
Heart Disease in Pregnancy: A Special Look at Peripartum Cardiomyopathy
2018-02-28 02:30DmitryYaranovMDandJeffreyAlexisMD
Dmitry Yaranov, MD and Jeffrey D. Alexis, MD
1 College of Medicine, University of Florida, Jacksonville, FL, USA
2 University of Rochester, Rochester, NY, USA
Abstract Peripartum cardiomyopathy (PPCM) is a disorder in which heart failure develops in the last month of pregnancy or within the f rst f ve months postpartum. The exact etiology is not known although recent studies suggest angiogenic imbalance is a key factor with soluble fms-like tyrosine kinase-1 (sFlt1) and a cleaved form of prolactin possibly playing important roles. This review discusses the epidemiology, risk factors, diagnosis, treatment and prognosis of PPCM and highlights recent advances in our understanding of this disorder.
Keywords: Peripartum ; cardiomyopathy ; heart failure
Introduction
Peripartum cardiomyopathy (PPCM) is a heart failure syndrome due to left ventricular systolic dysfunction that occurs between the late stages of pregnancy and the early postpartum period with poorly understood causes and pathogenesis [ 1, 2]. Although it resembles dilated cardiomyopathy, the clinical course is variable and outcomes differ signif cantly from those of other forms of cardiomyopathy [ 3]. PPCM affects women in different parts of the world, but with signif cant differences in clinical presentation, disease course, and outcomes [ 4, 5]. It remains one of the leading causes of maternal morbidity and death [ 6, 7].
PPCM was recognized as heart failure of pregnancy in the 19thcentury [ 8]; however, at that time it was not described as a separate form of cardiomyopathy [ 9 ]. The f rst case series was published in 1937 [ 10], but the term “ peripartum cardiomyopathy” was not used until 1971, when Demakis et al.[ 1] published a large case series and def ned the f rst diagnostic criteria (the development of heart failure in the last month of pregnancy or within fve months of delivery). The subsequent development of echocardiography led to the introduction of ejection fraction “ cutoff” into the new criteria in 1999 by a National Heart, Lung, and Blood Institute workshop[ 11]. At the same time a workgroup of the European Society of Cardiology updated the diagnostic criteria [ 12], and its most recent statement def nes PPCM as “ an idiopathic cardiomyopathy presenting with HF [heart failure] secondary to left ventricular(LV) systolic dysfunction towards the end of pregnancy or in the months following delivery, where no other cause of HF is found ” [ 13]. The lack of a precise def nition ref ects incomplete understanding of the disease. The aim of this review is to describe clinical characteristics, a novel hypothesis of pathogenesis, and outcomes of patients with PPCM.
Epidemiology
The incidence of PPCM in the United States ranges from 1 in 968 live births to 1 in 4350 live births [ 14 -17], with a mean of 1 in 3186 live births. Mielniczuk et al. [ 16] reported a trend toward an increase in incidence over time, from 1 in 4350 in 1990 to 1 in 2229 in 2000. The same trend was reported by Kolte et al. [ 17] in a population-based study of PPCM, with increasing incidence approaching 1 in 968 live births from 2004 to 2011. This increase in incidence could be explained by increased awareness and improved diagnostic abilities, as well as rising maternal age, changing demographics, and increase in multifetal pregnancies. Brar et al. [ 18]in a study from southern California concluded that the incidence of PPCM is dif ferent across dif ferent racial groups, the greatest incidence being in African Americans (1 in 1421), which is almost three times higher than in whites and seven times higher than in Hispanics ( Table 1 ). The high incidence of PPCM in African-American females in the United States was also conf rmed in other population studies [ 19, 20]. The incidence of PPCM in the United States differs by geographic region. It is lowest in the western states and highest in the south,where almost 50% of PPCM cases occur according to nationwide studies [ 17].
