
Intravascular ultrasound guided retrograde guidewire true lumen tracking technique for chronic total occlusion intervention
2018-05-23 07:23:11LiangHongYINGYuanShengFANYiLUKeXUChunJianLI
Journal of Geriatric Cardiology 2018年2期
Liang-Hong YING, Yuan-Sheng FAN, Yi LU, Ke XU, Chun-Jian LI,*
1Department of Cardiology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, China
2Department of Cardiology, the Affiliated Huai’an Hospital of Xuzhou Medical University and Huai’an Second People’s Hospital, Huai’an, China
Chronic total occlusion (CTO) occurs in approximately 20% known coronary atherosclerotic lesions, and CTO intervention has become a most challenging work. Although retrograde techniques have been applied and significantly increased the success rate of CTO intervention, there are still some CTOs that cannot be opened. In this letter, we report a CTO intervention that both antegrade and retrograde reverse controlled antegrade and retrograde subintimal tracking (CART) techniques failed. However, a new intravascular ultrasound (IVUS) guided technique was proposed and successfully re-opened the left circumflex (LCX)CTO.
A 70-year-old male was admitted to hospital due to exertional chest pain for one year. The patient had no hypertension, neither diabetes, but a smoking history of 50 years. His baseline ECG was normal, and echo showed that his left ventricular diastolic diameter (LVDd) was 47 mm and left ventricular ejection fraction (LVEF) was 68.7%. Elective coronary angiography (CAG) showed normal left main(LM), and normal left anterior descending (LAD) coronary artery. However, the LCX was totally occluded, and the right coronary artery had severe and diffused lesions. The first percutaneous coronary intervention (PCI) was performed for the RCA, and three stents were successfully implanted.
LCX-CTO was then carefully evaluated and it revealed that the CTO had a blunt entry point, although its length was less than 20 mm, there should be some calcification and bending. Therefore, its Japanese CTO score was 2 to 3(Figure 1A). A good point is that there were two atrial branches connecting the posterior lateral branch of RCA and LCX with Rentrop collateral connections (CC) of 2ndgrade.
Second PCI was performed on 22ndAugust, 2017 for the LCX CTO. Antegrade approach was planned to be initiated and would switch to retrograde approach if the antegrade approach failed. 7F EBU3.5 (Medtronic, Minneapolis, MN,USA) (through right radial artery) was selected for left coronary artery (LCA) and 7F AL0.75 (Cordis Corporation,Miami Lakes, FL, USA) (through femoral artery) was selected for RCA. Under the support of Corsair 135 (Asahi Intecc Co., Seto, Aichi, Japan), antegrade approach was performed using successively Fielder-XT (Asahi Intecc Co,LTD, Aichi, Japan), Miracle-6 (M-6) (Asahi Intecc Co,LTD, Aichi, Japan), Pilot-200 (Abbott Vascular, Santa Clara, CA), and Conquest pro (Asahi Intecc Co., LTD, Aichi, Japan) guidewires. However, the CTO entry point was too hard and none of the guidewires penetrated into the CTO body (Figure 1B).
Then, retrograde approach was started, and one of the atrial branches was selected for retrograde wiring. Under the support of Corsair 150 (Asahi Intecc Co., Seto, Aichi, Japan), a Sion guidewire was successfully manipulated to distal LCX, and tip injection showed a blunt CTO exit point.M-6 guidewire was then selected and manipulated into CTO body and further to the entry point. IVUS (Volcano Corporation, Cordova, CA, USA) was then adopted to examine the position of the retrograde guidewire, which showed that the M-6 was in the subintimal layer (Figure 1C & 2A). After re-manipulating the guidewires, M-6 moved to the intra-plaque position (Figure 1D & 2B), thus the gap between the antegrade and retrograde guidewires was shortened.According to the distance between the two guidewires from the IVUS image, 2.5 mm Sprinter balloon (Medtronic, Minneapolis, MN, USA) was selected and reverse CART was performed. However, after several ballooning, the M-6 could not cross the plaque into the proximal true lumen.Then, Fielder-XT guidewire was selected and manipulated to distal LCX by knuckle technique, and reverse CART was re-tried distally and still failed (Figure 1D). At this time, a Guidezilla catheter (Boston Scientific, Marlborough, MA)was inserted under the assistance of anchor balloon, and IVUS was used to guide the manipulation of the retrograde guidewire. A Gaya-3 (Asahi Intecc Co., Seto, Aichi, Japan)guidewire was selected as the retrograde guidewire, IVUS catheter was pushed to the distal possible position of the antegrade guidewire (Figure 1E), which showed that the antegrade guidewire was in the subintimal layer, but the retrograde Gaya-3 was in true lumen (Figure 1E & 3A).Then we gradually pulled back the IVUS catheter (Figure 1F), and carefully manipulated the retrograde guidewire all the way through the true lumen to the proximal LCX under the guidance of IVUS. Finally, the retrograde Gaya-3 guidewire was successfully manipulated to proximal LCX and LM (Figure 1G & 3B-H).
