
血清OPG/RANKL比例与脑梗死病因亚型关系的研究
2018-05-14 17:00宫青赵洪芹
中外女性健康研究 2018年18期
关键词:NIHSS评分
宫青 赵洪芹

【摘 要】 目的:探討脑梗死患者血清中的骨保素(OPG)/核因子kappa B 受体活化因子配体(RANKL)比例与脑梗死病因亚型关系。方法:选取2016年2月至2018年1月青岛大学医学院附属医院神经内科住院的急性脑梗死患者中的157例,根据TOAST分型分为大动脉粥样硬化性脑梗死(LAA)和小动脉闭塞性脑梗死(SAO)两组,另外选取100例健康体检者作为对照组。采用酶联免疫吸附法(ELISA)分别检测三组血清中的OPG、RANKL水平,计算OPG/RANKL比例并比较;将同一病因亚型根据患者梗死体积分为大梗死组、中梗死组和小梗死组,比较三组血清中的OPG、RANKL水平及OPG/RANKL比例。结果:LAA组血清中OPG水平、OPG/RANKL比例均明显高于SAO组和对照组,LAA组血清中RANKL水平均明显低于SAO组和对照组,SAO组OPG/RANKL比例亦明显高于对照组,其差异均具有统计学意义(P<0.05)。在LAA中,大梗死组患者血清中OPG水平、OPG/RANKL比例均明显高于中梗死组和小梗死组,RANKL水平则明显低于中梗死组和小梗死组,中梗死组患者血清中OPG水平、OPG/RANKL比例均明显高于小梗死组,RANKL水平则明显低于小梗死组,其差异均具有统计学意义(P<0.05)。在SAO中,大梗死组SAO患者血清中OPG水平、OPG/RANKL比例均明显高于中梗死组和小梗死组,RANKL则明显低于梗死组和小梗死组;中梗死组SAO患者OPG/RANKL比例明显高于小梗死组,其差异均具有统计学意义(P<0.05)。结论:脑梗死患者血清中OPG/RANKL比例在LAA、SAO病因亚型患者中均随患者病情严重程度而增高,且不同病因亚型的OPG/RANKL比例存在明显差异,也许能够通过检测脑梗死患者血清中OPG、RANKL水平,计算OPG/RANKL比例判断其病情的严重程度。
【关键词】 大动脉粥样硬化性脑梗死;小动脉闭塞性脑梗死;NIHSS评分
Relationship between serum OPG/RANKL and cerebral infarction subtypes
Gong Qing1, Zhao Hongqin2
1.Department of Neurology, Affiliated Hospital of Qingdao University, Qingdao, Shandong 266071;
Department of Neurology, Weihai Wendeng District People's Hospital, Weihai, Shandong 264000
2.Department of Neurology, Affiliated Hospital of Qingdao University, Qingdao, Shandong 266071
[Abstract] Objective:To explore the relationship between the proportion of OPG/kappa B receptor activating factor ligand (RANKL) in the serum of cerebral infarction and the subtype of cerebral infarction. Methods: From February 2016 to January 2018, 157 patients with acute cerebral infarction admitted in the neurology department of hospital were divided into two groups: large atherosclerotic cerebral infarction (LAA) and arteriolo occlusive cerebral infarction (SAO). In addition, 100 patients were selected as the control group. The levels of OPG and RANKL in three groups of serum were detected by enzyme linked immunosorbent assay (ELISA), and the proportion of OPG/RANKL was calculated and compared. The same disease type was divided into large infarction group, middle infarction group and small infarction group according to the infarct volume. The OPG, RANKL level and OPG/RANKL ratio in the serum of the three groups were compared.Results: the serum level of OPG and OPG/RANKL in serum of LAA group were significantly higher than that in group SAO and control group. The level of RANKL in serum of LAA group was significantly lower than that of group SAO and control group, and the proportion of OPG/RANKL in SAO group was significantly higher than that in control group, and the difference was statistically significant (P<0.05). In LAA, the level of OPG and OPG/RANKL in the serum of the large infarct group were significantly higher than that of the middle infarction group and the small infarction group. The level of RANKL was significantly lower than that in the middle and small infarct groups. The level of OPG and the OPG/RANKL in the serum of the patients in the middle infarct group were significantly higher than those in the small infarction group, and the RANKL level was significantly lower than that of the small infarction group. All of them were statistically significant (P<0.05). In SAO, the serum levels of OPG and OPG/RANKL in the patients with SAO in the large infarct group were significantly higher than those in the middle and small infarct groups. RANKL was significantly lower than that in the infarct group and the small infarct group. The proportion of OPG/RANKL in the middle infarction group was significantly higher than that in the small infarction group, and the difference was statistically significant (P<0.05).Conclusion:The proportion of OPG/RANKL in the serum of patients with cerebral infarction increased with the severity of the patients in LAA and SAO etiological subtypes, and the proportion of OPG/RANKL
*赵洪芹为本文通讯作者
in different etiological subtypes was significantly different. It may be able to determine the severity of the disease by measuring the level of OPG and RANKL in the serum of the patients with cerebral infarction.
