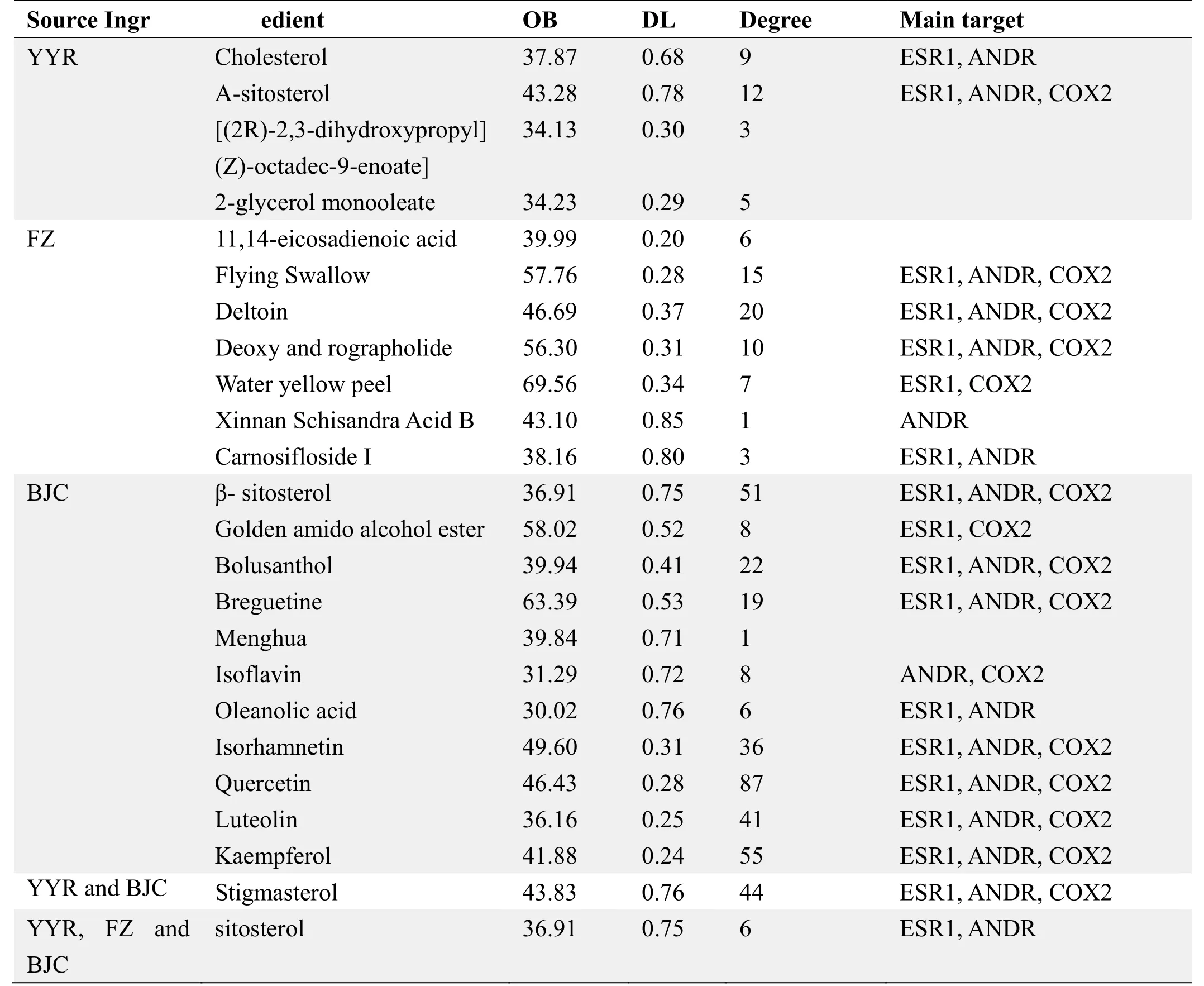
Table 1 Effective chemical components and main targets of Yiyi Fuzi Baijiang Powder
Compounds-targets-diseases network construction and analysis
A total of 305 corresponding diseases for 133 key targets were obtained after deletion of duplicates. There were 1017 edges in the network, representing the corresponding relationship between the compounds,targets, and diseases associated with YFBP. There were 462 nodes, including 133 drug targets and 305 diseases(Figure 2). The average degree of 133 targets was 7.65.The degree of 51 targets was observed to be greater than the average degree. The average degree of 305 diseases was calculated to be 1.78. The degree for 87 diseases was greater than the average degree. Using the two-network topological parameters of node degree and intermediate center degree, the diseases related to YFBP were predicted.
According to the International Classification of Diseases Code ICD-10, 305 diseases related to YFBP were classified. Seventy-eight different types of tumors(25.57%) accounted for the largest proportion of the diseases. The top 20 diseases included 7 different types of tumors and 4 diseases related to inflammation and pain,which are the main clinical manifestations of intestinal carbuncles. Among these, Crohn's disease, ulcerative colitis, and inflammatory bowel disease are considered to belong to the category of intestinal carbuncles in TCM(Table 2). We noted that the most potential diseases associated with YFBP were tumors and intestinal carbuncles. The results not only preliminarily corroborate the original decision of Zhang Zhongjing to treat intestinal carbuncles using YFBP, but also provide a scientific basis for historical prescriptions used in the treatment of malignant tumors.
