
Er,Cr:YSGG激光联合粘结剂封闭牙本质小管的封闭效果
2017-06-29 04:26:47张羽朱立江王香兰
海南医学 2017年11期
张羽,朱立江,王香兰
(1.潍坊医学院口腔医学院,山东潍坊261053;2.青岛市口腔医院多学科综合门诊,山东青岛266001)
Er,Cr:YSGG激光联合粘结剂封闭牙本质小管的封闭效果
张羽1,朱立江2,王香兰2
(1.潍坊医学院口腔医学院,山东潍坊261053;2.青岛市口腔医院多学科综合门诊,山东青岛266001)
目的通过扫描电镜观察,定量评估并比较自酸蚀粘结剂、Er,Cr:YSGG激光及其联合应用对牙本质小管的封闭效果。方法将40颗人新鲜拔除的第三磨牙制备成1.5 mm厚的牙本质片,用35%磷酸处理10 s,采用简单随机分组法将标本随机分为四组:A组为空白对照组,不做任何处理;B组和C组为自酸蚀粘结剂组和Er,Cr:YSGG激光组,分别用Clearfil S3 Bond自酸蚀粘结剂和Er,Cr:YSGG激光进行表面处理;D组为Er,Cr:YSGG激光联合粘结剂组,先用Er,Cr:YSGG激光进行表面照射,后用自酸蚀粘结剂进行表面处理,扫描电镜下观察各组牙本质表面及纵剖面的超微结构。结果(1)表面结构:A组牙本质小管口全部开放,清晰无玷污层;B组牙本质小管口表面覆盖大量晶体状结晶物,牙本质小管口明显缩窄;C组牙本质小管口表面呈凹凸不平的熔融状,牙本质小管口不规则地向管中心缩窄;D基本看不到牙本质小管口,牙本质表面覆盖有一层均匀的细结晶物。(2)纵剖面结构:A组牙本质小管呈条索状平行排列,小管内光滑无堵塞物;B组牙本质小管内可见长条状的致密树脂突堵塞物;C组牙本质小管内堵塞物进入牙本质小管深度较浅;D组牙本质小管内可见白色细条索状堵塞物,外部为一层均匀致密物质。(3)组间牙本质小管直径和面积比较,空白对照组>粘结剂组>激光组>联合组,组间牙本质小管堵塞率比较,联合组>激光组>粘结剂组,差异均有统计学意义(P˂0.05)。结论自酸蚀粘结剂,Er,Cr:YSGG激光,以及两者联合应用均能有效封闭牙本质小管,且联合组优于单独应用。
牙本质小管;Er,Cr:YSGG激光;自酸蚀粘结剂;扫描电镜
牙本质过敏症(dentinal hypersensitivity,DH)是指暴露的牙本质小管受到口腔环境的刺激如机械、温度、化学、渗透压等,以短暂、剧烈、尖锐的疼痛或不适,为主要临床特点的一种临床症状[1]。
药物脱敏剂作为传统的治疗牙本质敏感的方法,仍被广泛应用,研究表明药物脱敏剂对缓解牙本质敏感有显著效果,但远期效果不佳[2-3]。近年来激光由于其迅速、有效、安全等特点,被广泛应用到临床治疗中。Nd:YAG激光对牙本质小管的封闭作用优于其他激光[4-5],因而成为临床最常用的缓和牙本质敏感症状的激光。但由于Nd:YAG激光的热效应,具有较强的渗透性,容易使牙本质表面产生微裂,损伤骨组织及牙髓组织,其临床应用具有一定的局限性。Er,Cr:YSGG激光(又名水激光)因其不会损伤牙髓组织被用于牙本质敏感症的脱敏治疗,并取得了较好的效果。
目前对Er,Cr:YSGG激光的研究大部分停留在其与传统脱敏剂或传统激光的比较上,或对其不同功率及模式上的比较分析,且基本为描述性定性分析,尚未有学者对Er,Cr:YSGG激光与Clearfil S3 Bond联合应用效果与其单独应用效果做出比较。本实验通过定量测量扫描电镜下Er,Cr:YSGG激光与Clearfil S3 Bond联合应用及其单独使用下牙本质小管口的开放情况,比较并评估其对牙本质小管的封闭作用,为临床选择治疗牙本质敏感症的方法提供依据。
1 材料与方法
1.1 标本选择选取2016年3~4月在青岛市口腔医院新鲜拔除的人第三磨牙40颗,患者年龄20~30岁,牙齿形态完整,无龋坏、无隐裂,未做过根管治疗。本实验所用牙齿符合伦理学标准,且已取得患者同意。
1.2 材料实验所用试剂及设备见表1。

表1 实验试剂及设备表
1.3 实验方法
1.3.1 标本处理将新鲜拔除的离体牙去除牙石、牙周膜及牙周组织,置于等渗生理盐水中,4℃冰箱备用。制备牙本质盘标本,自牙尖下1~2.5 mm用涡轮机垂直于牙体长轴制备成1.5 mm厚的牙本质片,蒸馏水冲洗干净,用35%磷酸处理牙本质盘10s,高压水枪冲洗30S,置于等渗生理盐水中,4℃冰箱中备用。
