上颌前牙倾斜角度对种植治疗设计的影响
2016-12-21 03:17:59刘金蒲必双夏玉兰王成泽王罡兰晶
华西口腔医学杂志 2016年6期
刘金 蒲必双 夏玉兰 王成泽 王罡 兰晶
1.山东大学口腔医院修复科;2.种植科,济南 250012
上颌前牙倾斜角度对种植治疗设计的影响
刘金1蒲必双2夏玉兰2王成泽2王罡2兰晶2
1.山东大学口腔医院修复科;2.种植科,济南 250012
目的 利用锥形束CT(CBCT)研究上颌前牙与牙槽骨的相对位置关系。方法 选取上颌恒牙牙列完整的患者150例(年龄19~48岁,男性和女性各75例),按性别和牙位分为6个组。以牙槽骨长轴为基准,在CBCT影像上测量上颌前牙牙体长轴的相对倾斜角度(偏向腭侧为正,偏向唇侧为负)。使用SPSS 19.0软件对数据进行统计分析。结果 所有研究对象的上颌前牙的牙体长轴均偏向牙槽骨长轴的腭侧。男性上颌中切牙、侧切牙、尖牙的牙体长轴与牙槽骨长轴所成角度α的平均值分别为16.22°(2.50°~28.80°)、17.50°(3.80°~29.50°)、16.27°(1.00°~31.50°),而女性的相应测量结果平均值分别为15.20°(2.20°~27.20°)、15.99°(4.10°~33.30°)、15.01°(3.50°~27.40°)。结论 上颌前牙与牙槽骨的倾斜方向不一致,所有上颌前牙牙体长轴均偏向于牙槽骨长轴腭侧。通过CBCT观察上颌前牙与牙槽骨的位置关系,可以指导种植时机,种植体植入位置以及骨增量方案的选择。
锥形束CT; 牙体长轴; 牙槽骨长轴; 美学区; 牙种植
牙齿并不是垂直地排列在牙槽骨中,而是具有一定的倾斜方向与倾斜角度[1-2]。《口腔解剖生理学》教材(第7版)认为,“上颌切牙均向唇侧倾斜,与颌骨前端牙槽突的倾斜方向一致”[3]。临床工作中笔者却发现实际情况并非完全如此,上颌前牙牙体长轴与牙槽骨长轴并不完全一致,而是存在着一定的角度。这种指导理论与实际情况之间的差异会明显影响临床医生在种植及修复治疗时的设计和效果。本研究利用非侵入性的锥形束CT(cone beam computed tomography,CBCT)技术,在正中矢状面上测量成年人上颌前牙与牙槽骨的位置关系,从而为美学区的种植治疗提供参考。
1 材料和方法
1.1 研究对象的选择
收集2012年12月—2013年12月在山东大学口腔医院就诊的山东地区成年患者的CBCT资料,筛选出上颌恒牙列完整的患者150例,其中男女各75例,年龄19~48岁,其中19~28岁、29~38岁、39~48岁男女各25例。对病例进行信息采集时,应符合以下纳入标准:1)除第三磨牙外上颌恒牙牙列完整;2)无明显牙列拥挤或明显的牙间隙,牙间隙小于等于2 mm;3)前牙正常萌出,牙根发育正常;4)前牙无龋坏或非龋性缺损,无任何形式的修复体、充填体;5)牙周组织健康、无明显牙槽骨吸收;6)无任何明显病理性因素,如根尖囊肿、牙根内外吸收、颌骨疾病等;7)无任何牙颌外伤史或正畸、正颌治疗史;8)CBCT影像清晰,无伪影。