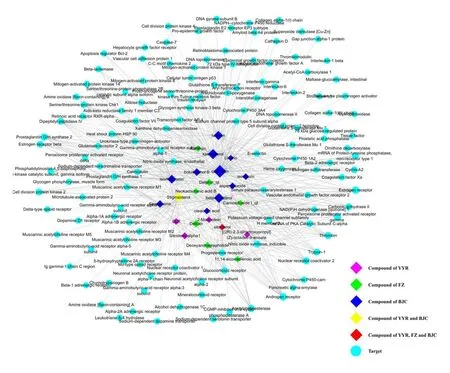
Figure 1 Active compounds-targets network diagram
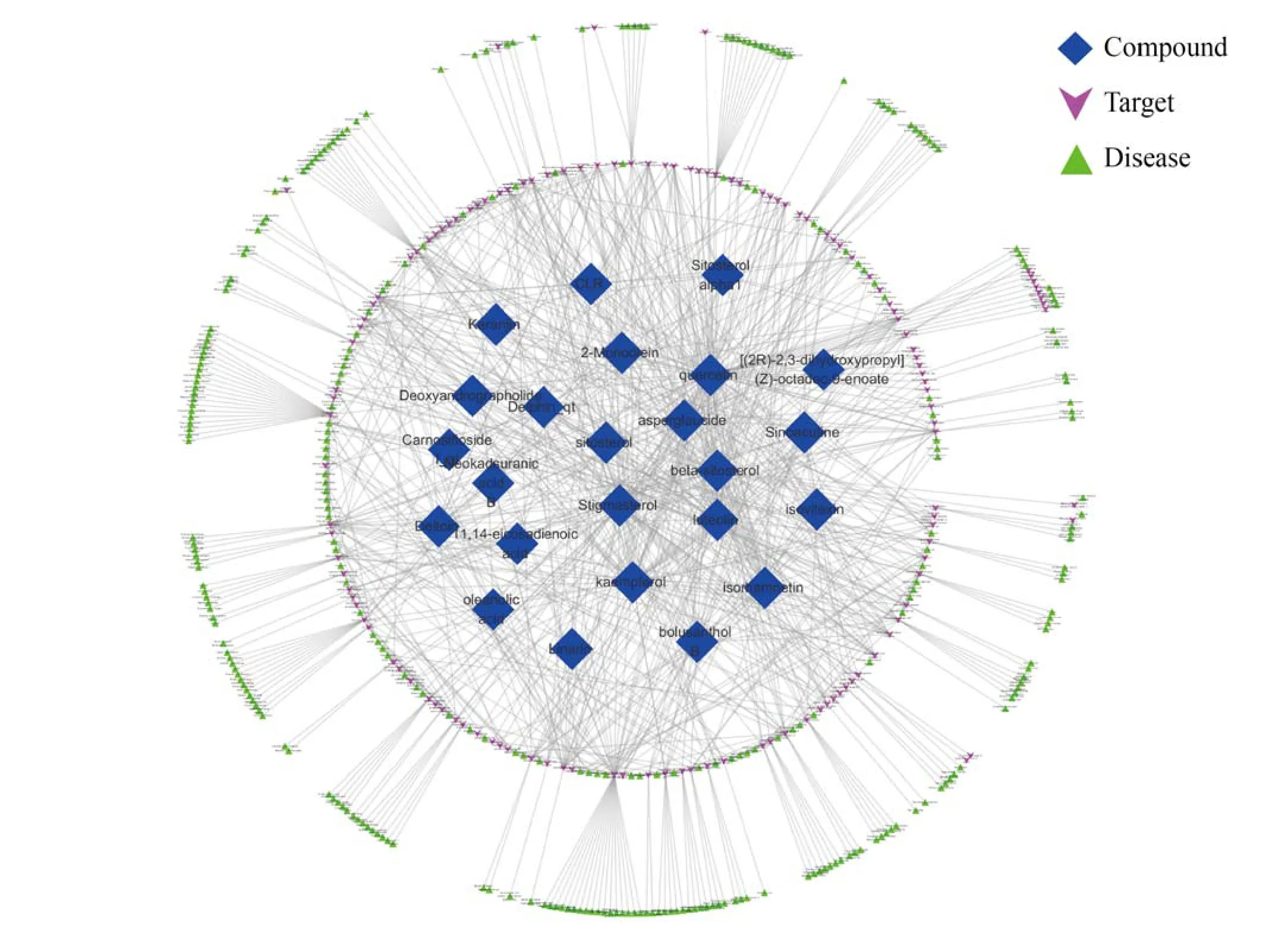
Figure 2 Compounds-targets-diseases network
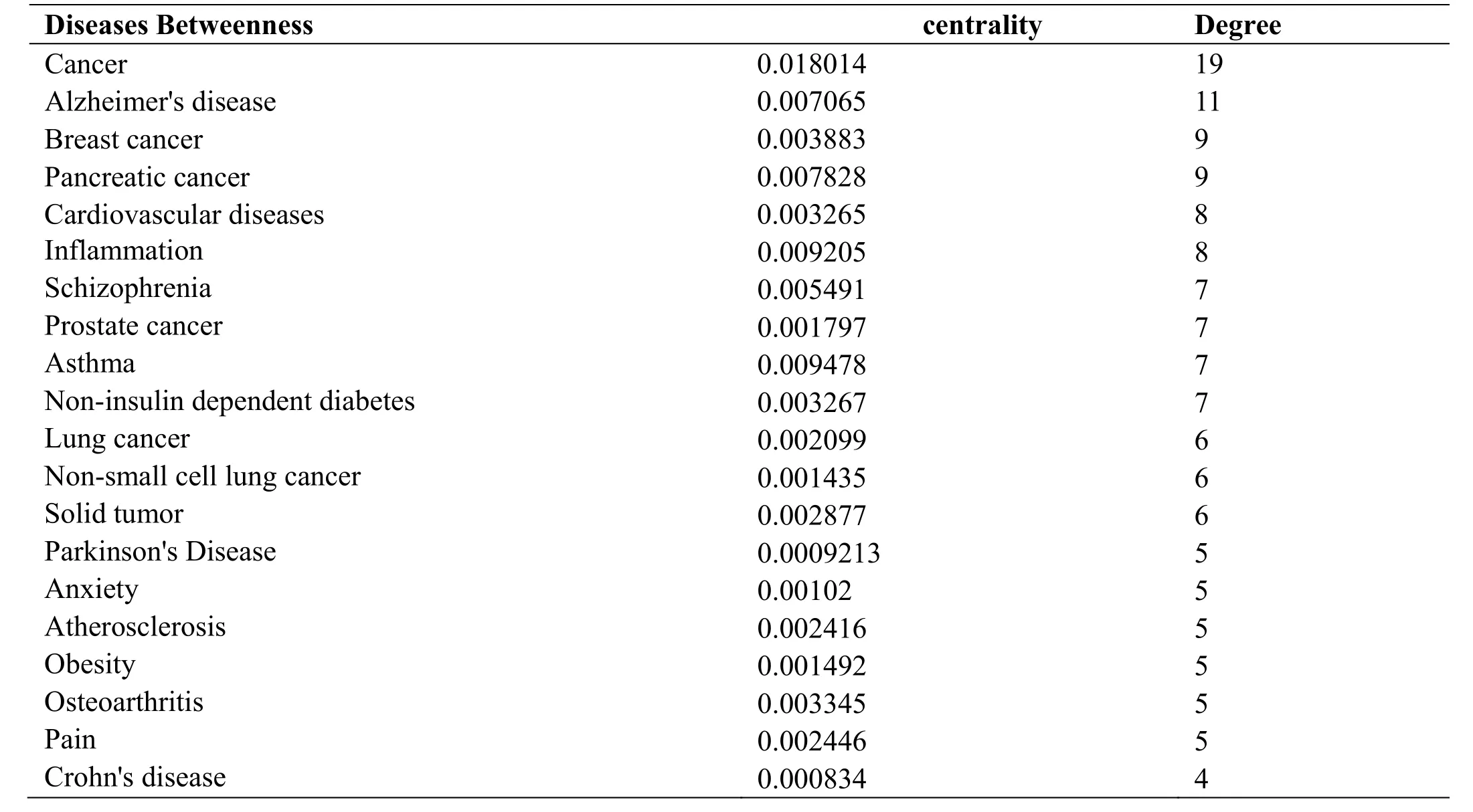
Table 2 The top 20 diseases related to YFBP
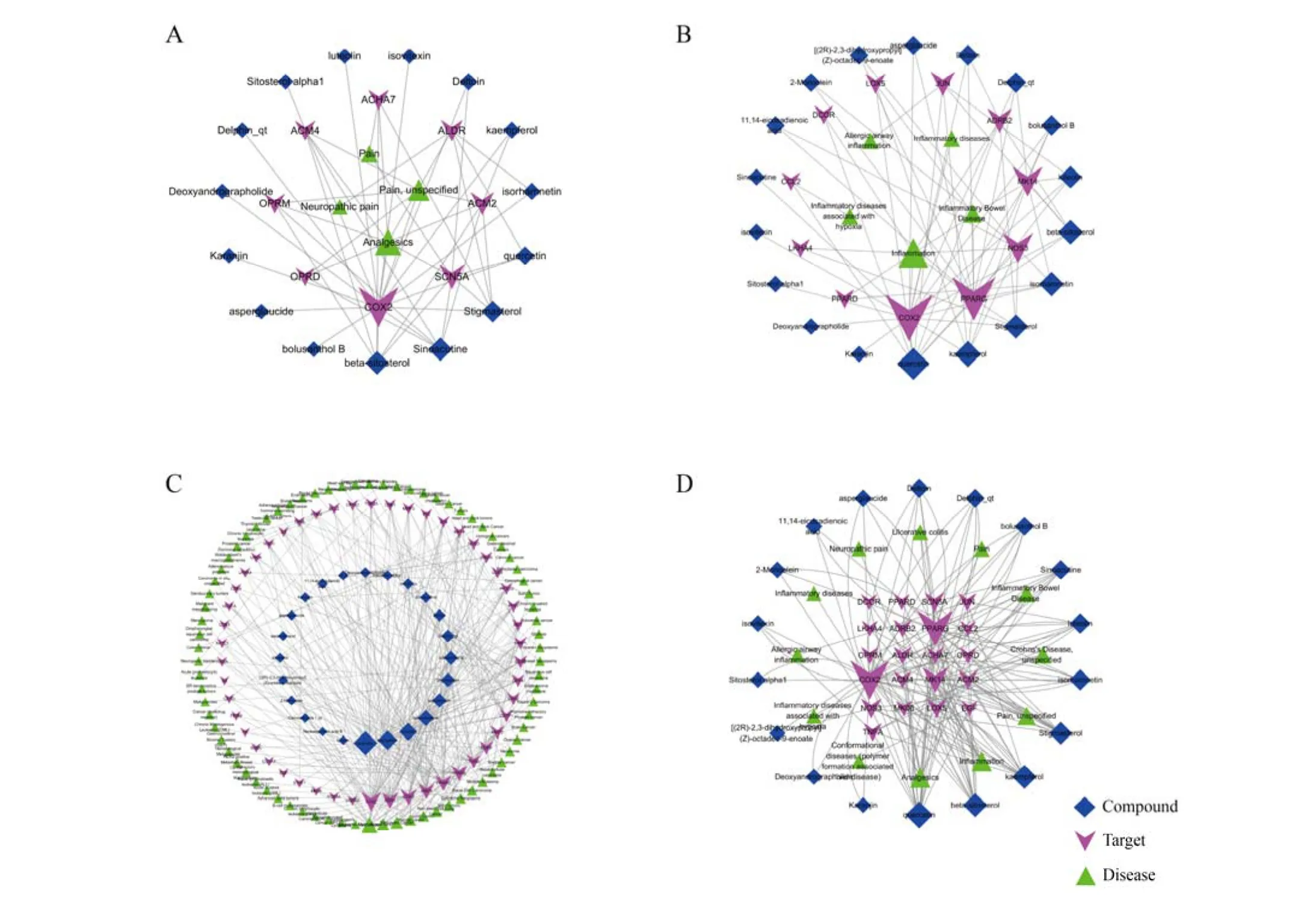
Figure 3 Compounds-targets-core diseases network
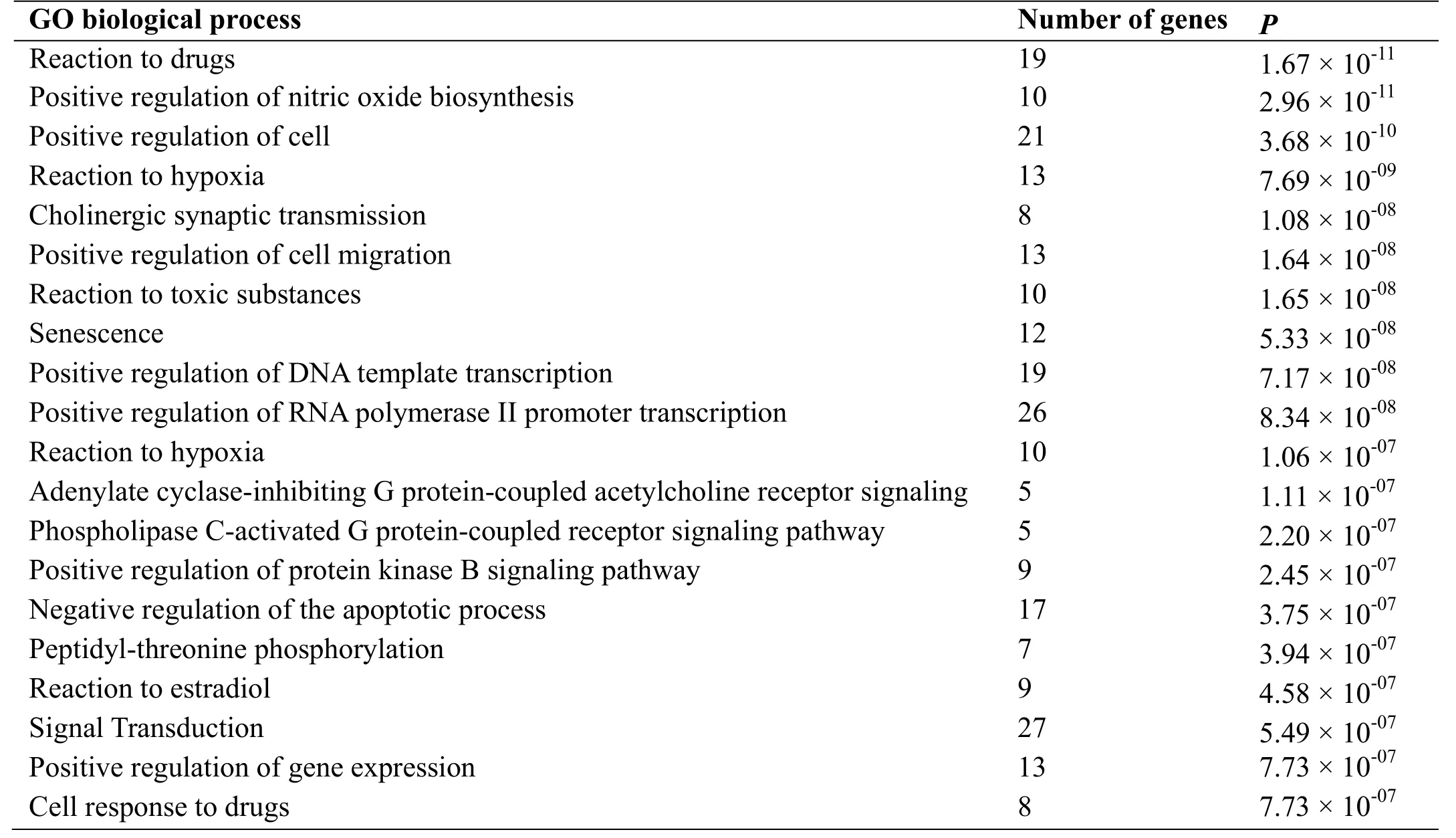
Table 3 Significantly enriched GO biological process
Annotation analysis of the target pathways of YFBP
Using the online biological information annotation database DAVID, the biological function and signal pathways affected by YFBP were revealed, and,following enrichment analysis, 419 KEGG pathways that could play the role of "different disease with the same treatment" were obtained, including responses to drugs,hypoxia, and toxic substances and 30 biological processes with significant roles in cell proliferation and cell migration (Table 3). There were 115 KEGG pathways for YFBP, including neuroactive ligand-receptor interactions,calcium-signaling