氩氦刀冷冻消融术治疗中晚期原发性肝癌患者的血小板计数变化规律研究
2017-06-19 19:25邓梨平程瑞文李秋国
中国全科医学 2017年18期
邓梨平,程瑞文,李秋国,李 平
·论著·
氩氦刀冷冻消融术治疗中晚期原发性肝癌患者的血小板计数变化规律研究
邓梨平*,程瑞文,李秋国,李 平
目的 探讨氩氦刀冷冻消融术治疗中晚期原发性肝癌患者的血小板计数变化规律。方法 选取2013年7月—2016年6月湖南中医药大学第一附属医院收治的中晚期原发性肝癌患者60例,均行氩氦刀冷冻消融术(术前血小板计数≥50×109/L)治疗,冷冻针布针1~3根者为A组,4~10根者为B组,11~15根者为C组。总结A组、B组、C组术前、术后血小板计数变化规律。结果 A组术前和术后3、7、14 d的血小板计数比较,差异无统计学意义(P>0.05);B组、C组术前和术后3、7、14 d的血小板计数比较,差异有统计学意义(P<0.05);B组、C组术后3 d与术前血小板计数比较,差异有统计学意义(P<0.01)。由于A组术前和术后血小板计数变化不明显,故仅对B组、C组患者按术前血小板计数再次分组,术前血小板计数≥50×109/L且<100×109/L定义为观察组,血小板计数≥100×109/L定义为对照组。对照组和观察组术前和术后3、7、14 d的血小板计数组内比较,差异有统计学意义(P<0.05);对照组、观察组术后3 d与术前血小板计数比较,差异有统计学意义(P<0.01)。结论 氩氦刀冷冻消融术治疗中晚期原发性肝癌,血小板计数≥50×109/L、冷冻针≤3根时血小板计数没有明显变化,4~15根时血小板计数表现为术后3 d下降到氩氦刀冷冻消融术前的50%左右,而术后7 d回升至术前水平,术后14 d保持稳定。
肝肿瘤;冷冻外科手术;血小板
邓梨平,程瑞文,李秋国,等.氩氦刀冷冻消融术治疗中晚期原发性肝癌患者的血小板计数变化规律研究[J].中国全科医学,2017,20(18):2223-2226.[www.chinagp.net]
DENG L P,CHENG R W,LI Q G,et al.Platelet count change rule in medium-advanced primary hepatic carcinoma treated by argon-helium cryosurgery[J].Chinese General Practice,2017,20(18):2223-2226.
我国大部分原发性肝癌患者发生于肝硬化背景下,部分患者合并脾功能亢进,确诊时多为中晚期,这些因素导致原发性肝癌的疗效欠佳。近年来研究显示,氩氦刀冷冻消融术治疗中晚期原发性肝癌的疗效较为理想[1-3],最常见的并发症是血小板计数减少[4],但很少有氩氦刀冷冻消融术后血小板计数的研究,更罕见对血小板计数变化规律的研究报道。本研究旨在探讨氩氦刀冷冻消融术治疗中晚期原发性肝癌患者的血小板计数变化规律,现报道如下。
1 资料与方法
1.1 一般资料 选取2013年7月—2016年6月湖南中医药大学第一附属医院收治的中晚期原发性肝癌患者60例,其中男50例,女10例;年龄33~76岁,平均年龄(47.0±10.7)岁;均有乙肝、肝硬化病史。
1.2 诊断标准 患者均符合我国原卫生部制定的《原发性肝癌诊疗规范(2011版)》中的相关诊断标准[5]。氩氦刀冷冻消融术条件[1-4]:(1)凝血常规中活化部分凝血活酶时间(APTT)、凝血酶原时间(PT)延长至参考范围下限2倍以内,纤维蛋白原(FIB)正常,国际标准化比值(INR)1.5以内;(2)肝功能按照Child-Pugh改良分级法评定为Child A级或者Child B级[6];(3)卧位肝脏被膜外无腹腔积液;(4)白细胞计数≥3.0×105/L,血小板计数≥50×109/L;(5)近3个月无消化道大出血和外科手术史。