1.2 测量方法
使用Galileos自带的SIDEXIS XG2.53软件打开所选取患者的CBCT图像,选取受测牙水平横断面(图1A,以左侧上颌中切牙为例),将横断面调整至受测牙颈部(图1B),再选取平分其近远中的平面作为矢状向平面(图1C),并调整角度使虚线通过牙体长轴(图1D)。该矢状向平面为受测牙的测量平面,即此受测牙的正中矢状面。
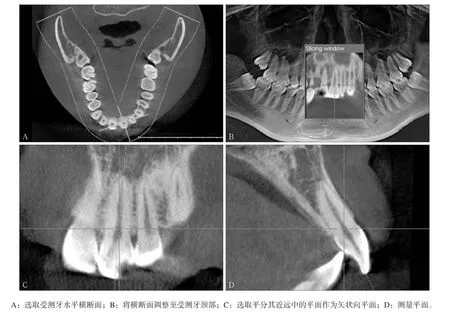
图1 上颌前牙测量平面的定位Fig 1 Orientating the measurement plane of maxillary anterior teeth
选取受测牙的正中矢状面,定点[4-10],如图2所示。A点:上颌前牙切缘中点;B点:上颌前牙根尖点;C点:上颌前牙唇侧牙槽嵴顶点;D点:上颌前牙腭侧牙槽嵴顶点;E点:位于上颌唇侧骨壁上,与上颌前牙根尖点的连线为最短距离的点;F点:位于上颌腭侧骨壁上,与上颌前牙根尖点的连线为最短距离的点;G点:C、D连线中点;H点:E、F连线中点。根据AB连线(牙体长轴)与GH连线(牙槽骨长轴)的角度关系确定α角:以牙槽骨长轴(GH连线)为基准,牙体长轴(AB连线)偏向唇/腭侧的角度即为α角,设定偏腭侧为正值,偏唇侧为负值。所有数据均由同一位测量者测得,每个测量项目测量3次,取平均值作为最终测量值,以确保数据的准确性。
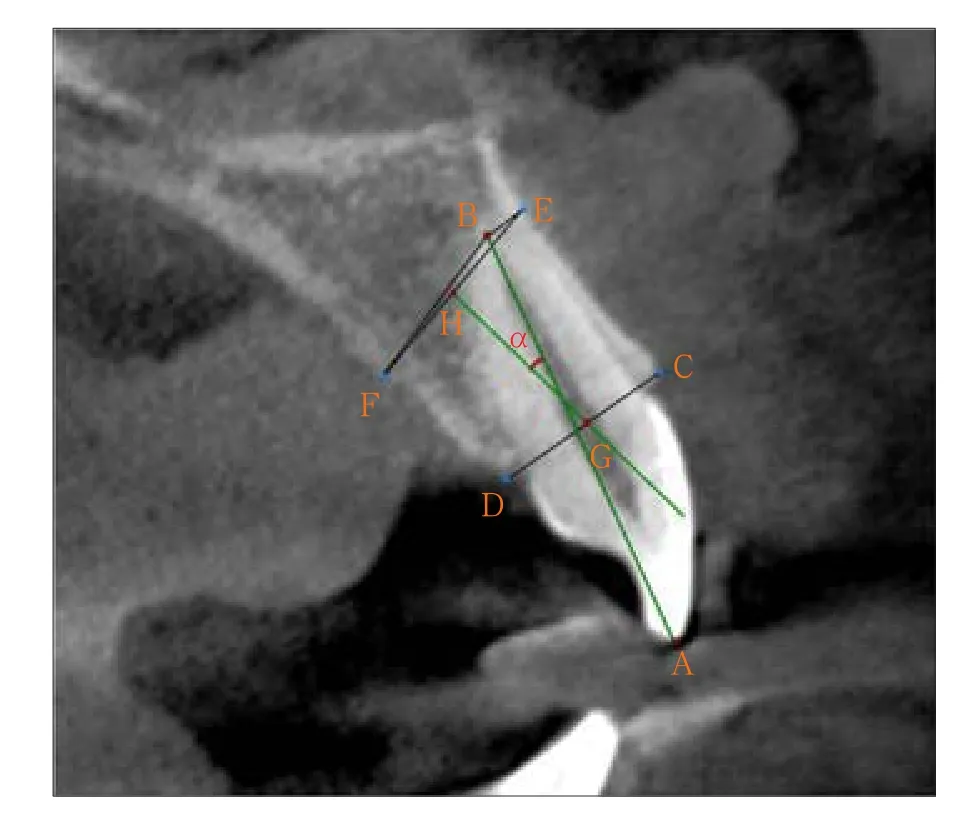
图2 上颌前牙定点及α角度的测量Fig 2 Location of landmark points and measurements of angle α
1.3 统计学分析
使用SPSS 19.0统计软件包进行统计分析。对不同性别、不同牙位测量所得数据(各75例)分别进行正态性检验,均符合正态性分布;再对相同性别同名牙位(例如女性左上中切牙和女性右上中切牙)进行t检验,检验水准为双侧α=0.05。由于相同性别同名牙位所得数据的差异无统计学意义,所以将相同性别同名牙位的数据合并(如女性上中切牙组),得出6个组,每组150颗牙齿,对合并所得的数据进行统计学描述。
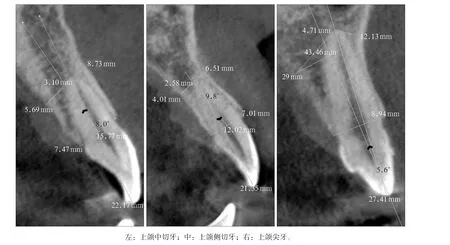
图3 第1类Fig 3 Type Ⅰ
2 结果
以牙槽骨长轴为基准,上颌前牙的牙体长轴偏向唇/腭侧的角度α测量结果见表1。由表1可以看出,所有上颌前牙的牙体长轴相对于牙槽骨长轴均偏向腭侧。
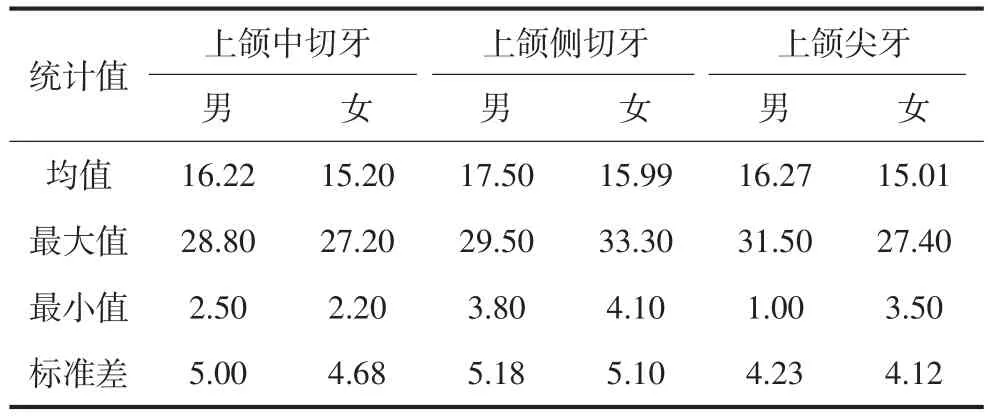
表1 上颌前牙牙体长轴相对于牙槽骨长轴偏向唇/腭侧角度α的测量值Tab 1 The internal angle α formed by the long axis of the maxillary anterior teeth and the long axis of the alveolar bone °, n=150