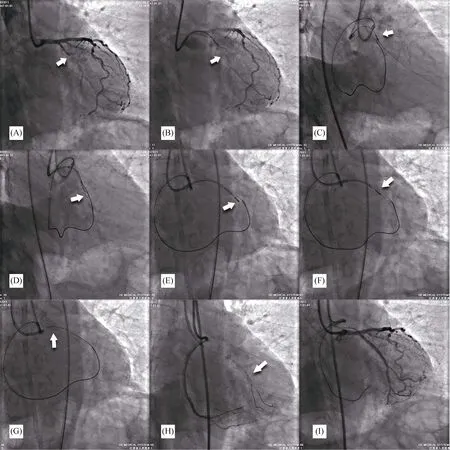
Figure 1. Images of LCX PCI. (A): LCX occlusion (arrow); (B): antegrade guidewire in false lumen (arrow); (C): retrograde guidewire in subintima proved by IVUS (arrow); (D): knuckled wire and reverse CART (arrow); (E): retrograde guidewire in true lumen proved by IVUS(arrow); (F): IVUS guided retrograde guidewire tracking (arrow); (G): Sumitsuji snare assisted retrograde guidewire externalization (arrow);(H): KDL catheter assisted antegrade guidewire placement (arrow); and (I): final result. CART: controlled antegrade and retrograde subintimal tracking; IVUS: intravascular ultrasound; LCX: left circumflex; PCI: percutaneous coronary intervention.

Figure 2. IVUS images of the retrograde guidewire. (A): Retrograde guidewire in subintima (arrow); and (B): retrograde guidewire in intra-plaque (arrow). IVUS: intravascular ultrasound.
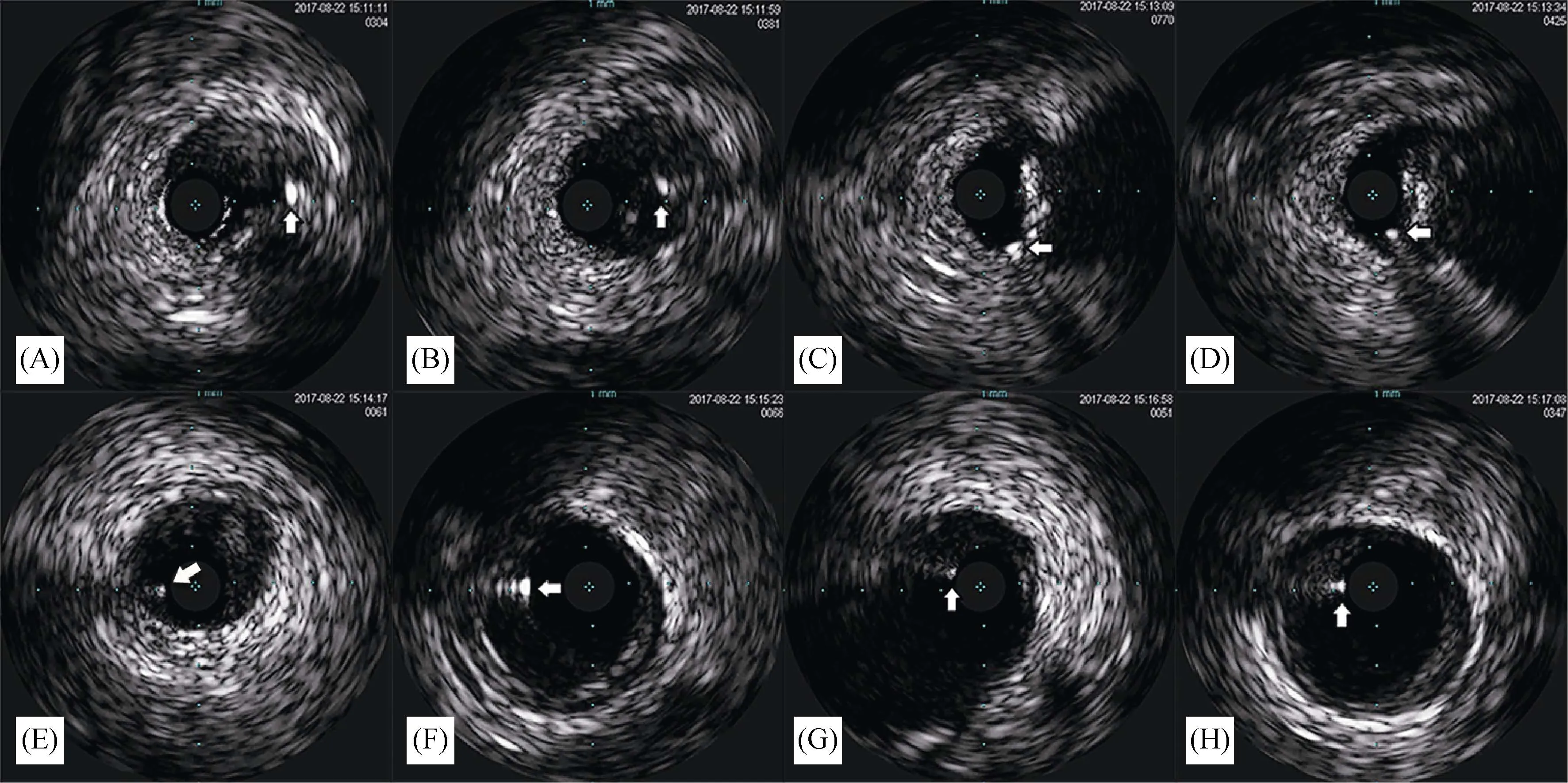
Figure 3. IVUS guided retrograde guidewire true lumen tracking. (A): distal LCX, antegrade guidewire in subintima (arrow); (B):distal LCX, retrograde guidewire in true lumen (arrow); (C)-(F): proximal LCX, both antegrade and retrograde guidewires in true lumen(arrow); (G): ostium LCX, both antegrade and retrograde guidewires in true lumen (arrow); and (H): LM, both antegrade and retrograde guidewires in true lumen (arrow). IVUS: intravascular ultrasound; LCX: left circumflex artery; LM: left main artery.