1.3 氩氦刀冷冻消融术方法 患者先行CT平扫+增强扫描以及MRI平扫+增强扫描,有强化的肿瘤病灶定义为肿瘤活性病灶[5],测量肿瘤活性病灶最大直径,制定氩氦刀冷冻消融术前的冷冻针布针方案,布针原则:(1)冷冻针穿刺通道避开肋骨、椎骨、胃肠道和胆囊。(2)冷冻针穿刺通道避开重要神经走行区域。(3)冷冻针穿刺通道避开门静脉和肝静脉1、2级属支。(4)肿瘤活性病灶最大直径2.0 cm内,布针≤3根;肿瘤最大直径≥2.0 cm,按照间隔1.0~1.5 cm布针且单次累计布针≤15根。然后在CT引导下按照以上布针方案逐点布好冷冻针,CT扫描验证布针结果与术前计划方案吻合,再启动以色列Galil Medical Cryohit 冷冻系统给予氩气冷冻消融15 min(压力3 500 psi),CT扫描检测冷冻范围,冰球覆盖活性肿瘤病灶区域边缘以达到减瘤灭
本文创新点:
(1)本研究对中晚期原发性肝癌的氩氦刀冷冻消融术治疗过程中血小板计数动态变化进行研究。(2)对氩氦刀冷冻消融术按照冷冻针多寡进行分组研究。(3)对氩氦刀冷冻消融术按照术前血小板计数进行分组研究。(4)总结冷冻针4~15根时患者血小板计数变化规律。(5)提出血小板计数变化除与消耗有关外可能存在其他机制。
活活性肿瘤的目的[7],氦气复温3 min(压力2 500 psi),再次重复一次冷冻和复温过程,并再次CT扫描检测冷冻范围,拔针,压迫止血并腹带加压包扎3 d,同时卧床休息。氩气为广州佛山华特公司生产,氦气为美国林得公司生产,纯度均为99.99%。1.4 分组标准 氩氦刀冷冻消融术后根据术中布针结果分组:布针1~3根者为A组(115例),布针4~10根者为B组(36例),布针11~15根者为C组(9例)。1.5 观察指标 观察氩氦刀冷冻消融术不同冷冻针数量组在术前和术后3、7、14 d血小板计数。

2 结果
2.1 氩氦刀冷冻消融术布针情况 60例患者3个月内无死亡病例,氩氦刀冷冻消融术布针情况详见表1。
2.2A、B、C组术前、术后血小板计数比较A组术前和术后3、7、14d的血小板计数比较,差异无统计学意义(P>0.05);B组、C组术前和术后3、7、14d的血小板计数组内比较,差异有统计学意义(P<0.05);B组、C组术后3d与术前血小板计数比较,差异有统计学意义(P<0.01,见表2)。由于A组术前和术后血小板计数变化不显著,故仅对B组、C组患者按术前血小板计数再次分组,术前血小板计数≥50×109/L且<100×109/L定义为观察组,血小板计数≥100×109/L定义为对照组。
2.3 对照组和观察组术前、术后血小板计数比较 对照组和观察组术前和术后3、7、14d的血小板计数组内比较,差异有统计学意义(P<0.05);其中对照组、观察组术后3d与术前的血小板计数比较,差异有统计学意义(P<0.01,见表3)。
表1 氩氦刀冷冻消融术布针情况
Table1StatusofcryoneedlesusedingroupsA,BandCinargon-heliumcryosurgery
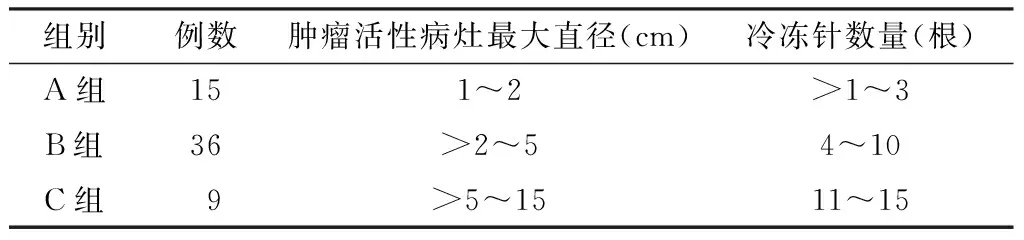
组别例数肿瘤活性病灶最大直径(cm)冷冻针数量(根)A组151~2>1~3B组36>2~54~10C组 9 >5~1511~15

Table2PlateletcountchangeingroupsA,BandCduringtheperioperativeperiodofargon-heliumcryoablation

时间点A组(n=15)B组(n=36)C组(n=9)术前100.2±45.180.9±31.272.4±21.8术后3d95.6±34.640.1±27.9a35.8±12.6a术后7d98.4±42.377.9±30.671.2±20.8术后14d99.7±42.678.2±32.673.5±20.1F值0.021.844.11P值>0.05<0.05<0.05
