
后路交叉置钉技术在青少年脊柱侧凸治疗中的应用
2017-09-02 06:40陈博昌
临床小儿外科杂志 2017年4期
张 彦 陈博昌 鲍 琨
后路交叉置钉技术在青少年脊柱侧凸治疗中的应用
张 彦 陈博昌 鲍 琨
目的探讨后路交叉置钉技术对于治疗青少年脊柱侧凸的临床疗效。 方法 2010年1月至2014年1月,68例青少年脊柱侧凸病例,男10例,女58例,年龄11~16岁,平均13.5岁;其中4例为神经肌肉型脊柱侧凸,其余为特发性脊柱侧凸;术前冠状面主弯Cobb角平均56.2°,胸椎(T5~T12)后凸角度平均17.7°,手术方法为后路交叉置入椎弓根螺钉对脊柱侧凸进行矫正,对术后Cobb角、主弯Cobb角矫正率结果进行评价。 结果 术后随访12~40个月,平均22.5个月。术后主弯Cobb角矫正到18.5°,与术前比较有差异(t=3.705,P<0.01),末次随访时平均20.2°,与术后比无差异(t=1.053,P>0.05)。胸椎(T5~T12)后凸角术后平均22.8°,末次随访时平均23.2°,术前与术后、术后与末次随访相比较均无差异(P>0.05)。术后主弯Cobb角矫正率为70.5%,而末次随访时虽然主弯矫正率(69.4%)有一定丢失,但和术后比较无差异(t=0.126,P>0.05)。术后无患者出现脊髓或神经根损伤。末次随访时无内固定松动及断钉断棒,植骨融合牢固,均未出现明显的矫正丢失。 结论 对于青少年脊柱侧凸后路手术矫正,采用交叉置钉技术是一项值得推广的低费用、高安全的脊柱侧凸矫正技术。
青少年;脊柱侧凸;外科手术;随访研究
全椎弓根螺钉技术是目前治疗青少年脊柱侧凸的主流技术,受到很多脊柱外科医生的欢迎。相比其他脊柱内固定方法有更好的三平面矫正效果。全椎弓根螺钉技术,具有融合节段少,术后矫正率丢失低,并发症少的优势[1-5]。但由于脊柱侧凸患者的椎体常出现严重旋转及变形,导致椎弓根钉置入风险大大增高,随着椎弓根钉置入数量的增加,其神经血管损伤的风险也相应增高[6,7]。同时,椎弓根钉置入数量增加势必会使手术费用提高,增加了患者家属接受手术治疗的经济负担。那么如何在矫正效果和手术并发症及治疗费用间寻找一个平衡点,本研究采用了后路交叉置钉技术来矫正青少年脊柱侧凸,在保证矫正效果的前提下,有效的减少了椎弓根置入数量,降低了病患的治疗费用及手术风险。
材料与方法
一、一般资料
2010年1月到2014年1月,本院共收治68例青少年脊柱侧凸病例,男10例,女58例,年龄11~16岁,平均13.5岁;其中4例为神经肌肉型脊柱侧凸,其余为特发性脊柱侧凸;术前Cobb角48°~82°,平均56.2°;胸椎(T5~T12)后凸角度17.7°±8.2°。
二、置钉原则及方法所有病例采用后路交叉
置入椎弓根螺钉方法进行校正,根据术前脊柱全长正侧位片及bending位片,确定远近端稳定椎和融合节段,螺钉数量根据“融合椎体节段数+4”作为用钉最高上限。上下稳定椎采用双节段两侧同时置钉建立框架结构,中间节段则采用交叉置钉方法布钉(图1)。靠近框架结构的椎体,若节段间侧向弯曲小于15°,该椎体螺钉省却。对于顶椎及椎体旋转严重的节段,在导航下置入椎弓根钉,提高置钉的准确性,保证手术安全。
置钉后,按脊柱生理后凸弧度弯棒,先后安装凹侧棒和凸侧棒,采用转棒和逆向转钉技术尽可能恢复椎体旋转。逐一调整钉棒距离并结合椎体去旋转技术对畸形进行三平面的矫正。
三、观察指标
术后定期在本院复查,行脊柱全长正侧位片检查。测量术前,术后及末次随访时冠状面主弯Cobb角,矢状面上胸椎(T5~T12)后凸角度。冠状面矫正率的计算方法为:(术前Cobb角~术后Cobb角)/术前Cobb角。
四、统计学分析
采用SPSS 18.0进行统计分析,Cobb角采用平均值±标准差(±s)表示,手术前后和末次随访与术后的的比较采用配对t检验。术后及末次随访矫正率的比较采用配对卡方检验。以P<0.05视为差异有统计学意义。
结 果
冠状面Cobb角术前48~82°,平均56.2°,术后4.2~35.5°,平均18.5°,末次随访4.5~30.4°,平均20.2°,术前与术后比有显著性差异(t=3.705,P<0.01),术后与末次随访相比无显著性差异(t=1.053,P>0.05)。胸椎(T5~T12)后凸角度从术前的17.7°±8.2°改善到术后的22.8°±6.5°,末次随访为23.2°±7.4,术前与术后,术后与末次随访相比较均无显著性差异(P>0.05),具体见表1。