The incidence of PPCM outside the United States is less studied. The incidence tends to differ among geographic regions of the world. Wide variation in reporting may be due to differences in reporting patterns and diagnostic approaches. Reports suggest a high incidence of PPCM in Haiti and northern parts of Nigeria, with incidences of 1 in 299 live births and 1 in 100 live births, respectively [ 21, 22].A much lower incidence of PPCM is reported in Japan (1 in 6000 live births [ 2]) and South Africa (1 in 1000 live births [ 23]).
Etiology
The cause of PPCM remains unknown. PPCM is distinguished from other cases of idiopathic dilated cardiomyopathy by its temporal relationship to pregnancy. The exact pathophysiological mechanisms that lead to PPCM are poorly def ned.Many potential processes have been proposed as a cause of PPCM, such as viral myocarditis, abnormal immune response to pregnancy, maladaptive response to hemodynamic stresses of pregnancy,stress-activated cytokines, excessive prolactin excretion, and prolonged tocolysis. However,none of these are scientif cally proven to date [ 11,13 , 24 ] .
Recent animal and human data support a hypothesis of systemic angiogenic imbalance, accentuated by preeclampsia, as one of the potential mechanisms in the development of PPCM. Peroxisome proliferato-r activated receptor γ coactivator 1 α (PGC-1 α) is a transcriptional coactivator of metabolic programs in many tissues that stimulates the expression of angiogenic factors, such as vascular endothelial growth factor (VEGF), which leads to formation of new blood vessels [ 25, 26]. The lack of PGC-1 α has been linked to development of severe cardiomyopathy of pregnancy in knockout mouse models [ 27].The use of antiangiogenic therapies in oncology has been linked to development of dilated cardiomyopathy as a side effect of the therapy [ 28]. Late gestation is associated with placental secretion of VEGF inhibitors such as soluble fms-like tyrosine kinase-1(sFlt1), which also damages the vasculature. Higherlevels of sFlt1 are seen with multiple-gestation pregnancy or preeclampsia [ 29]. Among women with preeclampsia, subclinical cardiac dysfunction (as detected by the myocardial performance index) correlates with sFlt1 levels [ 30 - 32R ]e. cent analysis from the Investigations of Pregnancy-Associated Cardiomyopathy (IP AC) investigators demonstrated correlation of higher sFlt1 levels with the severity of symptoms and major adverse clinical events in patients with PPCM [ 33].

Table 1 Reported Incidence (Per 10,000 Live Births) of Peripartum Cardiomyopathy in the United States according to Race/Ethnicity.
Another novel mechanism of PPCM development is linked to the transcription factor signal transducer and activator of transcription 3 (ST AT3),cathepsin D, and prolactin. In a mouse model, myocardial STAT3 def ciency enhances the activity and production of cathepsin D, a peptidase that cleaves prolactin and converts it into its vasotoxic form,16-kDa prolactin [ 34 - 36C e].l lular accumulation of 16-kDa prolactin leads to cardiac endothelial cell apoptosis and development of PPCM in STAT3-def cient mice. Treatment with bromocriptine,which inhibits anterior pituitary prolactin secretion, completely reverses PPCM in these mice [ 35].Addition of bromocriptine to standard heart failure therapy in humans appeared to improve the composite clinical outcome in a proof-of-concept pilot study, which may support the proposed pathophysiological mechanism [ 37].
Although the position statement from the European Society of Cardiology classif es PPCM as a nonfamilial form of dilated cardiomyopathy[ 38], there has been evidence of PPCM as the initial manifestation of familial dilated cardiomyopathy and familial patterns of the disease [ 39 - 42].
Risk Factors
Older maternal age, multiparity, multifetal pregnancies, pregnancies complicated by preeclampsia and gestational hypertension, and African-American background have been identif ed as risk factors predisposing women to PPCM.
Although reported in women of all childbearing ages, PPCM tends to be more prevalent in older women (age greater than 30) with high parity and age extremes [ 2 - 41 , 3 , 23 , 43 ]. Although parity has been considered a risk factor for PPCM, not all studies have demonstrated such an association.
