急诊重症监护室患者与社区健康人群肠道假丝酵母构成的比较与分析
2017-03-02 03:17李贞章黎华董丹凤江岑彭奕冰
微生物与感染 2017年1期
李贞,章黎华,董丹凤,江岑, 彭奕冰
上海交通大学医学院附属瑞金医院检验科,上海 200025
·论著·
急诊重症监护室患者与社区健康人群肠道假丝酵母构成的比较与分析
李贞,章黎华,董丹凤,江岑, 彭奕冰
上海交通大学医学院附属瑞金医院检验科,上海 200025
本研究旨在分析社区正常人群与急诊重症监护室(intensive care unit,ICU)患者肠道假丝酵母(又称念珠菌)的组成,比较两组人群肠道念珠菌构成的差异。2014年5—7月,收集1 732名上海社区健康人群的粪便标本;2014年2月—2015年1月,收集191名上海交通大学医学院附属瑞金医院急诊ICU患者的粪便或肛周拭子标本。经真菌培养收集单个菌落,通过内转录间隔区(internal transcribed spacer,ITS)序列分析进一步鉴定菌种,分析两组人群肠道定植真菌的组成特点。结果显示,社区健康人群的肠道标本中检测到9种念珠菌,定植率为13.16%;同时有两种和三种念珠菌定植的比例分别为3.81%和0。急诊ICU患者肠道标本只检测到5种念珠菌,但定植率高达37.17%;同时有两种和三种念珠菌定植的比例分别为9.95%和2.09%。社区健康人群和急诊ICU患者肠道中常见念珠菌分别为白念珠菌(5.25%vs. 27.23%)、光滑念珠菌(5.83%vs. 13.61%)、热带念珠菌(0.52%vs. 7.33%)、近平滑念珠菌(4.16%vs. 2.09%)、Candidametapsilosis(1.10%vs. 1.05%)。结果显示,急诊ICU患者的肠道念珠菌定植率显著高于社区人群(P<0.001),同时有两种(P=0.001)和三种(P<0.001)念珠菌定植的比例也显著高于社区人群。这种肠道念珠菌的高度定植及多重定植可能增加急诊ICU患者发生念珠菌感染的概率。
真菌;假丝酵母;肠道菌群;健康人群;重症监护室
假丝酵母(又称念珠菌)是引发黏膜感染及侵袭性感染的重要致病菌[1]。近年来念珠菌菌血症在重症监护室(intensive care unit,ICU)的发病率逐年上升。但侵袭性念珠菌感染早期缺乏特异的症状和体征,且患者常伴有多种复杂的基础性疾病,因此早期诊断较困难,这给临床预防治疗侵袭性念珠菌感染带来了挑战。已有研究报道了一些监测侵袭性念珠菌感染发生的指标,其中念珠菌定植被认为是独立危险因素[2]。
念珠菌并不一定是致病菌,它是人体正常菌群的一部分,常定植在正常人的呼吸道、肠道及阴道。当机体免疫功能下降时,有可能引发疾病[3]。在ICU侵袭性念珠菌感染患者中,88.6%在感染前经历过较长时间的念珠菌定植[2]。
肠道菌群是引发机体微生物感染的来源之一。疾病状态下,肠黏膜上皮受损,菌群的生长环境发生变化,种群间的拮抗作用减弱,优势菌群会大量繁殖。另外,因机体免疫力下降,肠内菌更易向上或向体内移位,从而引起肺炎、肠源性感染和内毒素血症等[4]。有研究表明,定植在肠道的念珠菌是引发念珠菌菌血症的重要来源[5]。因此,了解肠道定植菌群的组成及分布有重要意义。