注:与术前比较,aP<0.01

Table3Plateletcountchangeinthecontrolandobservationgroupsduringtheperioperativeperiodofargon-heliumcryoablation

时间点对照组(n=24)观察组(n=21)术前120.7±16.875.2±23.5术后3d65.8±19.7a38.1±27.9a术后7d118.6±14.372.9±20.6术后14d119.8±20.274.5±18.5F值9.832.77P值<0.05<0.05
注:与术前比较,aP<0.01
3 讨论
3.1 氩氦刀冷冻消融术治疗中晚期原发性肝癌的现状 近年来有较多对氩氦刀冷冻消融术的研究报道[8-10],不断印证了氩氦刀冷冻消融术治疗中晚期原发性肝癌的确切疗效[11-14],其最常见的并发症是血小板计数减少,甚至发生出血[15],所以均强调氩氦刀冷冻消融术前血小板计数不低于100×109/L,但由于我国大部分原发性肝癌患者发生于肝硬化背景下,部分患者合并脾功能亢进,血小板计数常低于100×109/L,导致该技术使用受限[5]。王珏琼[6]总结肝硬化患者肝功能在Child A级和Child B级血小板计数分别为(70.36±15.67)×109/L和(61.35±11.62)×109/L,故本研究将血小板计数定义为≥50×109/L入组来研究,以期扩大治疗适应证,使更多患者受益。目前国内未查询到对血小板计数低于100×109/L患者进行研究的文献,也未查询到有关血小板计数变化规律的研究报道。
3.2 血小板计数的变化 本研究结果提示布针3根及以内的氩氦刀冷冻消融术后14 d内血小板计数变化不明显,提示3根及以内冷冻针形成冰球范围内的微血栓所消耗的血小板很快被机体代偿,在血小板计数变化层面上是安全的。B组、C组(布针4~15根)氩氦刀冷冻消融术后3 d血小板计数显著降低,分析与冷冻针数量增加时冰球范围增大,形成微血栓增多,消耗血小板增加有关,理论上随着冷冻针数量的增加消耗血小板数量相应增加,因而理论上也应该随着冷冻针数量的增加术后血小板计数减少率相应增加,但是结果B组、C组术后3 d血小板计数减少率均约为术前的50%,而术后7 d快速恢复,回升并稳定到术前水平。提示血小板计数的变化与冷冻针(4~15根)数量的多少无明显相关性。冷冻针的多寡在一定程度上与肿瘤的大小直接相关,故也提示氩氦刀冷冻消融术后血小板计数的变化在一定程度上与肿瘤的大小无明显相关性,布针4~15根的血小板计数不同分组提示,每组氩氦刀冷冻消融术后3 d与术前血小板计数变化比较均有显著下降,血小板计数减少率均约为术前的50%,而术后7 d快速恢复,回升并稳定到术前水平,提示氩氦刀冷冻消融术后血小板计数的变化规律与术前(≥50×109/L)具体数值无明显相关性,这些均提示氩氦刀冷冻消融术导致血小板计数减少除微血栓形成消耗血小板的这一机制外可能存在其他机制,有待进一步研究证实。
综上所述,氩氦刀冷冻消融术治疗中晚期原发性肝癌,血小板计数≥50×109/L时,冷冻针数量≤3根血小板计数没有明显变化,4~15根血小板计数表现为术后3 d下降到氩氦刀冷冻消融术前的50%左右,而术后7 d回升并稳定到术前水平,值得进一步研究。
作者贡献:邓梨平进行试验设计、资料收集整理、撰写论文并对文章负责;邓梨平、程瑞文、李秋国进行试验实施、评估;李平进行质量控制及审校。
本文无利益冲突。
本文的不足之处:
(1)本研究属小样本研究,且仅对血小板计数进行统计分析,未对血小板功能进行检测和统计分析。(2)使用的以色列Galil Medical Cryohit 冷冻系统,与美国冷冻系统未做对比分析。(3)本文是回顾性研究而非前瞻性对照研究。