A Sumitsuji snare was made by the Guidezilla catheter, a Runthrough NC guidewire (Terumo Corporation,Tokyo,Japan), and a 2.0 × 20 mm Sprinter balloon (Medtronic,Minneapolis, MN, USA). Then the Gaya-3 guidewire was successfully pulled into the antegrade guiding catheter by the snare (Figure 1G). After balloon anchoring, the Corsair 150 was pushed into the antegrade guiding catheter, and a RG-3 (Asahi Intecc Co., Seto, Aichi, Japan) guidewire was used to accomplish the guidewire externalization. Two Runthrough NC guidewires were introduced to distal LCX and obtuse marginal (OM) using a Kaneka double lumen catheter (Kaneka Medix, Osaka, Japan) (Figure 1H). After pre-dilation, two Endeavor stents (Medtronic, Minneapolis,MN, USA) (2.25 × 30 mm and 2.25 × 24 mm) were successfully implanted under the support of the Guidezilla catheter. Finally, 2.5 × 9 mm Sprinter non-compliant balloon (Medtronic, Minneapolis, MN, USA) was adopted to perform the post-dilation. Final angiography showed TIMI III blood flow and IVUS proved good stent apposition (Figure 2).
During retrograde PCI, contemporary reverse CART is currently recommended if retrograde guidewire crossing fails.However, contemporary reverse CART may not always success even under the IVUS guidance,[1]and sometimes this could be caused by the inability of the pre-dilation bal-loon to make the fenestration force of the retrograde guidewire.[2]Conventional reverse CART with a larger balloon would be recommended in this situation. However, a larger balloon may cause larger dissection and hematoma which may affect the stent apposition, prolong the intima healing and even cause high risk of stent thrombosis or restenosis.