pathways, cancer pathways, TNF signaling pathways, PI3K-Akt signaling pathways,estrogen-signaling pathway, the HIF-1 signaling pathway,and the cGMP-PKG signaling pathway (Table 4).
Analysis of mechanism of YFBP in treatment of tumor and intestinal palsy
The compounds and targets related to tumor, pain, and inflammation were introduced into the Cytoscape software to construct a network and conduct analysis of their network topology. Analysis of the pain-related compound-target-disease network (Figure 3) revealed that COX-2 is the main target for the treatment of pain using YFBP, followed by SCN5A (sodium voltage-gated channel alpha subunit 5) and ACM2 (Muscarinic acetylcholine receptor M2); β-sitosterol and serotonin are the main target compounds for the treatment of pain using YFBP, which can be combined with 6 pain-related targets.Through annotation analysis of pain-related targets, it was found that YFBP mainly relies on ligand-receptor interactions affecting neural activity, cholinergic synaptic transmission, and G-protein coupled receptor signaling pathways for pain relief.
The analysis of the inflammation-related compoundtarget-disease network (Figure 3) suggested that COX-2 is also the main target for the treatment of inflammation by YFBP, followed by PPARG (Peroxisome Proliferator Activated Receptor Gamma), NOS3 (Nitric oxide synthase 3), and MAPK14 (Mitogen-activated protein kinase 14). Meletin is the most important compound for the treatment of inflammation, which can bind to 9 inflammation-related targets, followed by campherol,which can bind to 6 targets. Through annotated analysis of pathways related to inflammation-related targets, it was found that YFBP exerted its therapeutic effect in inflammation-related diseases by affecting TNF- and VEGF-signaling pathways. Pain and inflammation are the main clinical manifestations of intestinal fistulae; YFBP may treat intestinal fistulae by a mechanism related to the treatment of pain and inflammation, which is consistent with the results of the compound-target-disease network analysis (Table 2).
