
A Numerical Investigation of the Effects of Benign Paroxysmal Positional Vertigo on the Balance Function of the Inner Ear
2018-10-10 02:48ShenYuJizheWangYanGuoXiuzhenSunandShuangShen
Shen Yu, Jizhe Wang , Yan Guo , Xiuzhen Sun and Shuang Shen
Abstract: A three-dimensional numerical model of the membranous labyrinth of the semicircular canal of the inner ear was established to investigate the effects of canalithiasis of BPPV on the balance function of the inner ear. The movement of otolith particles in the membranous labyrinth was simulated when a person turns his head to a specific position. The effects of otolith movements on the balance function of the inner ear were simulated for different numbers, diameters, and initial positions of otoliths. The simulation results show that the otolith diameter affects the movement duration of otoliths in the membranous labyrinth. The number and diameter of otoliths, the diameter of the membranous labyrinth, and the initial position of the otoliths can cause changes in the pressure difference on both sides of the cupula of the crista ampullaris (cupula). The latent period and onset period are related to the diameter of otolith particles and the position of the head. There is also a correlation between the severity of the disease and the diameter and number of otolith particles.
Keywords: Benign paroxysmal positional pertigo, membranous labyrinth, cupula of the crista ampullaris, otolith.
1 Introduction
Benign paroxysmal positional vertigo (BPPV) is a self-limiting peripheral vestibular disease characterized by transient vertigo induced by head movements to a specific position accompanied by nystagmus. The main cause of canalithiasis of BPPV is the accumulation of detached otoliths in the membranous labyrinth of semicircular canal.When the head moves, the movement of otoliths disturbs the fluid-solid interaction between the endolymph and the cupula, causing vestibular dysfunction and subsequently dizziness symptoms. The detached otoliths are more commonly seen in the posterior semicircular canal. There will be a few seconds of latency before the onset, which is usually within 1 min. Many studies have been carried out on clinical diagnosis and treatment method. Diagnosis primarily relies on the electronystagmograph to extract nystagmus signals from patients and determine the affected semicircular canal [Zhou,Kong, Gao et al. (2017); Xiong, Wu, Liu et al. (2012); Liang, Sun, Peng et al. (2017)].Treatment involves a variety of reduction techniques that guide the detached otoliths back into the utricle and eliminate their effects on the cupula during head movement [Tian,Sheng and Wang (2016); Zou, Li, Wang et al. (2016); Xiong, Zhao, Liu et al. (2016)].Obrist et al. [Obrist, Hegemann, Kronenberg et al. (2010)] created a large single semicircular canal model to study the movement of otoliths in the semicircular canal.Mathematical models have been also developed to deduce the movement patterns of otoliths in a single semicircular canal [Squires, Weidmann, Hain et al. (2004); Obrist and Hegemann (2008); House and Honrubia (2003)]. Because the semicircular canal is buried deeply inside the temporal bone, non-invasive detection of is difficult. Therefore, certain phenomena such as latent period and onset period cannot be thoroughly understood,which limits the study of the disease. Therefore, a three-dimensional numerical model of the semicircular canal of the inner ear was established and the numerical simulation for the movement of otoliths in the canal during onset period was carried out. The entire movement process and its effects on the pressure difference between the two sides of the cupula were studied. Through simulation, this paper examines the role of otoliths in the onset of BPPV, as well as disease symptoms like the latent period and the onset period of the disease, with the aim of giving clinicians a deeper understanding of BPPV.
2 Materials and methods
Based on the geometric parameters of the semicircular canal in the right ear of a healthy volunteer (female, 67 years old, no history of ear disorders, no abnormal anatomical structure) provided by Ifedibaet et al. [Ifediba, Rajguru, Hullar et al. (2007)], the threedimensional numerical model was reconstructed consisting of three semicircular canals and three cupulas. Since the posterior semicircular canal is the main canal for the occurrence of canalithiasis, only the posterior semicircular canal structure was extracted from the three semicircular canals. The finite element model of the posterior semicircular canal was built with the software of Ansys Workbench, as shown in Fig. 1. The entire tubular structure is truncated by the cupula that is assumed undeformation. The model is meshed consisting of 56,517 tetrahedral elements and 12,789 nodes.
