免冲洗皮肤清洁剂在失禁性皮炎预防护理中应用效果的Meta分析
2018-06-07 09:17张晓雪王欣然
卫生职业教育 2018年11期
张晓雪,张 宇,王欣然
(首都医科大学宣武医院,北京 100053)
失禁性皮炎(IAD)是指因皮肤长期暴露在大小便中引起的炎症,常发生在外阴、臀部、大腿上部等区域[1,2]。失禁性皮炎患者会出现极度不适感,治疗费时且成本极高[3]。已有数据显示,IAD患者普遍存在于各医疗机构,患病率达5.6%~50.0%[4~7],发病率达3.4%~25.0%[8~10]。皮肤护理是护理工作的重要内容,失禁性皮炎的预防和护理对医务人员来说是一个巨大的挑战。
失禁是失禁性皮炎的主要风险因素[4],失禁患者的皮肤清洁是皮肤护理中最具挑战性的[11]。传统方法是利用肥皂和水进行肛周皮肤清洁[12]。研究显示,高pH值的皮肤清洁剂会使皮肤角质层充水,改变脂质硬度,增加皮肤损伤风险[13],而毛巾可造成摩擦损害,进而损伤皮肤屏障功能[14]。另外,清洁本身也会破坏皮肤的屏障功能,因此要在清除由失禁产生的刺激物和预防或最大限度降低因清洁造成的刺激之间取得平衡。有研究显示,免冲洗皮肤清洁产品结合洗涤剂和表面活性剂可以清除皮肤表面污物,很多产品含有保湿成分,有利于保持皮肤水分、保护皮肤屏障功能[15]。本研究收集免冲洗皮肤清洁剂用于失禁性皮炎皮肤护理的随机对照试验和类试验研究,通过Meta分析,探讨免冲洗皮肤清洁剂在失禁性皮炎预防与护理中的应用效果,为临床提供可靠依据。
1 资料与方法
1.1 文献检索策略
检索自建库至2017年6月公开发表的中英文随机对照试验(RCT)和类试验研究,不包含未公开出版的灰色文献,中文以“失禁/失禁性皮炎/尿布皮炎/尿布疹”“免冲洗皮肤清洁剂/一次性清洁产品”为关键词,在中国期刊全文数据库(CNKI)、万方数据知识服务平台检索。英文以“incontinence/incontinence associated-dermatitis/incontinence injury/incontinence lesion/incontinence sore/moist*lesion/moist*injury/moist*wound/most*damage”“skin protect*/skin product*/skin clean*/washcloth/no-rinse clean*”为检索词在 Cochrane Library,Medline,Web of Science,CINAHL 和EMBASE数据库检索。
1.2 纳入标准
1.2.1 研究设计 采取随机对照试验或类试验研究。
1.2.2 研究对象 纳入标准:(1)住院患者;(2)年龄≥18 岁;(3)失禁患者或已发生IAD的患者。
1.2.3 干预措施 试验组:采取免冲洗皮肤护理策略,包括使用免冲洗皮肤清洗剂或其他免冲洗皮肤清洁产品;对照组:进行常规皮肤清洗护理。
1.2.4 结局指标 失禁性皮炎患病率,护理人员清洁皮肤所花费的时间,失禁性皮炎严重程度。
1.3 排除标准
有下列情况之一的文献即被排除:未介绍免冲洗产品名称及使用方法或随访时间不明确;未获得原文且摘要提供信息不足,导致原始数据无法转换和应用。
1.4 文献筛选和资料提取
根据研究内容设计标准化资料提取表,内容包括文献基本信息、研究设计、研究对象、样本量、试验组和对照组干预方法,失禁性皮炎诊断标准、主要结局指标及评价标准等。由两名研究人员根据纳入标准进行文献筛选,之后交叉核对,如有异议,通过讨论或由第三名研究人员裁决。
1.5 文献质量评价
由两名研究人员按照Cochrane Handbook Version 5.1.0手册的质量评价标准进行评价,包括随机方法是否正确、是否分配隐藏、是否为盲法、结局指标数据的完整性和研究结果是否偏倚。独立评价文献质量后,两名评价员根据上述标准对文献质量进行讨论,达成共识后形成最终文献质量评价(见图1、2)。