We analyzed the tumor-associated compound-target-disease network (Figure 3) and found that COX-2 is the main target for the treatment of tumors with YFBP, followed by ESR1 and CDK2(Cyclin-dependent kinase 2); Quercetin is the main compound for the treatment of pain, which is capable of binding to 40 tumor-associated targets, followed by kaempferol (28 targets), and luteolin (14 targets).Through annotation analysis of tumor-associated targets,it was found that YFBP exerts its anti-tumor effect mainly through the PI3K-Akt, estrogen, and TNF signaling pathways.
Discussion and prospects
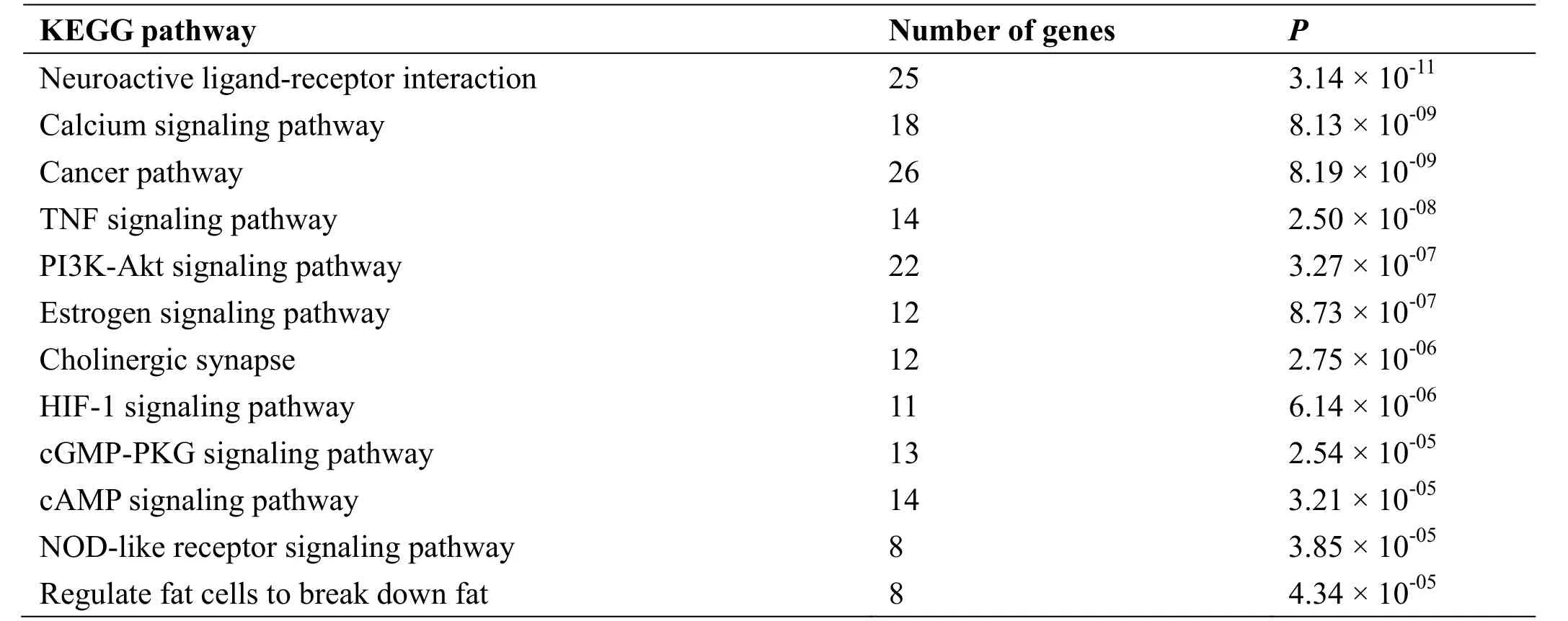
Table 4 Significantly enriched KEGG pathway
The curative effects of TCM have always been praised,but it is widely criticized for its unclear mechanisms of action. Modern research theory holds that traditional Chinese medicinal compounds work through multiple targets and pathways, but it is difficult to verify their effective components individually through experiments,owing to issues arising from compatibility and complex components. The development of network pharmacology provides a good research platform for this problem.Database searches for TCM planes can reveal the components of each drug in the compound prescription.Based on the OB and DL values, we can screen out the active components that can be absorbed and utilized by the human body. These targets predict potential diseases that may be treated, and the DAVID online data platform can be used to analyze possible mechanisms for the same.This approach can provide logical directions for later experimental verification.
Chinese physician Zhang Zhongjing in the Jingui Linglan mainly used YFBP for the treatment of intestinal carbuncles, mainly characterized by inflammation and pain. In modern medicine, intestinal carbuncles encompass appendicitis abscesses, abdominal abscesses,Crohn's disease, ulcerative colitis, and so on. By constructing a component-target-disease network (Figure 3) associated with intestinal carbuncle (including inflammation, pain, Crohn's disease, ulcerative colitis,and inflammatory bowel disease), we found that 18 active ingredients, including β-sitosterol, quercetin, and kaempferol, could bind to COX-2, PPARG, MK14 and other targets by acting on TNF (tumor necrosis factor),NOD-like receptor, Toll-like receptor, MAPK(mitogen-activated protein kinase), and receptors for other signaling pathways. COX-2 is the most important target for YFBP in the treatment of intestinal carbuncles.Studies have shown that TNF [22], NOD-like receptor[23], Toll-like receptor [24], and MAPK [25, 26]signaling pathways play an important role in the occurrence and development of inflammatory bowel diseases, such as Crohn's disease, ulcerative colitis, and other inflammatory bowel diseases. Mizoyama [27] and Habtemariam [28] et al. have confirmed through experiments that kaempferol, luteolin, and quercetin from YFBP can play a role in relieving symptoms and treating inflammatory bowel disease. The results preliminarily corroborate Zhang Zhongjing's original decision to treat intestinal carbuncles using YFBP.