根据上颌前牙区α角度的频数分布,将α角度分为α<10°、10°≤α≤20°、α>20°共3个角度区间,分别记为第1类、第2类、第3类(如图3~5所示)。角α在3个角度区间的分布百分比见表2。
所有分组属于第1类的牙数均少于15%,其中男性上颌侧切牙组、男女性上颌尖牙组不足10%;上颌前牙区超过半数以上的受测牙都属于第2类,其中男女性上颌尖牙组属于此类的均占78.67%(118/150);女性上颌前牙区属于第3类的牙齿基本不足20%,其中侧切牙区比例最大,为20.67%(31/150),而男性上颌前牙属于第3类的比例在中切牙、侧切牙、尖牙组相差较大,分别为25.33%(38/150)、35.33%(53/ 150)、16.00%(24/150)。女性上颌侧切牙、男性上颌尖牙组测量结果的最大值均超过30°(表1)。
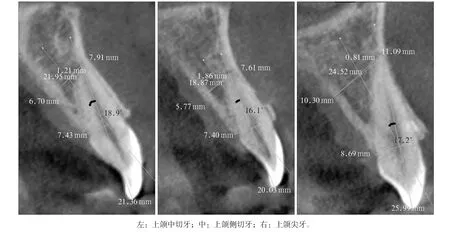
图4 第2类Fig 4 Type Ⅱ

图5 第3类Fig 5 Type Ⅲ

表2 上颌前牙牙体长轴相对于牙槽骨长轴偏向唇/腭侧的角度α分布百分比 Tab 2 Frequency distribution of angle α formed by the long axis of the maxillary anterior teeth and the long axis of the alveolar bone %
3 讨论
前牙区是美学的敏感区,在此区进行种植治疗极富挑战性。在种植义齿修复过程中,从术前设计到种植体的定位、植入、二期手术与修复过程中的设计和操作都会对种植义齿的美观产生直接或间接的影响[11]。
目前,种植术前设计已经可以预测最终修复后的美学、生物力学和功能恢复情况,即修复引领下的种植体植入(prosthetically driven implant placement),这一概念已经取代了以牙槽骨量决定种植体植入的概念[12-13]。在以修复为导向的前提下,如果种植体能够顺着牙槽窝的方向植入,那么最终的修复体仅需要一个常规直基台就可获得理想的三维形态。即刻种植和早期种植往往易于做到这一点,但是如何保证延期种植也能获得良好的美学效果,正是本研究所要探讨的问题。
上颌前牙长期缺失会导致牙槽嵴顶吸收及颌骨唇侧重度凹陷[14],常迫使种植体的植入角度或位置发生改变。由于种植体非轴向植入会造成种植体周围骨损失并对骨结合有阻碍作用,所以种植体长轴与修复后牙体长轴最大程度重合才是最有利的植入方向。虽然种植体过度倾斜可通过角度基台来调整,但会带来两个方面的问题:一方面,上颌前牙区的角度基台增加到25°时,种植体应力会增加18%[15],当种植体的应力增大到其所能承受的范围之外时必然会导致种植失败率增加;另一方面,种植体过度倾斜会影响最终的美观效果。因此基台的角度不是任意的,而应控制在一定范围内。由此可见,术前的正确定位十分重要,在进行延期种植治疗方案设计时,应参考对侧同名牙或邻牙,尽可能恢复牙槽骨原有骨量及形态,从而保证种植体良好的三维位置及轴向。