[Key words]Large atherosclerotic cerebral infarction; Small artery occlusive cerebral infarction; NIHSS score
据流行病学调查显示[1],我国急性脑梗死占全部脑卒中的70%左右,其中75%以上的患者因病致残,40%以上患者则会成为重度残疾,而脑梗死致死率则超过22%。目前,众多研究[2-3]认为OPG、RANK、RANKL三者共同构成一个系统或者信号通路,且血清中OPG、RANKL水平与脑梗死存在相关性。本研究通过观察不同TOAST病因分型脑梗死患者血清中的OPG、RANKL水平及OPG/RANKL比例变化,探索脑梗死早期诊断的新指标。
1 资料与方法
1.1 一般资料
选取2016年2月至2018年1月青岛大学医学院附属医院神经内科住院的急性脑梗死患者中的120例。纳入标准:所有入选患者均符合1995年全国第四届脑血管病学术会议修订的急性脑梗死的诊断标准,且年龄≥40岁;均经头颅磁共振成像(MRI)或CT确诊,且均有梗死病灶;患者首次发病且用药时间在发病72h内;所有患者的NIHSS评分显示均存在神经功能损伤。排除标准:排除不明原因及其他原因的脑梗死,例如动脉夹层、动脉炎、药物等因素导致的脑梗死;排除心、肝、肾功能明显不全者[4]。另外选取100例健康体检者作为对照组。三组研究对象在年龄、性别、吸烟史、糖尿病史等基线资料的差异无统计学意义(P>0.05),具有可比性。
1.2 研究方法
根据TOAST分型[5]将120例脑梗死患者分为大动脉粥样硬化性脑梗死(LAA)和小动脉闭塞性脑梗死(SAO)两组。其中LAA组74例,SAO组46将同一病因亚型根据患者梗死体积分为大梗死组(梗死体积>10cm3)、中梗死组(梗死体积为5~10cm3)和小梗死组(梗死体积<5cm3)。
1.2.1 OPG水平检测 患者禁食8h后,清晨采集其肘静脉血8mL,其中5mL放入4℃冰箱中,在2h内采用离心机以3000r/min的速度离心10min,分离血清置于EP管,标记后置于-80℃冰柜中备用。采用酶联免疫吸附法(ELISA)检测。往OPG抗体的包被孔中依次加入样品、标准品、HRP标记的检测抗体,经过恒温培育、洗涤后;用TMB显色(TMB在过氧化物酶的催化下呈现蓝色,酸化后最终呈现黄色),颜色的深浅与所测样品中的OPG浓度呈相关;将酶标仪的波長设置为450nm,测定样品的吸光度(OD值),并采用标准曲线计算其OPG的浓度。检测由具有3年以上检验经验的专业人员负责,并严格执行试剂的说明规范和操作
1.2.2 RANKL水平检测 RANKL的检测同OPG检测。
1.3 TOAST分型诊断标准
LAA:经颈动脉声波、血管造影或 MRA 检查,发现存在颈动脉闭塞或狭窄50%上,颅内、外的大动脉存在粥样硬化,皮质、小脑、脑干或皮质下梗死体积>1.5cm[6]。
SAO:患者影像学表现有以下任何一个临床症状即为SAO。1)有最大直径<1.5cm的腔隙性梗死灶;2)临床上有非典型腔隙梗死的症状,影像学检查未见对应病灶;3)临床上有非典型腔隙性梗死的症状,影像可见<1.5cm的病灶。
1.4 观察指标
观察LAA组、SAO组和对照组三组研究对象血清中OPG、RANKL水平及OPG/RANKL比例;观察不同梗死灶大小的LAA组、SAO组血清中的OPG、RANKL水平及OPG/RANKL比例。
1.5 统计学方法
采用SPSS 23.0统计软件进行处理,计量资料以均数±标准差(±s)表示,服从正态分布及方差齐时采用单因素方差分析检验,否则采用秩和检验;计数资料采用率表示,采用χ2检验。P<0.05为差异有统计学意义。
2 结果
2.1 三组研究对象血清中OPG、RANKL水平及OPG/RANKL比例。见表1。