1.3.2 实验分组与处理将40个标本依次编号,采用简单随机分组法将40个标本随机分配分成四组,每组10个。A组为空白对照组,不做任何处理;B组为自酸蚀粘结剂(Clearfil S3 Bond)组,用小毛刷蘸取粘结剂在干燥的牙本质表面同向均匀涂30 s,气枪吹干,光固化20 s。C组为Er,Cr:YSGG激光组,选取蓝宝石工作头,所有操作步骤均与牙面呈90°,距牙本质盘表面1 mm处均匀式扫描,操作分三步,首先在功率0.1 W,空气量为1,水量1条件下照射20 s;然后在功率0.25 W,空气量为1,水量1条件下照射20 s;最后在功率0.25 W,空气量为0,无水条件下照射20 s。D组为Er,Cr:YSGG激光联合粘结剂组,先按照C组步骤进行水激光处理,然后进行B组步骤涂粘结剂。每组随机选取一个标本用持针器将标本正中钳开,断面不做任何处理。
1.3.3 扫描电镜观察将标本用2.5%戊二醛4℃下固定2 h,乙醇梯度脱水,真空干燥,镀金,在扫描电镜2 000倍下观察四组的横断面的牙本质小管封闭情况,在扫描电镜3 000倍及1 000倍下观察纵断面的超微结构。选取清晰的2 000倍下横断面图像,导入Image-ProPlus 6.0图像分析系统,系统根据颜色变化自动识别牙本质小管边界,根据标尺计算出牙本质小管开放区域的面积S及牙本质小管平均直径D。空白组开放区域牙本质小管面积计为S1,计算各实验组的牙本质小管堵塞率=(1-S/S1)×100%。
1.4 统计学方法按上述公式计算出各实验组牙本质小管堵塞率,用SPSS19.0软件对四组牙本质小管开放区域面积S,牙本质小管平均直径D以及三个实验组的牙本质小管堵塞率进行统计学分析,多组间采用单因素方差分析(ANOVA),LSD-t检验进行两两比较,检验标准α=0.05。
2 结果
2.1 各组牙本质小管表面的扫描电镜观察空白对照组,牙本质小管口全部开放,清晰无玷污层(图1A);Clearfil S3 Bond自酸蚀粘结剂组,牙本质小管口表面覆盖大量晶体状结晶物,牙本质小管口明显缩窄,部分牙本质小管口被完全封闭(图1B);Er,Cr:YSGG激光组牙本质小管口表面呈凹凸不平的熔融状,牙本质小管口不规则地向管中心缩窄,大小不均匀,部分牙本质小管口被完全封闭(图1C);联合组基本看不到牙本质小管口,牙本质表面覆盖有一层均匀的细结晶物,可看到个别不清晰的牙本质小管口影像(图1D)。

图1 各组牙本质小管表面的扫描电镜观察(×2 000)注:A为空白对照组;B为Clearfil S3 Bond自酸蚀粘结剂组;C为Er,Cr:YSGG激光组;D为联合组。
2.2 各组牙本质纵剖面的扫描电镜观察空白对照组牙本质小管呈条索状平行排列,小管内光滑无堵塞物;Clearfil S3 Bond自酸蚀粘结剂组,牙本质小管内可见长条状的致密树脂突堵塞物,进入牙本质小管深度约为58 μm;Er,Cr:YSGG激光组牙本质小管内堵塞物进入牙本质小管深度较浅,约为16 μm,部分牙本质小管表面有不规则熔融状结构,可能为熔融的牙本质形成;联合组牙本质小管内可见白色细条索状堵塞物,进入小管深度约60 μm,外部为一层约30.6 μm的均匀致密物质,有可能为激光照射后粗糙的牙体表面与粘结剂的混合产物,见图2和图3。

图2 各组牙本质纵剖面的扫描电镜观察(×3 000)注:箭头所示为牙本质小管内堵塞物;A为空白对照组;B为Clearfil S3 Bond自酸蚀粘结剂组;C为Er,Cr:YSGG激光组;D为联合组。
2.3 横断面开放牙本质小管直径、开放牙本质小管口面积及牙本质小管堵塞率的统计分析表2为各组开放牙本质小管直径、开放牙本质小管口面积及牙本质小管堵塞率的均值和标准差及其比较,四组差异均具有统计学意义(P˂0.01),表明粘结剂组、激光组、联合组均能有效封闭牙本质小管;各组间两两比较,差异有统计学意义(P˂0.05),认为各组在封闭牙本质小管作用上存在差异。扫描电镜2 000倍下开放牙本质小管直径空白对照组>粘结剂组>激光组>联合组,开放牙本质小管口面积空白对照组>粘结剂组>激光组>联合组,牙本质小管堵塞率联合组>水激光组>粘结剂组。
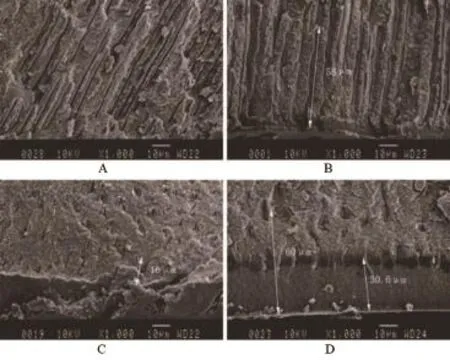
图3 各组牙本质纵剖面的扫描电镜观察(×1 000)注:A为空白对照组;B为Clearfil S3 Bond自酸蚀粘结剂组;C为Er,Cr:YSGG激光组;D为联合组。

表2 各组开放牙本质小管直径开放牙本质小管口面积及牙本质小管堵塞率比较(x-±s)
3 讨论