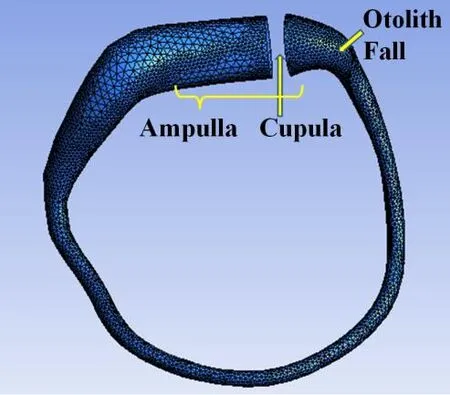
Figure 1: Finite element model of the posterior semicircular canal
Endolymph is considered to be an incompressible Newtonian fluid with a rigid wall. The physical parameters of the endolymph were obtained from literatures [Hain, Squires and Stone (2005)]. Endolymph density is 1000 kg/m3, Endolymph viscosity is 0.001 kg/m/s.The main component of otoliths is calcium carbonate and their density is approximately 2,700 kg/m3. Their shape is assumed to be spherical. The number and diameter of otolith particles are different in different patients. In this study, the number and diameter of otolith particles are set as 1-27 μm and 30-300 μm, respectively [Obrist, Hegemann,Kronenberg et al. (2010)]. Normally, the diameter of otolith particles will not reach 300 μm that is just an extreme case. Gravity and Stokes drag force are the main forces considered when otolith particles move in the endolymph.
BPPV is triggered by the movement of the head to a specific position. Detached otoliths move within the semicircular canal, causing microflows of the endolymph. The microflows cause the pressure difference to change on both sides of the cupula. The software of Workbench was used to perform numerical simulation and study the effects of the number, size, and location of otolith particles on the severity of disease.
3 Results
The patient moved from a sitting position to a lying position. When the patient is at rest,the otolith particles fall from the area near the ampulla (Fig. 2). First, the effects of otolith diameter are considered. The number of otolith particles in the membranous labyrinth is set to 1. The otolith diameters were set to 30 μm and 300 μm. Fig. 3(a) shows that when the 30 μm otoliths begin to fall from a location near the ampulla, the pressure difference between the two sides of the cupula is smaller. As time passes, the resulting pressure difference increases in the first 4 s and reaches to the peak value at the 5th second. When the otolith diameter is 300 μm, the pressure difference across the cupula is relatively small when the otoliths start to fall from a point near the ampulla. Then, the pressure difference quickly increases to its peak value within a short time and then rapidly decreases until it becomes zero (Fig. 3(b)). Throughout the process, the pressure difference generated by 300 μm otoliths is much larger than that generated by 30 μm otoliths.

Figure 2: Otolith particles movement

Figure 3: Effects of different otolith sizes on the pressure difference across two sides of the cupula. (a) The otolith diameter is 30 μm. (b) The otolith diameter is 300 μm
To examine the influence of the number of otolith particles, the otolith diameter was set to 30 μm and the number of otoliths was set to 1, 8, and 27. As shown in Fig. 4, variation patterns of the pressure difference between the two sides of the cupula over time is similar in all three cases. When the otoliths begin to fall from a location near the ampulla,the resulting pressure difference is smaller. As the otoliths move, the pressure difference increases until it reaches its peak value; the time to reach the peak value is almost 5 s.Subsequently, the pressure difference starts to decrease. However, the different number of otoliths caused different pressure difference. When the number of otoliths is small, the pressure difference is small, and vice versa.