表1 影像学参数和统计分析(±s)Table 1 Descriptive analyses of demographic and radiographic parameters(±s)

表1 影像学参数和统计分析(±s)Table 1 Descriptive analyses of demographic and radiographic parameters(±s)
冠状面Cobb角(°)胸椎后凸Cobb角(°)主弯矫正率(%)术前56.2±4.8 17.7±8.2术后 18.5±6.9 22.8±6.5 70.5±6.5末次随访 20.2±8.2 23.2±7.4 69.4±10.5术前vs术后 t=3.705,P=0.0004148术后vs末次随访 t=1.053,P=0.296 t=1.464,P=0.t=0.102,P=0.919 t=0.126,P>0.05
术后无患者出现脊髓或神经根损伤。术后主弯Cobb角矫正率为70.5%,而末次随访时虽然主弯矫正率69.4%)有一定丢失,但和术后比较无显著性差异(t=0.126,P>0.05)。随访时间12~40个月,平均22.5个月,无内固定松动及断钉断棒,植骨融合牢固(图2)。
讨 论
椎弓根螺钉技术近二十年来逐渐成为治疗青少年脊柱侧凸的主流技术,被多数脊柱外科医生所采用。相对于传统的钩棒系统及钩钉棒混合系统,全椎弓根螺钉系统有更好的三平面矫正效果,同时具有融合节段少,术后矫正率丢失低,长期随访翻修率低等优势[1-5]。此外,随着椎弓根钉技术发展,单纯后路手术就可以完成矫正,减少了前路松解的手术操作,并且通过矫正胸廓畸形能有效的改善肺功能[8,9]。虽然椎弓根螺钉技术具有上述的优点,但仍有不少学者对于该技术的使用存在质疑。Liljenqvist UR等[10]通过回顾性研究发现椎弓根螺钉技术对于侧凸矫正效果略好于钩棒技术,但统计学上无明显差异。椎弓根螺钉在椎弓根及椎体皮质上的穿出率为25%,但无明显神经损伤症状出现。其他学者也报道了椎弓根螺钉固定后出现的神经并发症,发生率为0.26%~17%[6,7]。有学者报道椎弓根螺钉技术对于侧凸患者矢状面上的矫正效果不佳[11]。Kim YJ等[12]和Vora V等[13]发现采用椎弓根螺钉治疗的脊柱侧凸患者出现胸椎后凸减少。Quan GM等[14]发现椎弓根螺钉治疗侧凸,冠状面上矫正效果越好,矢状面上矫正效果越差。
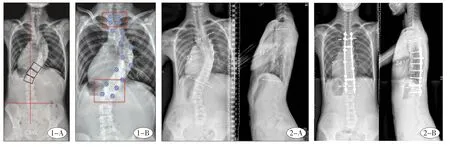
图1 A,术前脊柱全长正位片;B:术前手术设计,远近固定两个节段建立框架结构,中间节段凹侧和凸侧交叉间隔置钉。图2 A,患者女性,13岁,特发性脊柱侧弯,A:术前脊柱全长正侧位片,冠状面上主胸弯Cobb角为52°,矢状面上T5~T12角度为11°。B:术后脊柱全长正侧位片,冠状面上主胸弯Cobb角矫正为5°,矢状面上T5 T12角度矫正为24°。Fig.1 A,Preoperative spinal anterior-posterior radiograph;B,Preoperative plan:two levels at upper and lower ends of fusion block were fixed bilaterally,pedicle screwswere placed at intervals on both concave and convex sides at themiddle level. Fig.2 A,3-year-old female patientwith idiopathic scoliosis.A:Preoperative spinal radiograph,coronalmain thoracic Cobb anglewas52 degrees and sagittalalignment11 degrees from T5-T1.B:Immediate postoperative spinal radiograph illustratedmain thoracic curve correction of 5 degrees on coronal plane and T5-T12 angle correction of 24 degrees on sagittal plane.