目前有关肠道菌群的研究多集中于细菌,肠道念珠菌的研究较少;加上近年来念珠菌菌血症的发病率逐年上升,尤其是ICU危重患者。为此,本研究分析了社区正常人群与急诊ICU患者肠道念珠菌的组成,比较两组人群肠道念珠菌构成的差异。
1 材料与方法
1.1 标本收集
于2014年5—7月收集上海社区健康人群的粪便标本,接种于科玛嘉显色平板,35 ℃培养48 h,根据菌落颜色,收集单个菌落于YPD-甘油培养液中-80 ℃冻存。社区健康人群为进行健康普查的人群,符合下列条件:①无腹泻;②近1个月未使用抗生素及抗真菌药物;③无其他明显的疾病症状。收集2014年2月—2015年1月进入上海交通大学医学院附属瑞金医院急诊ICU约1周的患者,无腹泻且未发生侵袭性念珠菌感染。取其粪便或肛周拭子标本,接种于科玛嘉显色平板培养,收集单个菌落于YPD-甘油培养液中-80 ℃冻存。
1.2 菌株鉴定
所收集的菌株经API板条(法国生物梅里埃公司)初步鉴定菌种,其后经内转录间隔区(internal transcribed spacer,ITS)测序进一步鉴定。即将冻存的菌株接种SDA平板复苏后,参照Redkar等[6]的方法提取DNA,保存于-20 ℃,采用聚合酶链反应(polymerase chain reaction,PCR)扩增ITS片段进一步鉴定菌种[7]。引物为ITS1:5′-TCCGTA-GGTGAACCTGCG-3′;ITS4:5′-TCCTCCGCTT-ATTGATATGC-3′。PCR反应体系50 μL,包括10×PCR缓冲液(无Mg2+)5 μL、25 mmol/L MgCl25 μL、2.5 mmol/L dNTP 4 μL、10 μmol/L引物各1 μL、TaqDNA聚合酶(5 U/μL)0.5 μL、DNA(100 ng/μL)1 μL、ddH2O 32.5 μL。扩增程序:94 ℃ 5 min,94 ℃ 30 s,50 ℃ 30 s,72 ℃ 30 s,共30个循环;72 ℃ 5 min。PCR扩增产物委托Invitrogen公司测序。
1.3 仪器与试剂
PCR扩增仪(PTC-100 Thermal Cycle)购自美国MJ Research公司,ITS分析所用引物由Invitrogen上海技术服务部合成,溶壁酶(lyticase)购自美国Sigma公司,PCR试剂盒购自日本TaKaRa公司,电泳成像系统为Tanon 4100成像系统。
1.4 数据分析
整理菌种鉴定后的结果,用SPSS 19.0分析软件比较社区人群与急诊ICU患者中各种念珠菌检出率的差异。连续性变量以mean±SD表示,用独立样本t检验比较;分类变量用百分比表示,用卡方检验比较。P<0.05为有显著性差异。
2 结果
2.1 社区健康人群肠道念珠菌的构成情况
本研究中共纳入社区人群1 732人,平均年龄(63.38±15.98)岁;男性占43.73%,女性占56.27%。其中13.16%的人群肠道中有念珠菌定植,多为一种念珠菌定植(9.30%),3.87%的人群同时有两种念珠菌定植(表1)。同时有两种念珠菌定植的社区人群中,多见白念珠菌+光滑念珠菌(35人)、白念珠菌+近平滑念珠菌(20人)、白念珠菌+Candidametapsilosis(4人)(表2)。在社区人群共检测到9种念珠菌,其中白念珠菌占5.25%、光滑念珠菌占5.83%、热带念珠菌占0.52%、近平滑念珠菌占4.16%、Candidametapsilosis占1.10%。