[1]叶伟东,纪建松,涂建飞,等.氩氦刀冷冻消融联合肝动脉栓塞化疗术治疗中晚期肝癌的疗效分析[J].介入放射学杂志,2015,24(5):392-395.DOI:10.3969/j.issn.1008-794X.2015.05.007. YE W D,JI J S,TU J F,et al.Argon-helium cryoablation combined with transcatheter arterial chemoembolization for the treatment of advanced hepatocellular carcinoma:analysis of therapeutic effectiveness[J].Journal of Interventional Radiology,2015,24(5):392-395.DOI:10.3969/j.issn.1008-794X.2015.05.007.
[2]庄炜钊,黄晨,姬智艳,等.TACE 联合氩氦刀冷冻消融治疗中晚期肝癌的疗效分析[J].医学影像学杂志,2016,26(12):2247-2250. ZHUANG W Z,HUANG C,JI Z Y,et al.Analysis of therapeutic effetiveness of argon-helium cryoablation combined with transcatheter arterial chemoembolization for the treatment of advanced hepatocellular carcinoma[J].Journal of Medical Imaging,2016,26(12):2247-2250.
[3]邱国钦,许丽贞,罗鹏飞,等.氩氦刀冷冻消融联合TACE治疗巨大肝癌的临床观察[J].临床肿瘤学杂志,2015,20(6):540-544. QIU G Q,XU L Z,LUO P F,et al.Clinical observation of argon-helium knife cryotherapy combined with transcatheter arterial chemoemboli-zation (TACE) on huge liver cancer[J].Chinese Clinical Oncology,2015,20(6):540-544.
[4]程瑞文,邓梨平,李平,等.TACE联合氩氦刀冷冻消融术治疗原发性肝癌后血小板观察[J].中国中西医结合影像学杂志,2016,14(2):206-208.DOI:10.3969/j.issn.1672-0512.2016.02.028. CHENG R W,DENG L P,LI P,et al.Observation of platelet changes after TACE combined with argon-helium cryoablation in treatment of primary liver cance[J].Chinese Imaging Journal of Integrated Traditional and Western Medicine,2016,14(2):206-208.DOI:10.3969/j.issn.1672-0512.2016.02.028.
[5]中华人民共和国卫生部.原发性肝癌诊疗规范(2011版)[J].临床肿瘤学杂志,2011,16(10):929-946.DOI:10.3969/j.issn.1009-0460.2011.10.017. Ministry of Public Health in China.Diagnosis and treatment of primary liver cancer (2011 edition)[J].Chinese Clinical Oncology,2011,16(10):929-946.DOI:10.3969/j.issn.1009-0460.2011.10.017.