In addition, YFBP has been widely used in the treatment of painful diseases, such as angina pectoris [29],prostatic pain [30], dysmenorrhea and chronic pelvic pain[31, 32]; and inflammatory diseases [33] like prostatitis,pelvic inflammatory disease [34, 35], cervicitis, chronic rhinosinusitis [36], adnexitis, endometritis [36-38], anal sinusitis, and cholecystitis [39]. In addition, various compounds from YFBP have been shown to alleviate pain and inflammation, such as guilt-glutenol [40], legumes[41] and quercetin [42], which all have analgesic effects.Granado et al. [43] have shown that quercetin can reduce the inflammatory response in liver cells via TNF signaling. Lee et al. [44] confirmed that quercetin could alleviate inflammation in mouse retinal photoreceptor cells. Chen et al. [45] confirmed that kaempferol could alleviate LPS-induced acute lung injury in mice through the TNF signaling pathway.
Zhang Zhongjing pointed out that when YFBP was used in the treatment of intestinal carbuncle, it should be distinguished from abdominal tumors. However, in recent years, an increasing number of studies have found that chronic inflammation plays an extremely important role in the occurrence and development of tumors. Moderate inflammation can activate the immune system and promote the clearance of the foreign antigens. However,persistent and recurrent chronic inflammation can lead to repeated injury to tissues and organs, resulting in DNA damage, and genomic instability leads to malignant transformation in tissues [46, 47]. Therefore, we speculated that YFBP could play a role in treating tumors by treating chronic inflammation. This result was also confirmed by the analysis of the tumor-related component-target-disease network. COX-2 is the main target of YFBP in the treatment of tumors, followed by ESR1 and CDK2. Quercetin was the most potent antitumor component of YFBP. Quercetin not only has strong antitumor properties [48], but also can reverse the polytropic in-resistance of prostate cancer by PI3K-Akt signaling pathway [49], and when combined with metformin, it inhibits the proliferation of prostate cells via the PI3K-Akt signaling pathway [50]. Sildenol [51]and luteolin [52] in YFBP also have been shown to exhibit antitumor effects. Kanglaite, developed from YFBP, has been widely used in the treatment of tumors[53, 54]. Du Yanlin et al. [55] found that YFBP combined with chemotherapy could significantly alleviate the toxic effects of chemotherapy and improve patients' quality of life.
We found that COX-2 was the most important target for YFBP, both in intestinal carbuncles and malignant tumors. COX is the key enzyme that catalyzes arachidonic acid to prostaglandins. It has two isozymes,COX-1 and COX-2. The expression of COX-2 is not high under homeostatic conditions, but it is synthesized rapidly when the cells are stimulated and participates in many pathophysiological processes [56]. Non-steroidal anti-inflammatory drugs mainly exert their anti-inflammatory and analgesic effects by inhibiting COX-2. Nimesulide and celecoxib, commonly used in clinical practice, also exert their analgesic effects by selectively inhibiting COX-2 activity. Growing evidence suggests that COX-2 continues to be highly expressed in different tumor tissues [57], and plays an important role in tumor apoptosis, angiogenesis, invasion, and metastasis [58]. As early as 2006, Bertagnolli et al. [59]and Pruthi et al. [60] found that celecoxib could reduce the incidence of colon adenomas (precancerous lesions of the large intestine) and alleviate the progression of prostate cancer. In breast cancer mouse models [61],celecoxib combined with an EP4 antagonist(ONO-AE3-208) was also shown to slow tumor growth and inhibit angiogenesis, lymph angiogenesis, and lung and lymph node metastasis.
Conclusion
In this study, we used the method of network pharmacology to screen out the active ingredients and related targets of YFBP, and found that intestinal carbuncle and tumors were the main diseases which could be treated by YFBP, and elaborated its potential mechanism of action. The preliminary confirmation of the conventional use of using YFBP in the treatment of intestinal carbuncle provides additional scientific evidence for the use of this prescription in the treatment of malignant tumors. However, the limitation of the study is that it does not factor in the compatibility of the three Chinese medicines and the chemical reaction between different components during the decoction process, which may affect the active components. Therefore,experimental verification is needed to further elucidate the specific mechanism of action of this prescription.
1. Hopkins AL. Network pharmacology. Nat Biotechnol 2007, 25: 1110-1111.
2. Hopkins AL. Network pharmacology: the next paradigm in drug discovery. Nat Chem Biol 2008, 4:682-690.
3. Drews J. Drug discovery: a historical perspective.Science 2000, 287: 1960-1964.
4. Wang Y, Li C, Li D, et al. Chinese medicine pharmacological research strategies based on biological networks and integration of disease and syndrome. Chin J Integr Tradit Western Med 2012,32: 552-555.
5. Liu QS, Zhang ZQ, Fang L, et al. Application of high-throughput technology and network pharmacology in screening active components of traditional chinese medicine. China J Tradit Mater Med 2012, 37:134-137.
6. Zhang JL, Chen GQ. Theory and practice of Golden Chamber.Beijng:People's Health Publishing House,2009: 228-229.
7. Cheng SF, Cheng SL, Ma JL, et al. A case study on the treatment of Crohn's disease with Yiyi Fuzi Baijiang powder. Chin J Tradit Chin Med Inform 2011,18: 87.
8. Zu GY, Chang YJ, Dong XL, et al. Clinical observation on treatment of ulcerative colitis with traditional Chinese medicine retention enema combined with heat sensitive moxibustion. Sichuan Tradit Med, 2017, 35: 77-79.