表1 社区人群与急诊ICU患者肠道念珠菌定植情况的比较
Tab.1 The intestinalCandidain healthy population and emergency ICU (EICU) patients
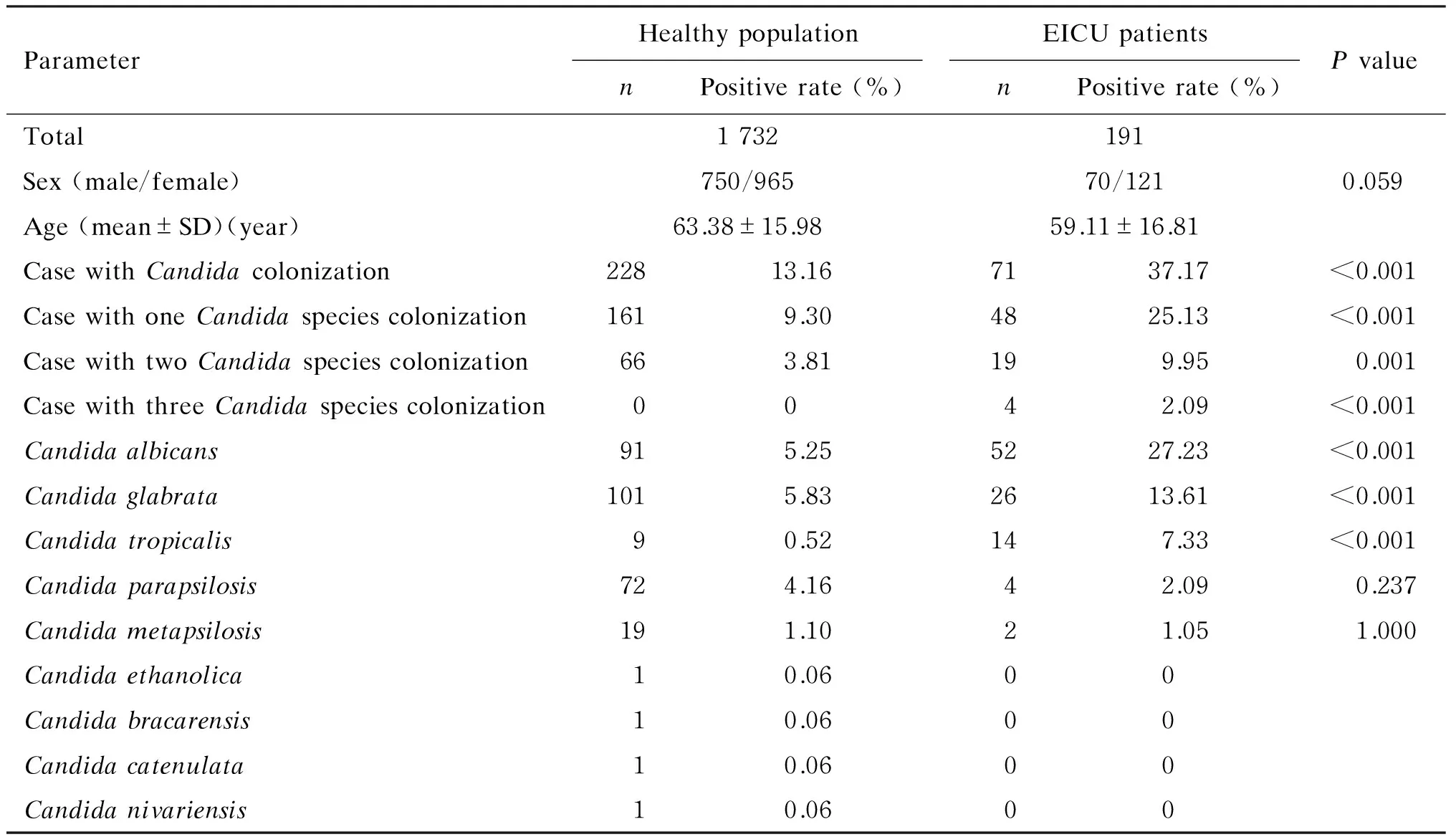
ParameterHealthypopulationnPositiverate(%)EICUpatientsnPositiverate(%)PvalueTotal1732191Sex(male/female)750/96570/1210.059Age(mean±SD)(year)63.38±15.9859.11±16.81CasewithCandidacolonization22813.167137.17<0.001CasewithoneCandidaspeciescolonization1619.304825.13<0.001CasewithtwoCandidaspeciescolonization663.81199.950.001CasewiththreeCandidaspeciescolonization0042.09<0.001Candidaalbicans915.255227.23<0.001Candidaglabrata1015.832613.61<0.001Candidatropicalis90.52147.33<0.001Candidaparapsilosis724.1642.090.237Candidametapsilosis191.1021.051.000Candidaethanolica10.0600Candidabracarensis10.0600Candidacatenulata10.0600Candidanivariensis10.0600
注:本研究中社区人群1 732人,其中17人未收集到性别信息。
表2 同时有两种念珠菌定植的情况
Tab.2 Cases with twoCandidaspecies colonization
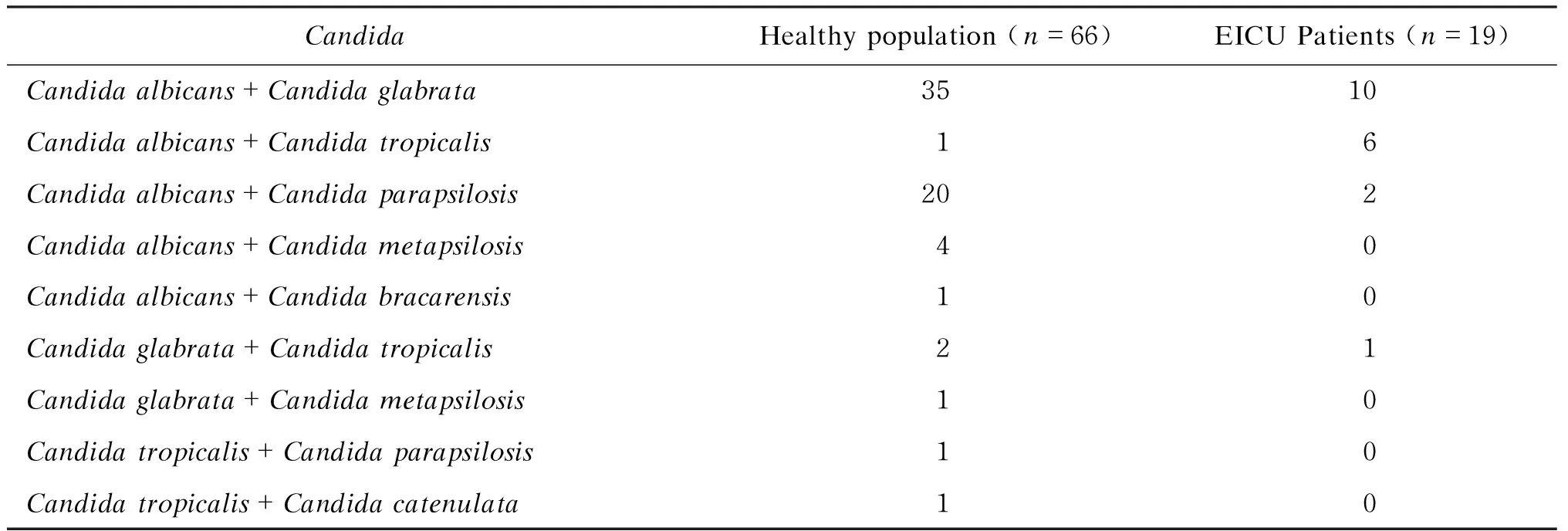
CandidaHealthypopulation(n=66)EICUPatients(n=19)Candidaalbicans+Candidaglabrata3510Candidaalbicans+Candidatropicalis16Candidaalbicans+Candidaparapsilosis202Candidaalbicans+Candidametapsilosis40Candidaalbicans+Candidabracarensis10Candidaglabrata+Candidatropicalis21Candidaglabrata+Candidametapsilosis10Candidatropicalis+Candidaparapsilosis10Candidatropicalis+Candidacatenulata10
2.2 急诊ICU患者肠道念珠菌的构成情况