虽然椎弓根螺钉技术已成熟运用于青少年脊柱侧凸的治疗,但对于置钉位置的选择及置钉的数量仍存在争议[15-17]。全椎弓根螺钉技术已被很多脊柱外科医生所采用,但是否每个螺钉都是必要的尚没有定论。脊柱侧凸的患者椎体发生旋转变形,使得椎弓根螺钉置入的难度和危险性显著增加,螺钉置入数量的增加必然会使神经血管损伤风险增高[18,19]。同时螺钉置入数量的增加,会使手术费用显著提高。由于目前国内植入物基本是自费,因此需要我们在治疗中努力寻找既能保证治疗质量,又能相对控制治疗费用的方法。全椎弓螺钉技术,术中螺钉使用数量为“融合节段×2”,而交叉置钉技术的螺钉数量是“融合节段+4”,两种方法比较,后者可以减少螺钉数量为“融合节段-4”。如果设计10个节段融合,可节省至少6枚螺钉,这对于减少治疗费用的意义是显而易见的。Bharucha NJ等[16]发现置钉的密度与术后临床、放射结果及并发症的发生无明显关系,但置钉密度低组的手术费用明显降低。有诸多研究比较了钩棒系统及椎弓根钉系统对于侧凸的矫正效果,发现钩棒系统的平均矫正率为49%~52%,而椎弓根系统的平均矫正率为56%~71%[4,20-23]。本研究发现主弯矫正率为70.5%,无一例患者出现神经血管并发症,末次随访时矫正率无明显丢失且固定节段完全融合。由此可见,本研究所采用的后路交叉置钉技术获得了满意的治疗效果,同时有效降低了置钉数量。
青少年脊柱侧凸的三平面矫正中很重要的一点是对椎体旋转的矫正,通过对椎体旋转的矫正可提高冠状面侧凸矫正率,改善肺部功能及外观畸形[24,25]。本研究采用交叉置钉技术,在有效较少置钉数量的基础上,保证矫正节段每个椎体上至少置入一枚椎弓根螺钉,使得矫正过程中能很好的控制每个椎体的旋转。同时术中我们对于椎体变形严重的节段采用导航辅助置钉技术,降低神经血管损伤风险的同时,提高置钉的准确性增加其把持力。后路交叉置钉取得良好的矫正效果应该是基于脊柱侧凸患者还存在较好的柔韧度的基础上,对于僵硬性的脊柱侧凸其矫正效果可能会低于预期,其治疗效果有待于进一步比较研究。
本研究的不足之处在于随访时间还较短,平均随访时间才2年。同时由于本研究采用全椎弓根螺钉治疗的患者病例数较少,无法进行有效的自身对比研究。但初步结果显示对于青少年脊柱侧凸后路手术矫正,采用交叉置钉技术是一项值得推广的低费用、高安全的脊柱侧凸矫正技术。
1 Crawford AH1,Lykissas MG,Gao X,et al.All-pedicle screw versus hybrid instrumentation in adolescent idiopathic scoliosis surgery:a comparative radiographical study with aminimum 2—Year follow-up[J].Spine(Phila Pa 1976),2013,38(14):1199—1208.DOI:10.1097/BRS.0b013e31828ce597.
2 Yilmaz G,Borkhuu B,Dhawale AA,et al.Comparative analysis of hook,hybrid,and pedicle screw instrumentation in the posterior treatment of adolescent idiopathic scoliosis[J].J Pediatr Orthop,2012,32(5):490—499.DOI:10.1097/BPO.0b013e318250c629.
3 Wu X,Yang S,Xu W,et al.Comparative intermediate and long-term results of pedicle screw and hook instrumentation in posterior correction and fusion of idiopathic thoracic scoliosis[J].J Spinal Disord Tech,2010,23(7):467—473. DOI:10.1097/BSD.0b013e3181bf6797.
4 Kim YJ,Lenke LG,Kim J,et al.Comparative analysis of pedicle screw versus hybrid instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis[J].Spine(Phila Pa 1976),2006,31(3):291—298.DOI:10.1097/01. brs.0000197865.20803.d4.
5 Cheng I,Kim Y,Gupta MC,et al.Apical sublaminar wires versus pedicle screws-which provides better results for surgical correction of adolescent idiopathic scoliosis?[J].Spine(Phila Pa 1976),2005,30(18):2104—2112.