[6]王珏琼.血小板、凝血指标与老年肝硬化患者Child-Pugh分级的关系[J].中国老年学杂志,2013,33(24):6103-6105.DOI:10.3969/j.issn.1005-9202.2013.24.015. WANG J Q.The relationship between platelet,coagulation index and Child-Pugh grading in elderly patients with liver cirrhosis[J].Chinese Journal of Gerontology,2013,33(24):6103-6105.DOI:10.3969/j.issn.1005-9202.2013.24.015.
[7]张积仁,Gregory Graves.氩氦刀靶向肿瘤治疗技术[M].美国加州大学:先锋生物科学出版社,2002,38. ZHANG J R,GRAVES G.Cryocare targeted cryoablation therapy[M].University of California:Pioneer Bioscience Publishing,2002,38.
[8]郑泽华.肝动脉化疗栓塞联合氩氦刀冷冻消融治疗中晚期肝癌患者的疗效观察[J].现代诊断与治疗,2015,26(20):4728-4729. ZHENG Z H.Clinical observation of transcatheter arterial chemoembolization combined with argon helium cryoablation in the treatment of patients with advanced hepatocellular carcinoma[J].Modern Diagnosis and Treatment,2015,26(20):4728-4729.
[9]沈立杰.射频消融、氩氦刀冷冻对原发性肝癌治疗效果的对比分析[J].医学影像学杂志,2015,25(7):1216-1220. SHEN L J.Comparative analysis of treatment effect of primary hepatic carcinoma (PHC) by applying Ar-He Cryablation and radiofre-quency radiation[J].Journal of Medical Imaging,2015,25(7):1216-1220.
[10]陈习波,宋华志,何远春,等.氩氦刀冷冻消融联合肝动脉插管化疗栓塞治疗原发性肝癌的疗效研究[J].实用癌症杂志,2015,30(11):1710-1712.DOI:10.3969/j.issn.1001-5930.2015.11.038. CHEN X B,SONG H Z,HE Y C,et al.Efficacy of argon-helium cryoablation combined with transcatheter arterial chemoembolization in the treatment of primary hepatic cancer[J].The Practical Journal of Cancer,2015,30(11):1710-1712.DOI:10.3969/j.issn.1001-5930.2015.11.038.
[11]刘秋华,周革阶,张伯,等.TACE联合氩氦刀冷冻治疗原发性肝癌临床分析[J].肝胆胰外科杂志,2014,26(4):278-280. LIU Q H,ZHOU G J,ZHANG B,et al.Clinical analysis of primary hepatic carcinoma treated by TACE combined with cryoablation[J].Journal of Hepatopancreatobiliary Surgery,2014,26(4):278-280.
[12]侯晓玮,宋谦,李露嘉,等.TACE 联合氩氦冷冻消融治疗原发性肝癌效果观察[J].实用医药杂志,2013, 30(4):293-295.DOI:10.3969/j.issn.1671-4008.2013.04.003. HOU X W,SONG Q,LI L J,et al.The efficacy of primary hepatic carcinoma treated by TACE combined with argon-helium cryoablation[J].Practical Journal of Medicine & Pharmacy,2013,30(4):293-295.DOI:10.3969/j.issn.1671-4008.2013.04.003.
[13]徐稳深,吴阳,严双喜.肝癌冷冻消融治疗的临床应用分析[J].包头医学院学报,2016,32(5):16-17. XU W S,WU Y,YAN S X.Analysis of the clinical application of cryoablation for liver cancer[J].Journal of Baotou Medical College,2016,32(5):16-17.
[14]王成虎,徐高峰,吉洪海,等.氩氦刀冷冻联合肝动脉化疗栓塞治疗原发性肝癌的对照研究[J].齐齐哈尔医学院学报,2015,36(33):5043-5045. WANG C H,XU G F,JI H H,et al.Control study on argon-helium cryotherapy combine hepatic arterial chemoembolization of primary liver cancer[J].Journal of Qiqihar University of Medicine,2015,36(33):5043-5045.