9. Ru J, Li P, Wang J, et al. TCMSP: a database of systems pharmacology for drug discovery from herbal medicines. J Cheminform 2014, 6:13.
10. Xue R, Fang Z, Zhang M, et al. TCMID: Traditional Chinese Medicine integrative database for herb molecular mechanism analysis. Nucleic Acids Res 2013, 41: 1089-1095.
11. Chen CY. TCM Database@Taiwan: the world's largest traditional Chinese medicine database for drug screening in silico. PLoS One 2011, 6: e15939.
12. Xu X, Zhang W, Huang C, et al. A novel chemometric method for the prediction of human oral bioavailability. Int J Mol Sci 2012, 13:6964-6982.
13. Wishart DS, Feunang YD, Guo AC, et al. DrugBank 5.0: a major update to the DrugBank database for 2018. Nucleic Acids Res 2018, 46: 1074-1082.
14. Tao W, Xu X, Wang X, et al. Network pharmacology-based prediction of the active ingredients and potential targets of Chinese herbal Radix Curcumae formula for application to cardiovascular disease. J Ethnopharmacol 2013, 145:1-10.
15. Li J, Zhao P, Li Y, et al . Systems pharmacology-based dissection of mechanisms of Chinese medicinal formula Bufei Yishen as an effective treatment for chronic obstructive pulmonary disease. Sci Rep 2015, 5: 15290.
16. Kohl M, Wiese S, Warscheid B. Cytoscape: software for visualization and analysis of biological networks.Methods Mol Biol 2011, 696: 291-303.
17. Hu Y, Scherngell T, Man SN, et al. Is the United States still dominant in the global pharmaceutical innovation network? PLoS One 2013, 8: e77247.
18. Uniprot CT. UniProt: the universal protein knowledgebase. Nucleic Acids Res 2018, 46: 2699.
19. Dennis GJ, Sherman BT, Hosack DA, et al. DAVID:database for annotation, visualization, and integrated discovery. Genome Biol 2003, 4: P3.
20. Huang DW, Sherman BT, Lempicki RA. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat Protoc 2009, 4:44-57.
21. Huang DW, Sherman BT, Lempicki RA.Bioinformatics enrichment tools: paths toward the comprehensive functional analysis of large gene lists.Nucleic Acids Res 2009, 37: 1-13.
22. Russi L, Scharl M, Rogler G, et al. The efficacy and safety of golimumab as third- or fourth-line anti-tnf therapy in patients with refractory crohn's disease: a case series. Inflamm Intest Dis 2017, 2: 131-138.
23. Ranson N, Veldhuis M, Mitchell B, et al. Nod-Like receptor pyrin-containing protein 6 (NLRP6) is up-regulated in ileal crohn's disease and differentially expressed in goblet cells. Cell Mol Gastroenterol Hepatol 2018, 6: 110-112.
24. Gu J, Liu G, Xing J, et al. Fecal bacteria from Crohn's disease patients more potently activated NOD-like receptors and Toll-like receptors in macrophages, in an IL-4-repressible fashion. Microb Pathog 2018, 121: 40-44.
25. Loren V, Cabre E, Ojanguren I, et al. Interleukin-10 enhances the intestinal epithelial barrier in the presence of corticosteroids through p38 MAPK activity in Caco-2 monolayers: a possible mechanism for steroid responsiveness in Ulcerative Colitis. PLoS One 2015,10: e130921.
26. Zhang D, Wang L, Yan L, et al. Vacuolar protein sorting 4B regulates apoptosis of intestinal epithelial cells via p38 MAPK in Crohn's disease. Exp Mol Pathol 2015, 98: 55-64.
27. Mizoyama Y, Takaki H, Sugihara N, et al. Inhibitory effect of flavonoids on N-acetylation of 5-aminosalicylic acid in cultured rat hepatocytes.Biol Pharm Bull 2004, 27: 1455-1458.
28. Habtemariam S, Belai A. Natural therapies of the inflammatory bowel disease: the case of rutin and its Aglycone, Quercetin. Mini Rev Med Chem 2018,18:234-243.
29. Ynag T, Zhong XX, He QY. Preliminary study on the treatment of chest arthralgia by he Qingyong associate professor with Yiyi Fzi Baijiang Powderr.Chin Tradit Med Emerg 2016, 5: 821-822.
30. Winges DM, Yao HQ, Li LR, et al. Professor Wang Qi, a master of Chinese medicine, on the treatment of prostate pain syndrome based on the "three discrimination mode". Chin J Tradit Chin Med 2016:3559-3562.
31. Jiang C Clinical application of professor Fu Yuanmou's Yiyi Fzi Baijiang Powderr. Sichuan Tradit Med 2013, 31: 119-120..
32. Li GT, Yan W. Treatment of 60 cases of chronic pelvic pain syndrome with modified Yiyi Fzi Baijiang Powder. J pract inter Medicine Tradit Chin Med 2007, 10: 64.
33. Kong LQ. Improvement of pain symptoms of typeⅲprostatitis by Dachaihu decoction and Yiyi Fzi Baijiang Powder Chin J Basic Chin Med 2016:1270-1272.
34. Wang BF, Zheng XP, Lu HY, et al. Effect of Yiyi Fzi Baijiang Powder Jiawei decoction on hemorheology and serum C-reactive protein in patients with chronic pelvic inflammatory disease. Zhejiang J Tradit Chin Med 2015: 792-793.
35. Li BY. 54 cases of chronic sinusitis treated by Yiyi Fzi Baijiang Powder and Qianjin Reed stem decoction combined with Platycodon grandiflorum.Nei Mongolia J Tradit Chin Med 2015, 34: 331-32.
36. Ding L. Clinical experience of Hao Ning in the treatment of gynecological diseases with Yiyi Fzi Baijiang Powder. Nei Mongolia J Tradit Chin Med 2017, 36: 59-60.
37. Zhang EG, Wang JQ. Clinical application of Yiyi Fzi Baijiang Powder in the treatment of gynecology. Nei Mongolia J Tradit Chin Med 2015, 34: 64.