6 Diab M,Smith AR,Kuklo TR.Neural complications in the surgical treatment of adolescent idiopathic scoliosis[J]. Spine(Phila Pa 1976),2007,32(24):2759—63 1976),2007,32(24):2759—2763.DOI:10.1097/RS.0b013e318 15a5970.
7 Di Silvestre M,Parisini P,et al.Complications of thoracic pedicle screws in scoliosis treatment[J].Spine(Phila Pa 1976),2007,32(15):1655—1661.DOI:10.1097/BRS. 0b013e318074d604.
8 Kim YJ,Lenke LG,Bridwell KH,et al.Prospective pulmonary function comparison following posterior segmental spinal instrumentation and fusion of adolescent idiopathic scoliosis:is there a relationship between major thoracic curve correction and pulmonary function test improvement?[J].Spine(Phila Pa 1976),2007,32(24):2685—2693.DOI:10. 1097/BRS.0b013e31815a7b17.
9 Luhmann SJ,Lenke LG,Kim YJ,et al.Thoracic adolescent idiopathic scoliosis curves between 70 degrees and 100 degrees:is anterior release necessary?[J].Spine(Phila Pa 1976),2005,30(18):2061—2067.
10 Liljenqvist UR,Halm HF,Link TM.Pedicle screw instrumentation of the thoracic spine in idiopathic scoliosis[J]. Spine(Phila Pa 1976),1997,22(19):2239—2245.
11 Liu T,Hai Y.Sagittal plane analysis of selective posterior thoracic spinal fusion in adolescent idiopathic scoliosis:a comparison study ofall pedicle screw and hybrid instrumentation[J].JSpinal Disord,Tech,2014,27(5):277—282. DOI:10.1097/01.bsd.0000451597.91287.a0.
12 Kim YJ,Lenke LG,Cho SK,et al.Comparative analysis of pedicle screw versus hook instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis[J].Spine(Phila Pa 1976),2004,29(18):2040—2048.
13 Vora V,Crawford A,Babekhir N,et al.A pedicle screw construct gives an enhanced posterior correction of adolescent idiopathic scoliosis when compared with other constructs:myth or reality[J].Spine(Phila Pa 1976),2007,32(17):1869—1874.DOI:10.1097/BRS. 0b013e318108b912.
14 Quan GM,Gibson MJ.Correction of main thoracic adolescent idiopathic scoliosis using pedicle screw instrumentation:does higher implant density improve correction?[J]. Spine(Phila Pa 1976),2010,35(5):562—567.DOI:10. 1097/BRS.0b013e3181b4af34.
15 Li J,Cheung KM,Samartzis D,et al.Key-vertebral Screws Strategy for Main Thoracic Curve Correction in Patientswith Adolescent Idiopathic Scoliosis[J].Clin Spine Surg,2016,29(8):E434—441.DOI:10.1097/BSD. 0000000000000129.
16 Bharucha NJ,Lonner BS,Auerbach JD,et al.,Low-density versus high-density thoracic pedicle screw constructs in adolescent idiopathic scoliosis:domore screws lead to a better outcome?[J].Spine J,2013,13(4):375—381.DOI:10.1016/j.spinee.2012.05.029.
17 Tsirikos AI,Subramanian AS.Posterior spinal arthrodesis for adolescent idiopathic scoliosis using pedicle screw instrumentation:does a bilateral or unilateral screw technique affect surgical outcome?[J].JBone Joint Surg Br,2012,94(12):1670—1677.DOI:10.1302/0301—620X.94B12. 29403.
18 Belmont PJJr,KlemmeWR,Dhawan A,etal.In vivo accuracy of thoracic pedicle screws[J].Spine(Phila Pa 1976),2001,26(21):2340—2346.
19 Kothe R,O'Holleran JD,Liu W,et al.Internal architecture of the thoracic pedicle.An anatomic study[J].Spine(Phila Pa 1976),1996,21(3):264—270.
20 Liljenqvist U,Lepsien U,Hackenberg L,et al.Comparative analysis of pedicle screw and hook instrumentation in posterior correction and fusion of idiopathic thoracic scoliosis[J].Eur Spine J,2002,11(4):336—343.DOI:10.1007/s00586—002—0415—9.