表1 三组研究对象血清中OPG、RANKL水平及
OPG/RANKL比例(±s)
注:与SAO组、对照组比较,aP<0.05;与对照组比较,
bP>0.05;与对照组比较,cP<0.05
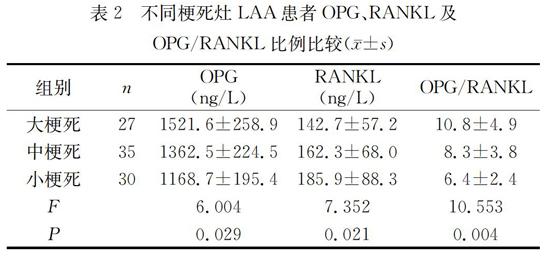
2.2 不同梗死灶LAA患者OPG、RANKL及OPG/RANKL比例。见表2。
表2 不同梗死灶LAA患者OPG、RANKL及
OPG/RANKL比例比较(±s)
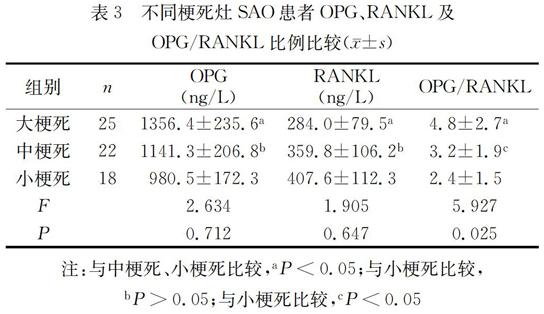
2.3 不同梗死灶SAO患者OPG、RANKL及OPG/RANKL比例。见表3。
表3 不同梗死灶SAO患者OPG、RANKL及
OPG/RANKL比例比较(±s)
注:与中梗死、小梗死比较,aP<0.05;与小梗死比较,
bP>0.05;与小梗死比较,cP<0.05
3 讨论
国外Stein JH[7]等研究发现,急性缺血性脑卒中患者血清重OPG水平明显高于正常对照组,且差异有统计学意义,说明OPG 可能参与了脑梗死的发病。国内李玲[8]等人的研究结果显示,动脉粥样硬化性脑梗死患者血清OPG水平明显高于健康对照组,差异有统计学意义,说明OPG参与了脑梗死的病发。凌芳[9]等人的研究结果也显示,易损斑块组急性脑梗死(AS)患者血清中的OPG水平均高于稳定斑块组,说明血清中的OPG水平与AS斑块的稳定性相关。目前,血清中OPG、RANKL水平与脑梗死病因亚型关系的研究很少。国内刘利宁[10]等人的研究显示:LAA型患者的动脉粥样硬化程度更为严重,血清中OPG水平最高。
本研究结果显示,LAA组血清中OPG水平、OPG/RANKL比例均明显高于SAO组和对照组,RANKL水平均明显低于SAO组和对照组,其差异均具有统计学意义(P<0.05);SAO组的OPG/RANKL比例亦明显高于对照组,其差异均具有统计学意义(P<0.05)。与王潇[11]、赵学谦[12]等人在LAA组和SAO组OPG水平的结论一致。本次研究说明,OPG、RANKL水平、OPG/RANKL比例与脑梗死的病因分型存在相关性,OPG/RANKL比例可能不但有助于脑梗死LAA和SAO病因亚型的分型,还有助于SAO的诊断。
本研究还显示,在LAA病因亚型患者中,大梗死患者血清中OPG水平及OPG/RANKL比例明显高于中梗死组和小梗死组患者,中梗死患者血清中OPG水平及OPG/RANKL比例明显高于小梗死患者,大梗死患者血清中RANKL水平明显低于中梗死组和小梗死组患者,中梗死患者血清中RANKL水平明显低于小梗死患者,其差异均具有统计学意义,这与目前的研究结论大体一致[13],说明LAA病因亚型患者血清中OPG、RANKL水平及OPG/RANKL比例與其病情严重程度相关;在SAO分型中,大梗死组SAO患者血清中OPG水平、RANKL水平、OPG/RANKL比例与中梗死组和小梗死组有明显差异(P<0.05),中梗死组SAO患者OPG/RANKL比例明显高于小梗死组(P<0.05),而中梗死组和小梗死组SAO患者血清中OPG、RANKL水平差异却无统计学意义(P>0.05),该研究结果不但显示SAO病因亚型患者血清中OPG、RANKL水平及OPG/RANKL比例与其病情严重程度,还显示OPG/RANKL比例更利于SAO病因亚型的早期诊断。
综上,血清中OPG、RANKL水平及OPG/RANKL与急性脑梗死患者TOAST病因亚型相关,且与病情严重程度相关,OPG/RANKL比例更利于病因亚型的诊断及病情严重程度的判断。
参考文献
[1] 中华医学会神经病学分会脑血管病学组急性缺血性脑卒中诊治指南撰写组.中国急性缺血性脑卒中诊治指南2010[J].中华神经科杂志,2010,02(02):16-19.