图1 纳入文献偏倚情况

图2 纳入文献偏倚风险
1.6 统计学分析
采用RevMan 5.3软件对资料进行综合分析。分类变量以比值比(OR)和95%CI为指标进行分析,连续性变量以均数(MD)及其95%CI为指标进行分析。进行异质性检验,P>0.1以固定效应模型进行描述;P<0.1为研究间存在异质性,以随机效应模型进行描述,检验水准为0.05。
2 结果
2.1 文献检索结果
共检索到文献5 133篇,剔除不同数据库中重复发表和交叉的文献545篇;通过阅读文章题目、摘要初筛文献50篇,进一步阅读全文,排除不符合纳入标准的文献后最终纳入文献6篇,文献筛选流程见图3。
2.2 纳入研究的方法学质量分析
纳入分析的6篇文献质量差异较大,只有一篇文献质量较高,为 A 级,5 篇[11,14,15~18]文献质量中等,为 B 级。6 篇文献均比较了患者基线资料,纳入研究基本特征见表1,方法学质量评价见表2。
2.3 Meta分析结果
2.3.1 使用免冲洗皮肤清洁剂对IAD患病率的影响 6篇文献中有两篇[14,17]随机对照试验以IAD患病率作为结局指标,同质性检验P=0.96,I2=0%,采用固定效应模型进行Meta分析(见图4),合并效应有统计学意义(Z=4.04,P<0.01),显示使用免冲洗皮肤清洁剂对失禁患者进行皮肤护理,可以有效降低IAD风险。
2.3.2 使用免冲洗皮肤清洁剂对皮肤护理时间的影响 6篇文间,减少护理人员工作量。

图3 文献筛选流程
3 讨论
本研究共纳入6篇文献,分别研究使用免冲洗皮肤清洁剂对IAD患病率及皮肤清洁时间的影响。我们发现,目前国内外对于失禁性皮炎的研究均不深入,由于失禁性皮炎概念提出较晚,医学界尚未统一其名称以及判断方法,导致研究结果差异较大,这也是本研究纳入文献数量有限以及文献异质性的主要原因。
3.1 降低失禁性皮炎风险及患病率
失禁性皮炎是因皮肤长期或反复暴露在大小便中引起的皮肤损伤。失禁是失禁性皮炎的独立危险因素[19],尿液、粪便中的水分进入角质细胞,导致角质层结构紊乱,水分过多可使刺激因子穿透角质层引起炎症[20]。传统的皮肤护理方法是,患者失禁后,医护人员使用标准肥皂、水和毛巾清洁皮肤,去除尿液、粪便和其他污物。但是,标准肥皂为碱性,可改变皮肤pH值,损伤角质细胞,破坏皮肤屏障功能[14],而毛巾的摩擦作用可进一步破坏皮肤屏障功能。另外,单独用水清洁也可破坏皮肤屏障功能,这一点已通过TEWL(被认为是屏障功能的敏感指标)的升高得以证实[21]。我们纳入的研究也证明,使用免冲洗皮肤清洁剂可以减轻对皮肤屏障功能的损害,避免失禁性皮炎发生。同时,文献[14]还建议使用接近正常皮肤pH值的产品进行清洁。目前,临床上多使用一次性湿巾配合清水清洁皮肤,免冲洗皮肤清洁剂由于价格昂贵以及传统清洁习惯的影响使用并不广泛。2015年,世界IAD专家小组的报告指出,在可能的情况下建议使用无需清洗的皮肤清洁剂;在没有皮肤清洁剂的情况下,可以使用温和型肥皂和清水清洁;如果没有温和型肥皂,则建议用清水清洁。
3.2 能够缩短皮肤清洁护理时间,减少护理人员工作量
2015年,世界IAD专家小组的报告提出失禁患者结构性皮肤护理方案,主要包括两项措施:清洁皮肤和保护皮肤。清洁献中有两篇[16,17]随机对照试验以皮肤清洁时间作为结局指标,同质性检验P<0.01,I2=97%,采用随机效应模型进行Meta分析(见图 5),合并效应有统计学意义(Z=2.30,P=0.02),说明使用免冲洗皮肤清洁剂对失禁患者进行皮肤护理,可以缩短清洁时皮肤是结构性护理的第一步,也是失禁皮肤护理中最耗时的一步。使用免冲洗皮肤清洁剂后,皮肤表面快速干燥。多项研究也证实,使用免冲洗皮肤清洁剂可以节省护理时间,提高工作效率[17,22,23],提高治疗效果,提升患者满意度[24]。

表1 纳入研究文献的基本特征

表2 纳入研究文献的方法学质量评价
[1]Savik K,Fan Q,Bliss D,et al.Preparing a large data set for analysis:using the Minimum Data Set to study perineal dermatitis[J].Journal of Advanced Nursing,2005,52(4):399-409.
[2]Nix D,Haugen V.Prevention and management of incontinence associated dermatitis[J].Drugs Aging,2010,27(6):491-496.
[3]Doughty D,Junkin J,Kurz P,et al.Incontinence-associated dermatitis:consensus statements,evidence-based guidelines for prevention and treat-ment,and current challenges[J].J Wound Ostomy Continence Nurs,2012,39(3):303-315.