21 Dobbs MB,Lenke LG,Kim YJ,et al.Selective posterior thoracic fusions for adolescent idiopathic scoliosis:comparison of hooks versus pedicle screws[J].Spine(Phila Pa 1976),2006,31(20):2400—2404.DOI:10.1097/01.brs. 0000240212.31241.8e.
22 Kuklo TR,Potter BK,Lenke LG,et al.
Surgical revision rates of hooks versus hybrid versus screws versus combined anteroposterior spinal fusion for adolescent idiopathic scoliosis[J].Spine(Phila Pa 1976),2007,32(20):2258—2264.DOI:10.1097/BRS.0b013e31814b1ba6.
23 Suk SI,Lee SM,Chung ER,et al.Selective thoracic fusion with segmental pedicle screw fixation in the treatmentof thoracic idiopathic scoliosis:more than 5-year follow—up[J]. Spine(Phila Pa 1976),2005,30(14):1602—1609.
24 Lee SM,Suk SI,Chung ER.Direct vertebral rotation:a new technique of three-dimensional deformity correction with segmental pedicle screw fixation in adolescent idiopathic scoliosis[J].Spine(Phila Pa 1976),2004,29(3):343—349.
25 Vallespir GP,Flores JB,Trigueros IS,etal.Vertebral copla
nar alignment:a standardized technique for three dimensional correction in scoliosis surgery:technical description and preliminary results in Lenke type 1 curves[J].Spine(Phila Pa 1976),2008,33(14):1588—1597.DOI:10. 1097/BRS.0b013e3181788704.
Application of bilateral interval pedicle screw ing for adolescent scoliosis patients.
Zhang Yan,Chen Bochang,Bao Kun.Department of Orthopedics,Sixth People′s Hospital,Shanghai Jiaotong University,Shanghai 200233,China.Corresponding author:Chen Bochang,Email:orthopedicchen@126.com
ObjectiveTo explore the clinical efficacy of bilateral interval pedicle screw placement for adolescent scoliosis.Methods A total of68 patients(10 boys and 58 girls)with adolescent scoliosis underwent posterior fusion using bilateral interval pedicle screw placement.Theirmean agewas13.5 years.The preoperative angles of thoracic coronal and sagittal Cobb were 56°and 17°.The variables ofmain sagittal and coronal Cobb angles at the immediate postoperative and the last follow-up,curve correction rate weremeasured and the clinical outcomes analyzed.Results Themean follow-up period was22.5months.And themean immediate postoperative and last follow-upmain thoracic coronal Cobb anglewere 18.5°and 20.2°.No statistically significant differences existed between preoperative and immediate postoperative(P<0.01),but not between immediate postoperative and last follow-up(P>0.05).Themean thoracic sagittal Cobb angle improved from 17.7°preoperatively to 22.8°immediate postoperatively.However,the change had no significant difference(P>0.05).Themean immediate curve correction rate of 70.5%differed not from that of the last follow-up(P>0.05).At the last follow-up,bone fusion was achieved in all patients.No instrumentation-related complications were noted.Conclusion Bilateral interval pedicle screwing is safe and efficacious for adolescent scoliosis.
Adolescent;Scoliosis;Surgical Procedures,Operative;Follow-Up Study
2015—08—25,修回期:2017—03—21)
(本文编辑:仇 君)
10.3969/j.issn.1671—635 3.2017.04.012.
10.3969/j.issn.1671-6353.2017.04.012
上海交通大学附属第六人民医院(上海市,200433)
陈博昌,Email:orthopedicchen@126.com
本文引用格式:张彦,陈博昌,鲍琨.后路交叉置钉技术在青少年脊柱侧凸治疗中的应用[J].临床小儿外科杂志,2017,16(4):364—367.
Citing this article as:Zhang Y,Chen BC,Bao K.Bilateral interval pedicle screw technigue for the surgical treatment of the adolescent scoliosis patients[J].JClin Ped Sur,2017,16(4):364—367.DOI:10.3969/j.issn.1671—635 3.2017. 04.012.
猜你喜欢
中国港湾建设(2022年12期)2022-12-28
中国典型病例大全(2022年9期)2022-04-19
儿童故事画报(2017年7期)2017-07-19
中国生物医学工程学报(2017年6期)2017-02-10
中华骨与关节外科杂志(2016年6期)2016-05-17
中华骨与关节外科杂志(2016年5期)2016-05-17
中国当代医药(2015年31期)2015-03-01
中国继续医学教育(2015年8期)2015-01-31
四川党的建设(2014年10期)2015-01-26
中国中医药现代远程教育(2014年20期)2014-03-01