[2] Marley K,Bracha S,Seguin B.Osteoprotegerin activates osteosarcoma cells that co-express RANK and RANKL[J].Exp CellRes,2015,338(01):32-38.
[3] Pérez de Ciriza C,Lawrie A,Varo N.Osteoprotegerin in cardiometabolic disorders [J].Int J Endocrinol,2015,20(15):564-571.
[4] 陈艳洁,于文霞,王彦,等.丁苯酞注射液治疗急性脑梗死的疗效及对血清中sTRAIL、OPG和TNF-α的影响[J].现代中西医结合杂志,2014,23(23):2580-2582.
[5] 李文武.急性脑梗死TOAST分型尿激酶静脉溶栓治疗198例临床疗效分析[J].大理大学学报,2017,02(04):41-45.
[6] Adams H P Jr, Bendixen B H, Kappelle L J,et al.Classification of subtype of acute ischemic stroke.Definitions for use in a multicenter clinical trial TOAST Trial of Org 10172 in Acute Stroke Treatment[J].Stroke,2013,24(05):35-41.
[7] Stein J H,Korcarz C E,Hurst R T,et al.Use of carotid ultrasound toidentify subclinical vascular disease and evaluate cardiovascular disease risk:a consensus statement from the American society of echo cardiography Intima-Media thickness taskforce[J].Journal of the American Society of Echocardiography,2008,21(02):189-190.
[8] 李玲,杜秦川,马瑞莲,等.血清RANKL和脑梗死患者动脉粥样硬化性脑梗死的相关性研究[J].宁夏医学杂志,2016,38(06):487-488.
[9] 凌芳,李强,聂德云.急性脑梗死患者血清HMGB1、OPG和MIF水平的变化及PAS三联疗法的干预作用[J].中华脑血管病杂志(电子版),2014,06(02):87-89.
[10]刘利宁,王满侠,秦敏,等.急性脑梗死患者血清sTRAIL、OPG水平与TOAST亚型的关系[J].中风与神经疾病杂志,2015,28(02):141-144.
[11]王潇,冯娟.血清骨保护素水平与急性脑梗死病因亚型及严重程度的关系[J].中国神经医学杂志,2014,13(02):265-267.
[12]赵学廉,方敬献.急性脑梗死患者血清骨保护素含量的改变及其临床意义[J].国际老年医学杂志,2016,37(03):100-101.
[13]Sandberg W J,Yndestad A,Oie E,et al.Enhanced T -cell expression of RANK ligand in acute coronarysyndrome:possible role in plaque destabilization[J].Arterioscler Thromb Vasc Biol,2006,26(04):857-863.
猜你喜欢
中外医疗(2018年14期)2018-10-20
医学信息(2018年8期)2018-06-17
中国现代医生(2018年7期)2018-04-26
中国医学创新(2017年23期)2018-03-08
中国社区医师(2017年25期)2018-02-23
中国现代医生(2017年25期)2017-10-20
糖尿病新世界(2016年23期)2017-04-17
中外医学研究(2017年8期)2017-03-30
中国现代医生(2016年25期)2016-11-19
医学信息(2015年7期)2015-03-20