PPCM in the United States has been reported across dif ferent racial groups, with the highest prevalence among African Americans [ 19 , 20 ].Experts hypothesize that racial association might be confounded by the increased incidence of PPCM in females of lower socioeconomic status [ 2].
Hypertension and preeclampsia are strong risk factors for PPCM. The rates of hypertension among women with PPCM range from 29 to 68% in reports available in the United States [ 1 , 14 , 15 , 44 ]. More than 20% of patients have preeclampsia, which is four-fold higher than in the general population.
Multifetal pregnancy is a well-documented risk factor with an incidence of PPCM as high as 15%[ 1 , 14 , 15 , 44 , 45 ], well above the national average of 3% [ 46].
Diagnosis and Treatment
The initial signs and symptoms of PPCM are similar to those of pregnancy, which often leads to late recognition of the disease. Most patients present with a clinical picture of decompensated heart failure.Physical examination f ndings are often suggestive of volume overload. Electrocardiography may reveal sinus tachycardia and nonspecif c ST-T wave abnormalities, as well as left ventricular hypertrophy and left atrial enlar gement [ 14]. Chest X-ray may show vascular congestion, pulmonary edema, and cardiomegaly. Two-dimensional echocardiography shows decreased left ventricular ejection fraction and various degrees of left ventricular dilatation [ 3].Right ventricular dysfunction with various degrees of tricuspid regurgitation and elevated right ventricular systolic pressures may be seen. Brain natruretic peptide (BNP) levels do not normally signif cantly change during pregnancy. Signif cant elevation of BNP levels could help in establishing the diagnosis of PPCM in the appropriate clinical context as BNP levels may be markedly elevated in PPCM [ 47].
Generally, standard evidence-based medical therapies for heart failure with reduced ejection fraction management have been used for patients with PPCM. Although prospective data on optimal medical therapy are lacking, management is based on clinical experience and extrapolated data from heart failure with reduced ejection fraction trials. The goal of therapy is to alleviate symptoms, facilitate ejection fraction recovery, and prevent thromboembolic complications. Caution should be used when heart failure therapy is implemented during pregnancy and lactation.
Loop diuretics, particularly furosemide, are usually the preferred agents to control symptoms of volume overload; however, caution should be exercised, given the potential risk of hypotension and oligohydramnios. Conventional renin-angiotensin axis inhibition angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are used postpartum, but are contraindicated during pregnancy because of well-documented teratogenicity during the second and third trimesters. β -Blockade should be considered. Intrauterine growth restriction has been reported with β-blockers, but the maternal benef t is thought to outweigh the fetal risk[ 48]. Metoprolol tartrate may be favored, considering a more extensive clinical experience during pregnancy compared with other β -blockers.
As PPCM carries higher risk of thromboembolic events compared with other forms of dilated cardiomyopathy, anticoagulation is advisable at least during pregnancy and the f rst 2 months postpartum. The use of unfractionated heparin or low-molecular weight heparin is safe during pregnancy, and the former is preferred near term because of its shorter half-life.
Most heart failure medications, including enalapril, captopril, β-blockers, and spironolactone, are compatible with breastfeeding [ 49].
The use of bromocriptine, a prolactin antagonist, has been proposed by several investigators.Bromocriptine therapy is not currently approved for the treatment of PPCM. Its use is based on the hypothesis of cathepsin D-mediated cleavage of prolactin and excess of an angiotoxic form of prolactin. Several studies have tested the hypothesis in vivo. A recent multicenter randomized study supported a potential benef t of bromocriptine use;however, the study failed to reach its primary end point of demonstrating a superior e ffect of long-term bromocriptine treatment compared with short-term bromocriptine treatment on recovery of ejection fraction [ 50]. A possible benef t of bromocriptine is a hypothesis proposed by researchers but further research is necessary. Patients in whom bromocriptine use is considered should be well informed of the potential eff cacy, but also the limited data, possible side effects, and the value of breastfeeding.