West NX的研究表明28%的牙本质敏感患者感到其严重或极其严重地影响到了其正常生活[6]。牙本质敏感症的临床表现复杂,发病机制至今尚未完全明确,液体流动学说目前被广泛接受[7]。研究表明,扫描电镜下牙本质敏感患牙的牙本质小管数目为不敏感牙本质小管数的8倍,且直径要比不敏感牙本质小管大[8],刺激因素可以通过开放暴露的牙本质小管刺激牙本质小管液流动传递给牙髓感觉中枢,产生疼痛,所以有效地封闭牙本质小管,抑制牙本质小管内液体流动,是治疗牙本质敏感症的有效方法。
Er,Cr:YSGG激光利用流体动力学原理将水、气、激光同时输出,其波长为2 780 nm,接近水的吸收峰值,牙本质中的主要成分为羟基磷灰石,羟基磷灰石及水分子吸收激光能量并作用于组织上产生微爆裂,从而有效切割牙体软硬组织,同时喷射出的水会对牙体组织及软组织产生降温作用,阻止激光的热效应。Er,Cr:YSGG激光的组织渗透力比较低,为14~20 μm,不会损伤牙髓及牙周组织[9]。Gholami等[4]的研究表明Er,Cr:YSGG,Nd:YAG,CO2激光对牙本质小管的封闭作用均较好,且Er,Cr:YSGG和Nd:YAG激光的封闭效果相差不大。但Nd:YAG激光的作用单一,不能切割软硬组织,经济度低,这为Er,Cr:YSGG激光代替Nd:YAG激光对过敏牙齿进行更安全的脱敏提供了理论支持。
Er,Cr:YSGG激光的高能量模式可以用于切割牙体硬组织,低能量模式可以用来切割牙体软组织。研究表明,过高能量的Er,Cr:YSGG激光照射会使牙本质产生熔融碳化现象[10-11],所以本实验选用低能量的Er, Cr:YSGG激光在有水和无水情况下反复照射牙本质小管表面,是防止过高的能量产生碳化、微裂现象,损伤牙体,既保证了Er,Cr:YSGG激光对牙本质小管的封闭作用,又保证了组织安全性。
研究表明,Er,Cr:YSGG激光能有效地缓解牙本质敏感症[12-14]。Er,Cr:YSGG激光组牙本质表面产生了粗糙的结晶层,且管间牙本质呈熔融状态向开放的牙本质小管口突出,与研究报道的激光照射后的牙本质小管口表面形态相似[4,11],其细微差异可能与激光选择的模式不同有关。其表面个别部分有碳化、微裂现象,个别部分小管封闭效果不佳,个别部位照射过度或不足,这可能与水激光照射的手法不均匀有关,要求操作者拥有更加熟练的操作手法。
近年来许多对激光联合药物脱敏的研究都取得了较好的效果[16-17]。联合组的扫描电镜2 000倍表面结构呈光滑的细结晶状,基本看不到牙本质小管口,偶可见被堵塞的环形牙本质小管口,基本与Yilmaz等[14]研究的NaF+CO2激光组表面结构相一致。其对每100 μm2开放牙本质小管直径及数量的比较发现单独激光组与联合组并没有显著差异但都优于单独氟化钠组。Hossain等[15]将33.9 J/cm2,空气含量70%,水含量20%的Er,Cr:YSGG激光照射6 s与37%磷酸酸蚀30 s后的牙釉质及牙本质表面的粗糙程度进行扫描电镜观察,Er,Cr:YSGG组的粗糙度为150~170 μm,明显优于酸蚀组的73~94 μm。本实验联合组牙本质表面覆盖一层约30.6 μm的均匀致密物质,有可能为激光照射后粗糙的牙体表面与粘结剂的混合产物,可以改善因咀嚼磨耗等原因导致的单独应用粘结剂或激光造成的远期效果不佳的不足。且粘结剂产生的树脂突可以顺着激光照射后开放的牙本质小管进入牙本质深层,弥补了Er,Cr:YSGG激光封闭牙本质小管深度不足的缺点。
虽然扫描电镜观察下各实验组脱敏治疗后的牙本质小管口形态、牙本质小管内封闭物封闭形式、牙本质表面沉积物的成分都不尽相同,但各实验组均有较好的封闭效果。但本实验未对牙本质小管封闭的远期效果进行实验,缺乏临床观察研究,有待进一步研究。
综上所述,扫描电镜下观察Er,Cr:YSGG激光与Clearfil S3 Bond自酸蚀粘结剂的单独及联合应用均能有效封闭牙本质小管,联合组优于Er,Cr:YSGG激光组,优于自酸蚀粘结剂组。
[1]Cartwright RB.Dentinal hypersensitivity:a narrative review[J]. Community Dent Health,2014,31(1):15-20.
[2]Patil SA,Naik BD,Suma R.Evaluation of three different agents for in-office treatment of dentinal hypersensitivity:a controlled clinical study[J].Indian J Dent Res,2015,26(1):38-42.