急诊ICU患者191人,平均年龄(59.11±16.81)岁;男性占36.65%、女性占63.35%。社区人群与急诊ICU患者的性别、年龄构成无显著性差异。急诊ICU患者肠道念珠菌的检出率显著高于社区人群(37.17%vs. 13.16%,P<0.001),且同时有两种(9.95%vs. 3.81%,P=0.001)和三种(2.09%vs. 0,P<0.001)念珠菌定植的比例显著高于社区人群。同时有两种念珠菌定植的急诊ICU患者中,最多见白念珠菌+光滑念珠菌(10人)。在急诊ICU患者肠道中只检测到5种念珠菌,阳性率依次为白念珠菌(27.23%)、光滑念珠菌(13.16%)、热带念珠菌(7.33%)、近平滑念珠菌(2.09%)、Candidametapsilosis(1.05%);其中白色念珠菌、光滑念珠菌及热带念珠菌的阳性检出率显著高于社区人群。
3 讨论
人体肠道内寄居着种类繁多的微生物,正常情况下这些微生物对人体无害,称为正常菌群。正常菌群不仅与人体保持平衡状态,菌群之间也相互制约,维持相对平衡。在这种状态下,正常菌群发挥其营养、免疫和拮抗等生理作用。在某些情况下,如机体免疫力下降、使用广谱抗生素等,会使肠道菌群失调,进而引发疾病[4]。因此,了解肠道正常菌群的构成、生理作用及其失调与疾病的关系,对维护人体健康有重要意义。
念珠菌是引发血流感染的重要致病菌。真菌血症的发病率在丹麦约为8.6/10万[8],在美国一些城市达26.2/10万[9],而上海高达32/10万[10],严重威胁着患者的生命健康。引发真菌血症的致病菌中念珠菌属最常见(91.97%),其次是毕赤酵母(3.65%)。念珠菌属中最常见者为白念珠菌(35.03%),其次为近平滑念珠菌(18.25%)、热带念珠菌(13.87%)、光滑念珠菌(11.68%)[1]。肠道是引发念珠菌菌血症的重要来源之一[5]。本研究发现念珠菌的肠道定植率在社区健康人群为13.16%,在急诊ICU患者达37.17%。肠道定植的念珠菌属中,白念珠菌、光滑念珠菌、热带念珠菌、近平滑念珠菌较常见。虽然光滑念珠菌在肠道的定植率远高于近平滑念珠菌,但前者引发的血流感染率低于后者。这可能是因为,一方面光滑念珠菌比近平滑念珠菌毒力弱;另一方面近平滑念珠菌不在患者定植也能引发血流感染,主要是通过外源性途径,如医疗设施、医护人员的手、静脉插管等[11-12]。
本研究发现,急诊ICU患者肠道念珠菌的检出率显著高于社区人群(37.17%vs. 13.16%,P<0.001),同时有两种(9.95%vs. 3.81%,P=0.001)和三种(2.09%vs. 0,P<0.001)念珠菌定植的比例也显著高于社区人群,表明急诊ICU患者肠道内念珠菌的数量和种类更丰富。这可能与急诊ICU患者大多使用过广谱抗生素有关。应用广谱抗生素后,对抗生素敏感的细菌被抑制或杀灭,而对抗生素不敏感的细菌和真菌则有机会大量繁殖。
综上所述,社区健康人群肠道内有念珠菌定植,且种类丰富。与社区健康人群相比,急诊ICU患者肠道念珠菌检出率显著升高,同时有两种和三种念珠菌定植的比例也显著增高。这种肠道念珠菌的高度定植及多重定植一定程度上增加了急诊ICU患者发生念珠菌感染的概率。
Dong D, Li Z, Zhang L, Jiang C, Mao E, Wang X, Peng Y. Clinical and microbiological investigation of fungemia from four hospitals in China [J]. Mycopathologia, 2015, 179(5-6): 407-414.