Outcomes and Prognosis
Before 2015, data on outcomes and prognosis in patients with PPCM were limited and very heterogeneous, mainly because of the low number of patients in single-center studies and retrospective data [ 32]. The IPAC study published in 2015 was a multicenter, prospective study to evaluate clinical characteristics, treatment, and clinical predictors of outcomes in women with PPCM in North America.The study enrolled 100 women, and survival and event data were analyzed for 97 patients at 6 months and for 91 patients at 12 months. Although most women (72%) recovered with conventional ther-apy, the event rate remained unacceptably high. The overall event-free survival rate was 93%, but was signif cantly lower for those with initial ejection fraction below 30% (82% survival rate at 1 year)( Figure 1 ). The rate of event-free survival was similar between African Americans and Caucasians, but was much lower for women presenting with very low ejection fraction ( < 30%). African-American women demonstrated lower mean ejection fraction both at presentation and at the 12-month follow-up and less ejection fraction recovery overall [ 51].
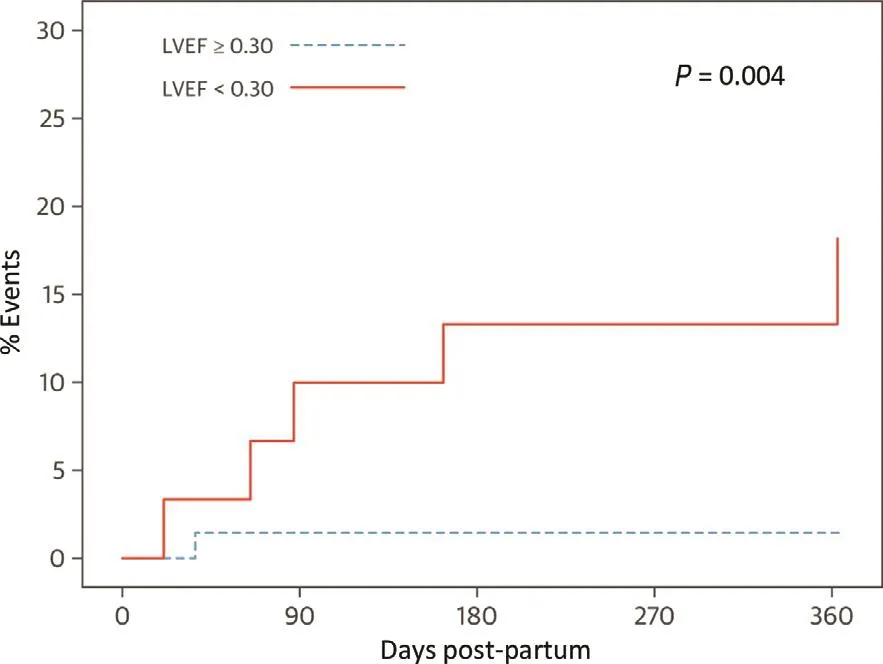
Figure 1 Event Rate by Baseline Left Ventricular Ejection Fraction.
Left ventricular ejection fraction and left ventricular end-diastolic dimension at presentation, race,body mass index, and time postpartum to presentation were the best clinical predictors of recovery at 12 months [ 51].
Conflict of Interest
The authors declare no conf ict of interest.
 Cardiovascular Innovations and Applications2018年4期
Cardiovascular Innovations and Applications2018年4期
- Cardiovascular Innovations and Applications的其它文章
- Challenges in Cardiovascular Risk Prediction and Stratification in Women
- Nonobstructive Coronary Artery Disease in Women: Risk Factors and Noninvasive Diagnostic Assessment
- Antiplatelet Therapy Considerations in Women
- Novel Imaging Approaches for the Diagnosis of Stable Ischemic Heart Disease in Women
- Psychosocial Stress, the Unpredictability Schema, and Cardiovascular Disease in Women
- Heart Failure with Preserved Ejection Fraction:Time to Revisit the Stiff Heart