In this case, we proposed a new technique for CTO intervention while contemporary reverse CART failed, which we named as IVUS guided Retrograde guidewire True lumen Tracking (IVUS-RTT) technique. The key maneuver of this technique was pushing or knuckling the antegrade guidewire till or near the CTO exit point and introducing a IVUS catheter, by which we make sure that the retrograde guidewire started from the true lumen.[3]Then, the IVUS was pulled back step by step, and simultaneously the retrograde guidewire was pushed forward and manipulated under the guidance of the IVUS. Finally, the retrograde guidewire could be successfully manipulated all the way in true lumen to proximal coronary artery and consequently to antegrade guiding catheter. It was possible that the retrograde guidewire could be introduced into subintima as the IVUS catheter initially in. However, this would not affect the guidewire externalization unless the false lumen were too long. Besides, as reported by Ozawa N, many channels seem to spread out from the proximal side, tree-like, within the lesion, while in the retrograde approach, the wire is unlikely to enter these branch channels.[4]Our new technique would result in reduced interventional times, lower radiation, and minimized vascular damage as compared with conventional angiographic guided PCI and other re-entry techniques (e.g.,reverse CART).[5]
To the best of our knowledge, there is no data yet on the same technique as we report. Gutierrez-Chico JL and Numasawa Y have reported similar cases respectively, in which they both placed IVUS catheter in side branch near the CTO entry point which successfully guided the retrograde guidewire intimal tracking.[5,6]However, there would not have appropriate side branch in most CTO cases. Besides, side branch IVUS would be useless while the main trunk lesion is too long to be screened.
The IVUS-RTT technique would be best indicated for short CTO lesions as in this case. However, while antegrade dissection and reentry technique for long CTO lesion fails,this technique would also be indicated if the retrograde guidewire could be successfully introduced to the CTO exit point. In conclusion, IVUS-RTT is an effective technique for retrograde CTO intervention, which is suggested to be applied for short CTO intervention, or while reverse CART or ADR techniques fail.
References
1 Dai J, Katoh O, Kyo E, et al.Approach for chronic total occlusion with intravascular ultrasound-guided reverse controlled antegrade and retrograde tracking technique: single center experience.J Interv Cardiol2013; 26: 434–443.
2 Nakabayashi K, Okada H, Oka T. The use of a cutting balloon in contemporary reverse controlled antegrade and retrograde subintimal tracking (reverse CART) technique.Cardiovasc Interv Ther2017; 32: 263–268.
3 Dash D, Li L. Intravascular ultrasound guided percutaneous coronary intervention for chronic total occlusion.Curr Cardiol Rev2015; 11: 323–327.
4 Ozawa N. A new understanding of chronic total occlusion from a novel PCI technique that involves a retrograde approach to the right coronary artery via a septal branch and passing of the guidewire to a guiding catheter on the other side of the lesion.Catheter Cardiovasc Interv2006; 68: 907–913.
5 Gutierrez-Chico JL, Han SH, Jaguszewski M,et al.Intravascular ultrasound-guided retrograde percutaneous coronary intervention of a chronic total occlusion.Kardiol Pol2016; 74:793–794.
6 Numasawa Y, Motoda H, Yamazaki H,et al.Successful percutaneous coronary intervention of a chronic totally occluded left anterior descending artery via an ipsilateral intraseptal channel using intravascular ultrasound-guided retrograde wire-crossing technique.Cardiovasc Interv Ther2014; 29:157–161.
 Journal of Geriatric Cardiology2018年2期
Journal of Geriatric Cardiology2018年2期
- Journal of Geriatric Cardiology的其它文章
- Thyrotoxicosis induced cardiogenic shock rescued by extracorporeal membrane oxygenation
- Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
- Prediction of sudden death in elderly patients with heart failure
- Treatment of coronary in-stent restenosis: a systematic review
- Long term outcomes of drug-eluting stent versus coronary artery bypass grafting for left main coronary artery disease: a meta-analysis
- Adherence to pharmacological and non-pharmacological treatment of frail hypertensive patients