[2] León C, Ruiz-Santana S, Saavedra P, Almirante B, Nolla-Salas J, Alvarez-Lerma F, Garnacho-Montero J, León MA; EPCAN Study Group. A bedside scoring system (“Candida score”) for early antifungal treatment in nonneutropenic critically ill patients with Candida colonization [J]. Crit Care Med, 2006, 34(3): 730-737.
[3] Schulze J, Sonnenborn U. Yeasts in the gut: from commensals to infectious agents [J]. Dtsch Arztebl Int, 2009, 106(51/52): 837-842.
[4] 祝司霞.肠道正常菌群与人体关系的分析 [J].医学信息(上旬刊),2010,23(11):4121-4122.
[5] Nucci M, Anaissie E. Revisiting the source of candidemia: skin or gut? [J]. Clin Infect Dis, 2001, 33(12): 1959-1967.
[6] Redkar RJ, Dubé MP, Mccleskey FK, Rinaldi MG, Del Vecchio VG. DNA fingerprinting of Candida rugosa via repetitive sequence-based PCR [J]. J Clin Microbiol, 1996, 34(7): 1677-1681.
[7] Tavanti A, Davidson AD, Gow NA, Maiden MC, Odds FC. Candida orthopsilosis and Candida metapsilosis spp. nov. to replace Candida parapsilosis groups II and III [J]. J Clin Microbiol, 2005, 43(1): 284-292.
[8] Arendrup MC, Bruun B, Christensen JJ, Fuursted K, Johansen HK, Kjaeldgaard P, Knudsen JD, Kristensen L, Møller J, Nielsen L, Rosenvinge FS, Røder B, Schønheyder HC, Thomsen MK, Truberg K. National surveillance of fungemia in Denmark (2004 to 2009) [J]. J Clin Microbiol, 2011, 49(1): 325-334.