38. Guo XQ, Zeng B. Treatment of 62 cases of chronic anal sinusitis with Yiyi Fzi Baijiang Powder and Taining suppository. Chin J surgery Integrat Chin Western Med 2010, 16: 72-73.
39. Chen YM, Zhang JH. Treatment of 48 cases of chronic cholecystitis with Yiyi Fzi Baijiang Powder.National Med Forum 1993, 5: 34.
40. Acikara OB, Citoglu GS, Dall'acqua S, et al.Bioassay-guided isolation of the antinociceptive compounds motiol and beta-sitosterol from Scorzonera latifolia root extract. Pharmazie 2014, 69:711-714.
41. Walker C, Oliveira SM, Tonello R, et al.Anti-nociceptive effect of stigmasterol in mouse models of acute and chronic pain. Naunyn Schmiedebergs Arch Pharmacol 2017, 390:1163-1172.
42. Ji C, Xu Y, Han F, et al. Quercetin alleviates thermal and cold hyperalgesia in a rat neuropathic pain model by inhibiting Toll-like receptor signaling.Biomed Pharmacother 2017, 94: 652-658.
43. Granado-serrano AB, Martin MA, Bravo L, et al.Quercetin attenuates TNF-induced inflammation in hepatic cells by inhibiting the NF-kappaB pathway.Nutr Cancer 2012, 64: 588-598.
44. Lee M, Yun S, Lee H, et al. Quercetin mitigates inflammatory responses induced by vascular endothelial growth factor in mouse retinal photoreceptor cells through suppression of nuclear factor Kappa B. Int J Mol Sci 2017, 18: pii: E2497.
45. Chen X, Yang X, Liu T, et al. Kaempferol regulates MAPKs and NF-kappa B signaling pathways to attenuate LPS-induced acute lung injury in mice. Int Immunopharmacol 2012, 14: 209-216.
46. Marazzi I, Greenbaum BD, Low D, et al. Chromatin dependencies in cancer and inflammation. Nat Rev Mol Cell Biol 2018, 19: 245-261.
47. Dou Z, Ghosh K, Vizioli MG, et al. Cytoplasmic chromatin triggers inflammation in senescence and cancer. Nature 2017, 550: 402-406.
48. Brito AF, Ribeiro M, Abrantes AM, et al. Quercetin in cancer treatment, alone or in combination with conventional therapeutics?. Curr Med Chem 2015,22: 3025-3039.
49. Shu Y, Xie B, Liang Z, et al. Quercetin reverses the doxorubicin resistance of prostate cancer cells by downregulating the expression of c-met. Oncol Lett 2018, 15: 2252-2258.
50. Sun S, Gong F, Liu P, et al. Metformin combined with quercetin synergistically repressed prostate cancer cells via inhibition of VEGF/PI3K/Akt signaling pathway. Gene 2018, 664: 50-57.
51. Wang J, Fang X, Ge L, et al. Antitumor, antioxidant and anti-inflammatory activities of kaempferol and its corresponding glycosides and the enzymatic preparation of kaempferol. PLoS One 2018, 13:e197563.
52. Cook MT. Mechanism of metastasis suppression by luteolin in breast cancer. Breast Cancer , 2018, 10:89-100.
53. Schwartzberg LS, Arena FP, Bienvenu BJ, et al. A randomized, open-label, safety and exploratory efficacy study of Kanglaite Injection (KLTi) plus gemcitabine versus gemcitabine in patients with advanced pancreatic cancer. J Cancer 2017, 8:1872-1883.
54. Fu F, Wan Y, Wu T. Kanglaite injection combined with hepatic arterial intervention for unresectable hepatocellular carcinoma: a meta-analysis. J Cancer Res Ther 2014, 10 Suppl 1: 38-41.
55. Du YL, Wang ZM, Lu DR, et al. Treatment of 33 cases of Colorectal Cancer with Yiyi Fzi Baijiang Powder combined with chemotherapy. Chin Tradit Med Sci Technol, 2015: 213-214.
56. Surdyka M, Slaska B. Defect in ND2, COX2, ATP6 and COX3 mitochondrial genes as a risk factor for canine mammary tumour. Vet Comp Oncol 2017, 15:1062-1072.
57. Misra S, Sharma K. COX-2 signaling and cancer:new players in old arena. Curr Drug Targets 2014,15: 347-359.
58. Chell S, Kaidi A, Williams AC, et al. Mediators of PGE2 synthesis and signalling downstream of COX-2 represent potential targets for the prevention/treatment of colorectal cancer. Biochim Biophys Acta 2006, 1766: 104-119.
59. Bertagnolli MM, Eagle CJ, Zauber AG, et al.Celecoxib for the prevention of sporadic colorectal adenomas. N Engl J Med 2006, 355: 873-884.
60. Pruthi RS, Derksen JE, Moore D, et al. Phase II trial of celecoxib in prostate-specific antigen recurrent prostate cancer after definitive radiation therapy or radical prostatectomy. Clin Cancer Res 2006, 12:2172-2177.
61. Xin X, Majumder M, Girish GV, et al. Targeting COX-2 and EP4 to control tumor growth,angiogenesis, lymphangiogenesis and metastasis to the lungs and lymph nodes in a breast cancer model.Lab Invest 2012, 92: 1115-1128.
 Traditional Medicine Research2018年6期
Traditional Medicine Research2018年6期
- Traditional Medicine Research的其它文章
- The role of Si-Jun-Zi decoction in the management of gastric precancerous lesions and its mechanism
- Recent advances in network pharmacology applications in Chinese herbal medicine
- A network pharmacology approach to investigate the mechanisms of Si-Jun-Zi decoction in the treatment of gastric precancerous lesions
- Analysis of the action mechanism of Fang Ji Huang Qi decoction in treating rheumatoid arthritis by network pharmacology
- Camel milk could be helpful in the treatment of asthma