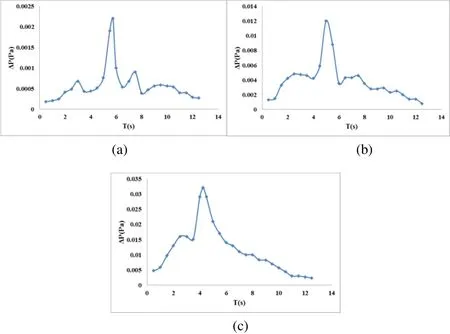
Figure 4: Effects of different otolith number on the pressure difference across two sides of the cupula. (a) Effects of 1 otolith. (b) Effects of 8 otoliths. (c) Effects of 27 otoliths
To study the effects of the initial location of otolith particles, the otolith diameter was set to 30 μm and the number of otoliths was set to 1. Two cases are considered here. The first case is that the patient moves from the sitting to the lying position and the otolith particles fall from the position near the ampulla into the canal. The second case is that the patient moves from the lying to the sitting position and the otolith particles fall from the canal. The Fig. 5(a) shows the resulting pressure difference in the first case, while the Fig.5(b) shows the resulting pressure difference in the second case. By comparing the two graphs, it can be seen that from the first case, a smaller pressure difference is generated during the first 4 s as otolith particles descend and the pressure difference suddenly increases to its maximum in approximately 5 s. In the second case, during otolith motion,the pressure difference rapidly increases to its peak value and then slowly decreases.Thus, different initial positions of the otolith result in different pressure difference.
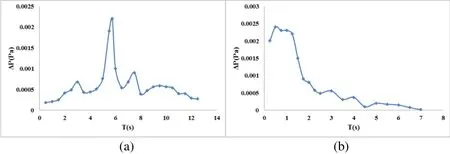
Figure 5: Effects of otolith particles on the pressure difference across two sides of the cupula. (a) Movement from sitting to lying. (b) Movement from lying to sitting
Two cases were compared to study the effects of otolith particles volume. The diameter and number of otoliths were set as 30 μm and 8, and 60 μm and 1, in the first and second case, respectively. The total volume of eight 30-μm otolith particles is equal to that of a single 60 μm particle. Fig. 6 shows that the pressure difference produced by eight 30 μm otoliths is significantly greater than that created by the single 60 μm otolith, despite the fact that the total volume is the same in the two cases. In other words, the pressure difference produced by large otoliths after fragmentation is greater than that by a single complete otolith.

Figure 6: Effects of otolith shape on the pressure difference across two sides of the cupula
4 Discussion
BPPV is a mechanical disorder of the vestibular system. When head moves to a specific position and stops moving, the otoliths will continue to move because of gravity in the membranous labyrinth of semicircular canal. The pressure difference is produced on both sides of the cupula to deform the cupula, and then causes vertigo. Different numbers,diameters, and initial positions of otoliths will affect the deformation of the cupula by affecting the pressure difference on both sides of the cupula. When the pressure difference is small, the cupula deformation is small, which is corresponding to the latent period. When the pressure difference is large, the cupula deformation is large, which is corresponding to the onset period.
By comparing the results of otolith particles of different diameters, it is noted that with the same number of otoliths, the pressure difference produced by the otoliths movement is directly proportional to the otoliths diameter. A larger otolith diameter causes greater disturbance to the surrounding endolymph during motion, which results in a greater pressure difference acting on the cupula. From the movement time, otoliths with small diameter move for a relatively longer time in the endolymph because the viscous force of the fluid acting on the smaller otoliths closer to the gravity as the otoliths fall. When the falling speed reaches to a certain value, it will approach a uniform movement. Therefore,the smaller otoliths will move for a longer time than the larger one and the pressure difference will last longer. Because of their small diameter, otolith particles will have relatively small impact on the cupula as they first begin to move in the ampulla. When the small otolith particles enter into the narrow part of the canal, they will produce a lager pressure difference. When larger-diameter otoliths fall, the gravity is much greater than the other forces acting on them. Thus, they will quickly fall to the bottom of the canal and the duration of pressure difference is also shorter. Hence, it can be seen that the latent period and onset period of BPPV are directly related to the size of otolith particles. Hain et al. [Hain, Squires and Stone (2005)] established a mathematical model to studying otolith motion in endolymph and drew a similar conclusion. This can explain why latent periods and onset periods are different among BPPV patients.