[9] Cleveland AA, Farley MM, Harrison LH, Stein B, Hollick R, Lockhart SR, Magill SS, Derado G, Park BJ, Chiller TM. Changes in incidence and antifungal drug resistance in candidemia: results from population-based laboratory surveillance in Atlanta and Baltimore, 2008-2011 [J]. Clin Infect Dis, 2012, 55(10): 1352-1361.
[10] Yang ZT, Wu L, Liu XY, Zhou M, Li J, Wu JY, Cai Y, Mao EQ, Chen EZ, Lortholary O. Epidemiology, species distribution and outcome of nosocomial Candida spp. bloodstream infection in Shanghai [J/OL]. BMC Infect Dis, 2014. http://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-14-241.
[11] Trofa D, Gácser A, Nosanchuk JD. Candida parapsilosis, an emerging fungal pathogen [J]. Clin Microbiol Rev, 2008, 21(4): 606-625.
[12] da Silva Ruiz L, Montelli AC, Sugizaki Mde F, da Silva EG, de Batista GC, Moreira D, Paula CR. Outbreak of fungemia caused by Candida parapsilosis in a neonatal intensive care unit: molecular investigation through microsatellite analysis [J]. Rev Iberoam Micol, 2013, 30(2): 112-115.
. PENG Yibing, E-mail: pyb9861@sina.com
Analysis of the composition of intestinalCandidain emergency intensive care unit patients and community healthy population
LI Zhen,ZHANG Lihua,DONG Danfeng, JIANG Cen,PENG Yibing
DepartmentofClinicalLaboratory,RuijinHospital,ShanghaiJiaoTongUniversitySchoolofMedicine,Shanghai200025,China
The purpose of the present study is to investigate the composition of intestinalCandidain community healthy population and emergency intensive care unit (EICU) patients. The stool or rectal swab samples were collected from 1 732 community healthy people in Shanghai between May 2014 and July 2014, and from 191 EICU patients in Ruijin Hospital, Shanghai Jiao Tong University School of Medicine between February 2014 and January 2015. After fungal culture, individual colonies were collected and further identified by amplifying and sequencing of internal transcribed spacers (ITSs). The composition characteristics of intestinal fungi in the two groups were analyzed by statistical method. The results demonstrated that, in the intestinal tract of community healthy population, 9Candidaspecies were detected. TheCandidacolonization rate of community healthy population was 13.16%, and the colonization rates of two or threeCandidaspecies were 3.81% and 0, respectively. While in the intestinal tract of EICU patients, only 5Candidaspecies were cultured. TheCandidacolonization rate of EICU patients was 37.17%, and the colonization rates of two or threeCandidaspecies were 9.95% and 2.09%, respectively. The positive rates of common intestinalCandidain community healthy population and EICU patients wereCandidaalbicans(C.albicans) (5.25%vs. 27.23%),C.glabrata(5.83%vs. 13.61%),C.tropicalis(0.52%vs. 7.33%),C.parapsilosis(4.16%vs. 2.09%),C.metapsilosis(1.10%vs. 1.05%). It is concluded that the colonization rate of intestinalCandidain EICU patients is significantly higher than that in community healthy population (P<0.001). The colonization rates of two or threeCandidaspecies in EICU patients are also higher than those in community healthy population (P=0.001,P<0.001). EICU patients have a higher colonization rate of intestinalCandida, to a certain extent, could increase the probability ofCandidainfection.
Fungus;Candida; Intestinal flora; Healthy population; Intensive care unit
国家自然科学基金(81371873、81572053、81301462)
彭奕冰
2016-02-24)
猜你喜欢
中老年保健(2022年2期)2022-08-24
中国饲料(2022年5期)2022-04-26
浙江中西医结合杂志(2022年3期)2022-03-23
科学(2020年4期)2020-11-26
临床检验杂志(2020年1期)2020-03-02
现代检验医学杂志(2016年1期)2016-11-12
西南军医(2016年6期)2016-01-23
现代检验医学杂志(2015年4期)2015-02-06
现代检验医学杂志(2015年2期)2015-02-06
现代检验医学杂志(2015年2期)2015-02-06