[3]Yu X,Liang B,Jin X,et al.Comparative in vivo study on the desensitizing efficacy of dentin desensitizers and one-bottle self-etching adhesives[J].Oper Dent 2010,35(3):279-286.
[4]Gholami GA,Fekrazad R,Esmaiel-Nejad A.An evaluation of the occluding effects of Er;Cr:YSGG,Nd:YAG,CO2and diode lasers on dentinal tubules:a scanning electron microscope in vitro study[J]. Photomed Laser Surg,2011,29(2):115-121.
[5]Dilsiz A,Aydin T,Canakci V,et al.Clinical evaluation of Er:YAG, Nd:YAG,and diode laser therapy for desensitization of teeth with gingival recession[J].Photomed Laser Surg,2010,28 Suppl 2:S11-S17.
[6]West NX,Sanz M,Lussi A,et al.Prevalence of dentine hypersensitivity and study of associated factors:a European population-based cross-sectional study[J].J Dent,2013,41(10):841-851.
[7]Närhi M,Jyväsjärvi E,Virtanen A,et al.Role of intradental A-and C-type nerve fibres in dental pain mechanisms[J].Proc Finn Dent Soc,1992,88 Suppl 1:507-516.
[8]Cummins D.Recent advances in dentin hypersensitivity:clinically proven treatments for instant and lasting sensitivity relief[J].Am J Dent,2010,23 Spec NoA:3A-13A.
[9]Hossain M,Nakamura Y,Yamada Y,et al.Compositional and structural changes of human dentin following caries removal by Er,Cr:YSGG laser irradiation in primary teeth[J].J Clin Pediatr Dent, 2002,26(4):377-382.
[10]Aranha AC,Eduardo Cde P.In vitro effects of Er,Cr:YSGG laser on dentine hypersensitivity.Dentine permeability and scanning electron microscopy analysis[J].Lasers Med Sci,2012,27(4):827-834.
[11]Yilmaz HG,Bayindir H.Clinical and scanning electron microscopy evaluation of the Er,Cr:YSGG laser therapy for treating dentine hypersensitivity:short-term,randomised,controlled study[J].J Oral Rehabil,2014,41(5):392-398.
[12]Adu-Arko AY,Sidhu SK,McCabe JF,et al.Effect of an Er,Cr:YSGG laser on water perfusion in human dentine[J].Eur J Oral Sci, 2010,118(5):483-488.