For patients with BPPV, the vary pattern of pressure difference with time is different as their positions change from sitting to lying and from lying to sitting. The great pressure difference appears at a later time when the patient moves from the sitting to lying position. From the description of clinical patients and the results of nystagmus measurements, it shows that the latent period is different in these two positions. When the patients move from sitting to lying, he will begin to feel dizzy after a few seconds. When the patients move from lying to sitting, the latent period is shorter. It can be seen that the latent period of BPPV is related to the change style of body position.
The ampulla at ends of the membranous labyrinth is inflated and its diameter is relatively large. Meanwhile, the canal in the middle part is relatively thin and the diameter is relatively small. When otolith particles begin to fall from the ampulla, the disturbance in the endolymph due to otolith motions has little effects on the pressure difference because the ampullary part is relatively enlarged. The effect gradually increases when the otoliths fall to the thinner portion. When the number of otoliths is large, a piston-like effect results and a large pressure difference is generated on both sides of the cupula.
Both the number and total volume of otolith particles will influence the pressure difference. This is because the number of otoliths directly affects the magnitude of disturbance of the otoliths to the endolymph as they fall. The more otoliths there are, the greater the disturbance is in the fluid. The effect of viscous drag is very important among the interactions between otoliths and endolymph. When a large-diameter otolith breaks into multiple small otoliths, its surface area increases and the viscosity drag also increases.Therefore, when a larger otolith breaks into many small otoliths the effects of the motion are greater than that of the single larger one. This is in agreement with the mathematical analysis of Hain et al. [Hain, Squires and Stone (2005)]. Therefore, it can be considered that the latent period and onset period of BPPV patients are related to the size of otolith particles and the severity is related to the number of otoliths.
From the above analysis, it can be observed that the latent period and onset period of BPPV are related to the size, number, location, and motion mode of otoliths in the membranous labyrinth. The otoliths in a patient’s membranous labyrinth may have different numbers and diameters, which cannot be measured directly. According to the results obtained, it is possible to deduce the condition of detached otoliths in the membranous labyrinth based on the latent period and onset period of BPPV. This allows a more accurate judgment of the patient’s condition and aids in treatment.
5 Conclusions
During the onset of BPPV, when the patient changes position from sitting to lying down,otoliths fall from the ampulla of the membranous labyrinth. The pressure difference on both sides of the cupula of the crista ampullaris is related to the volume, number, location,and motion mode of the otolith particles in the membranous labyrinth. A larger pressure difference occurs when the otolith particles are larger, but the pressure difference duration is shorter. When the otolith particles are relatively small, a smaller pressure difference will emerge for a few seconds, followed by a greater pressure difference with a longer duration. The pressure difference is greater with larger number of otolith particles.With the same total otolith volume, the pressure difference due to broken otoliths is larger than that caused by a complete otolith. Different motion ways will cause the variation patterns of pressure difference. Comparing the results of two positions transformation mode, the patients will experience a higher pressure difference in a very short time from lying down to sitting position. The above studies may have certain auxiliary benefits in the clinical diagnosis and treatment of BPPV.
Acknowledgment:This study was founded by the National Nature Science Foundation of China (11572079, 11772087, 31500765, 11472074, 11372069). These supports are acknowledged gratefully.
 Computer Modeling In Engineering&Sciences2018年8期
Computer Modeling In Engineering&Sciences2018年8期
- Computer Modeling In Engineering&Sciences的其它文章
- Angle of Attack Between Blood Flow and Mitral Valve Leaflets in Hypertrophic Obstructive Cardiomyopathy: An In Vivo Multipatient CT-based FSI Study
- The Analysis of Wall Shear Stress Modulated by Acute Exercise in the Human Common Carotid Artery with an Elastic Tube Model
- Hemodynamics of Enhanced External Counterpulsation with Different Coronary Stenosis
- A Fast-Fractional Flow Reserve Simulation Method in A Patient with Coronary Stenosis Based on Resistance Boundary Conditions
- Influence of Clip Locations on Intraaneurysmal Flow Dynamics in Patient-specific Anterior Communicating Aneurysm Models with Different Aneurysmal Angle
- Computational Fluid Dynamics Analysis of Shroud Design on Hemodynamic Performance and Blood Damage in a Centrifugal Blood Pump