图4 使用免冲洗皮肤清洁剂对IAD患病率的影响
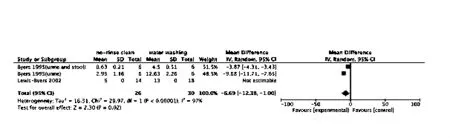
图5 使用免冲洗皮肤清洁剂对皮肤清洁时间的影响
[4]Bliss D Z,Savik K,Harms S,et al.Prevalence and correlates of perineal dermatitis in nursing home residents[J].Nurs Res,2006,55(4):243-251.
[5]Junkin J,Selekof J L.Prevalence of incontinence and associated skin injury in the acute care inpatient[J].J Wound Ostomy Continence Nurs,2007,34(3):260-269.
[6]Gray M,Beeckman D,Bliss D Z,et al.Incontinence-associated dermatitis:a comprehensive review and update[J].J Wound Ostomy Continence N-urs,2012,39(1):61-74.
[7]Campbell J L,Coyer F M,Osborne S R.Incontinence-associated dermatitis:a cross-sectional prevalence study in the Australian acute care hospital setting[J].Int Wound J,2016,13(3):403-411.
[8]Bliss D Z,Zehrer C,Savik K,et al.An economic evaluation of four skin damage prevention regimens in nursing home residents with incontinence-Economics of skin damage prevention[J].Journal of Wound Ostomy and Continence Nursing,2007,34(2):143-152.
[9]Long M A,Reed L A,Dunning K,et al.Incontinence-associated dermatitis in a long-term acute care facility[J].Journal of Wound Ostomy&Continence Nursing,2012,39(3):318-327.
[10]Borchert K,Bliss D Z,Savik K,et al.The incontinence-associated dermatitis and its severity instrument:development and validation[J].J Wound Ostomy Continence Nurs,2010,37(5):527-535.
[11]Brunner M,Droegemueller C,Rivers S,et al.Prevention of incontinence related skin breakdown for acute and critical care patients:comparison of two products[J].Urol Nurs,2012,32(4):214-219.
[12]Voegeli D.The effect of washing and drying practices on skin barrier function[J].Journal of Wound Ostomy and Continence Nursing,2008,35(1):84-90.
[13]Ananthapadmanabhan K P,Moore D J,Subramanyan K,et al.Cleansing without compromise:the impact of cleansers on the skin barrier and the technology of mild cleansing[J].Dermatologic therapy,2004(1):16-25.
[14]Beeckman D,Verhaeghe S,Defloor T,et al.A 3-in-1 perineal care washcloth impregnated with dimethicone 3%versus water and pH neutral soap to prevent and treat incontinence-associated dermatitis:a randomized,controlled clinical trial[J].J Wound Ostomy Continence Nurs,2011,38(6):627-634.
[15]Ersser S J,Getliffe K,Voegeli D,et al.A critical review of the interrelationship between skin vulnerability and urinary incontinence and related nursing intervention[J].Int J Nurs Stud,2005,42(7):823-835.
[16]Byers P H,Ryan P A,Regan M B,et al.Effects of incontinence care cleansing regimens on skin integrity[J].Journal of wound,ostomy,and continence nursing:official publication of The Wound,Ostomy and Continence Nurses Society,1995,22(4):187-192.
[17]Lewis Byers K,Thayer D.An evaluation of two incontinence skin care protocols in a long-term care setting[J].Ostomy Wound Manage,2002,48(12):44-51.
[18]Schoonhoven L,Van Gaal BGI,Teerenstra S,et al.Cost-consequence analysis of“washing without water”for nursing home residents:A cluster randomized trial[J].International Journal of Nursing Studies,2015,52(1):112-120.
[19]Black J M,Gray M,Bliss D Z,et al.MASD part 2:incontinence-associated dermatitis and intertriginous dermatitis:a consensus[J].J Wound Ostomy Continence Nurs,2011,38(4):359-370.
[20]Ichikawa Shigeta Y,Sugama J,Sanada H,et al.Physiological and appearance characteristics of skin maceration in elderly women with incontinence[J].Journal of Wound Care,2014,23(1):18-19.
[21]Voegeli D.Moisture associated skin damage:aetiology,prevention and treatment[J].Br J Nurs,2012,21(9):517-518.
[22]Beeckman D,Defloor T,Verhaeghe S,et al.What is the most effective method of preventing and treating incontinence associated dermatitis?[J].Nursing Times,2010,106(38):22-25.
[23]Warshaw E,Nix D,Kula J,et al.Clinical and cost effectiveness of a cleanser protectant lotion for treatment of perineal skin breakdown in lowrisk patients with incontinence[J].Ostomy Wound Manage,2002,48(6):44-51.
[24]Beeckman D,Schoonhoven L,Verhaeghe S,et al.Prevention and treatment of incontinence-associated dermatitis:litera ture review(Structured abstract)[J].Journal of Advanced Nursing,2009(65):1141-1154.
猜你喜欢
江苏安全生产(2022年8期)2022-11-01
保健医苑(2022年5期)2022-06-10
小资CHIC!ELEGANCE(2021年36期)2021-10-15
皮肤病与性病(2021年3期)2021-07-30
皮肤病与性病(2021年3期)2021-07-30
中国民间疗法(2020年22期)2021-01-07
艺术评鉴(2020年5期)2020-04-30
人大建设(2018年10期)2018-12-07
中国洗涤用品工业(2015年9期)2015-02-28
中国洗涤用品工业(2015年9期)2015-02-28