[13]Al-Omari WM,Palamara JE.Effect of Er,Cr:YSGG laser on human dentin fluid flow[J].Lasers Med Sci,2013,28(6):1445-1451.
[14]Yilmaz HG,Cengiz E,Kurtulmus-Yilmaz S,et al.Effectiveness of Er,Cr:YSGG laser on dentine hypersensitivity:a controlled clinical trial[J].J Clin Periodontol,2011,38(4):341-346.
[15]Hossain M,Nakamura Y,Yamada Y,et al.Analysis of surface roughness of enamel and dentin after Er,Cr:YSGG laser irradiation[J].J Clin Laser Med Surg,2001,19(6):297-303.
[16]钱付民,韦丽峰.Er,Cr:YSGG激光联合Gluma脱敏剂治疗牙本质过敏的疗效观察[J].河南科技大学学报(医学版),2016,34(1):38-41.
[17]Cakar G,Kuru B,Ipci SD,et al.Effect of Er:YAG and CO2 lasers with and without sodium fluoride gel on dentinal tubules:a scanning electron microscope examination[J].Photomed Laser Surg,2008,26 (6):565-571.
Occluding effects of the combined application of Er,Cr:YSGG laser and adhesive on dentinal tubules:an in vitro study.
ZHANG Yu1,ZHU Li-jiang2,WANG Xiang-lan2.
1.School of Stomatology,Weifang Medical University,Weifang 261053,Shandong,CHINA;2.Department of Multidisciplinary Consultation Clinic,Qingdao Stomatological Hospital, Qingdao 266001,Shandong,CHINA
ObjectiveTo quantitatively evaluate and compare the sealing effects of self-etching adhesive,Er,Cr:YSGG laser and the combined application on dentin tubules by scanning electron microscope (SEM).MethodsForty fresh extracting human third molar samples were made into dentin specimens of 1.5 mm thickness that were treated with 35%phosphoric acid for 10 seconds.The specimens were randomly divided into four groups by simple random distribution method.Group A served as the control group without any further treatment;group B was treated with Clearfil S3 Bond self-etching adhesive alone;groups C were irradiated with Er,Cr:YSGG laser; groups D were treated with Er,Cr:YSGG laser plus Clearfil S3 Bond self-etching adhesive.The surface was irradiated and subjected to surface treatment with a self-etching binder.The utrastructure of dentin surface and vertical section in different groups was observed by SEM.Results(1)Surface observation:In group A,all of the dentinal tubules were numerous exposed without smear layer.In group B,the dentin tubules orifices were covered with irregular crystalline substance and the aperture of dentin tubule significantly narrowed.In group C,dentin tubule surface had a melted appearance and the dentin tubule orifices irregularly narrowed to the pipe center.In group D,dentin tubule orifices can hardly be seen and the surface structure primarily showed a smooth crystalline substance appearance.(2)vertical section observation:In group A,the dentin tubules were arranged in parallel without blockage.In group B,the tubules were covered with long strips of dense resin clogs.In group C,the tubules were covered with blockages not deep as group B.In group D,the dentin tubules were covered with white thin dense funicular clogs,and outside is a layer of uniform density material.(3)In terms of diameters and areas of open dentinal tubules,there was significant difference between groups,group A>group B>group C>group D(P˂0.05).In terms of plugging rate of open dentinal tubules,group D>group C>group B (P˂0.05).ConclusionAll self-etching adhesive,Er,Cr:YSGG laser and the combined application can occlude the tubules effectively,and moreover,the combined application has an advantage over Er,Cr:YSGG laser,while the Er,Cr:YSGG laser is superior to self-etching adhesive.
Dentin tubules;Er,Cr:YSGG laser;Self-etching adhesive;Scanning electron microscope(SEM)
R781.2
A
1003—6350(2017)11—1728—04
2016-12-19)
10.3969/j.issn.1003-6350.2017.11.003
王香兰。E-mail:yuzhimeng123@126.com
猜你喜欢
建筑材料学报(2023年10期)2023-11-17 04:58:40
化工设备与管道(2022年2期)2022-08-02 07:24:12
长江大学学报(自科版)(2021年2期)2021-05-19 01:04:40
石油钻采工艺(2021年5期)2021-04-25 14:34:14
化工管理(2021年10期)2021-04-25 13:55:00
石油钻探技术(2020年5期)2020-12-03 07:29:28
世界最新医学信息文摘(2020年5期)2020-02-14 09:36:08
实用临床医学(2019年3期)2019-07-30 07:28:32
科技资讯(2019年3期)2019-04-25 06:23:42
中国继续医学教育(2016年11期)2016-06-08 06:15:36