[15]易峰涛,卢绮萍,吴坤.氩氦刀治疗实验性肝肿瘤并发出血的原因研究[J].中国临床研究,2016,29(2):166-168.DOI:10.13429/j.cnki.cjcr.2016.02.006. YI F T,LU Q P,WU K.Reasons of hemorrhage after argon-helium cryoablation in rabbits with experimental liver tumor[J].Chinese Journal of Clinical Research,2016,29(2):166-168.DOI:10.13429/j.cnki.cjcr.2016.02.006.
(本文编辑:崔莎)
Platelet Count Change Rule in Medium-advanced Primary Hepatic Carcinoma Treated by Argon-helium Cryosurgery
DENGLi-ping*,CHENGRui-wen,LIQiu-guo,LIPing
VascularandOncologyInterventionalDepartment,theFirstHospitalofHunanUniversityofChineseMedicine,Changsha410007,China
Objective To explore the platelet count change rule of medium-advanced primary hepatic carcinoma treated by argon-helium cryosurgery.Methods Sixty cases with medium-advanced primary hepatic carcinoma admitted in the First Hospital of Hunan University of Chinese Medicine from July 2013 to June 2016 were selected as the participants.All of them had preoperative platelet count equal to or greater than 50×109/L,and
argon-helium cryosurgery.Based on the number of cryoneedles used in the surgery,they were divided into group A(using 1-3 cryoneedles),group B(using 4-10 cryoneedles),group C(using 11-15 cryoneedles ).The postoperative platelet count change rules in groups A,B and C were summarized.Results Platelet count measured before the surgery,at 3,7,14 d after the surgery differed significantly in groups B and C(P<0.05),but not in group A(P>0.05).Platelet count measured before the surgery was obviously different from that measured at 3 d after the surgery in both groups B and C(P<0.01).As the change of platelet count was obvious in groups B and C,so we further studied the change of it in them.Patients with platelet count level lower than 100×109/L but equal to or greater than 50×109/L and those with it equal to or greater than 100×109/L in group B and group C were assigned to the observation group and control group,respectively.Platelet count measured before the surgery,at 3,7,14 d after the surgery differed significantly in both the observation group and control group (P<0.05).Significant differences were found between the platelet count measured before the surgery and that measured at 3 d after the surgery in both the observation group and control group (P<0.01).Conclusion During the perioperative period of argon-helium cryosurgery for medium-advanced primary hepatic carcinoma patients whose preoperative platelet count levels were equal to or greater than 50×109/L,platelet count did not change significantly in those used 1-3 cryoneedles,but in those used 4~15 cryoneedles,it dropped by almost half of the preoperative level at the 3rd day after surgery,then elevated to the preoperative level at the 7th day after surgery,and remained stable at the 14th day after surgery.
Liver neoplasms;Cryosurgery;Blood platelet
湖南省卫计委资助项目(C2016051)
R 735.7
A
10.3969/j.issn.1007-9572.2017.18.011
2016-09-08;
2017-02-28)
410007湖南省长沙市,湖南中医药大学第一附属医院血管肿瘤介入科
*通信作者:邓梨平,副主任医师;E-mail:13875788233@163.com
*Correspondingauthor:DENGLi-ping,Associatechiefphysician;E-mail:13875788233@163.com
猜你喜欢
中华实用诊断与治疗杂志(2022年1期)2022-08-31
中国典型病例大全(2022年12期)2022-05-13
数学小灵通(1-2年级)(2021年11期)2021-12-02
世界科学技术-中医药现代化(2021年12期)2021-04-19
世界科学技术-中医药现代化(2021年10期)2021-03-02
中华养生保健(2020年8期)2021-01-14
中等数学(2020年8期)2020-11-26
小学生学习指导(低年级)(2020年4期)2020-06-02
数学大王·低年级(2019年8期)2019-08-27
中国临床医学影像杂志(2019年4期)2019-06-18