本研究中发现,上颌前牙牙体长轴与颌骨前端的牙槽突的倾斜方向并不一致,上颌前牙牙体长轴相对于牙槽骨长轴均偏向腭侧。本研究按照倾斜度数的大小将上颌前牙牙体与牙槽骨的关系分为3种类型。第1类(图3)因角度较小,可认为牙齿与牙槽骨倾斜方向基本一致,同时此类牙齿一般伴有较厚的唇侧骨壁,拔牙时唇侧骨板往往得以完整保留,进行种植治疗设计时可优先选择即刻或早期种植,应用不翻瓣或翻瓣技术顺着牙槽窝的方向略偏腭侧植入,种植体即能获得良好的初期稳定性,同时可以适量植骨以防止远期骨丧失[16];延期种植时可能仅需进行简单的植骨处理。
第2类牙齿(图4)的唇侧往往有一层较薄的骨板,但拔牙过程中有可能出现唇侧骨板折裂或开窗,如果选择即刻种植或早期种植,应注意选择合适直径的种植体,定点时稍偏腭侧,确保种植体植入时对唇侧骨板无压力,避免唇侧骨板因压力产生微裂纹而导致骨吸收[17];种植体与唇侧骨板之间应余留一定的间隙,留出足够的新骨再生空间[18],并进行骨增量。
这类牙齿在缺失后其唇侧骨板会有部分吸收,且骨丧失会随着时间的延长而加剧,因此在延期种植时,为了获得唇侧软硬组织长期的生物学稳定性和良好的美学效果,种植体植入后一般需要进行同期引导骨再生(guided bone regeneration,GBR)[19]来保证种植体唇侧骨板的厚度。
第3类牙齿(图5)多数唇侧骨板菲薄或缺如,根尖区尤为明显。拔牙时唇侧骨板容易出现折断或缺损,拔除后极易发生唇侧骨板萎缩吸收,长期缺牙后多表现为骨厚度严重不足,并伴不同程度的骨高度不足,故延期种植时需大量植入人工骨粉,或者进行自体块状骨移植[20]。另外,由于此类牙齿与牙槽骨长轴的角度较大,按修复引导的理念进行即刻种植或早期种植时,种植体将会因唇侧骨板的菲薄或缺如而难以获得初期稳定性[13]。因此这类牙齿的种植治疗具有较高的难度和挑战性,需谨慎处理。术前通过CBCT观察可在一定程度上预测此类牙齿延期种植修复的困难,建议于拔牙同期进行拔牙窝植骨、位点保留[21],从而减少牙槽窝改建造成的骨丧失,为延期种植创造良好的手术条件。
总之,术前通过CBCT观察上颌前牙与牙槽骨的关系(特别是牙体长轴与牙槽骨长轴的唇舌向偏移关系),可以指导种植时机,种植体植入位置(方向、角度、深度)以及骨增量方案的选择。
[1] Berkovitz BKB, Holland GR, Moxham BJ. Oral anatomy, histology and embryology[M]. 3th ed. Edinburgh: Mosby, 2002:12-35.
[2] Yoshimine S, Nishihara K, Nozoe E, et al. Topographic analysis of maxillary premolars and molars and maxillary sinus using cone beam computed tomography[J]. Implant Dent, 2012, 21(6):528-535.
[3] 王美青. 口腔解剖生理学[M]. 7版. 北京: 人民卫生出版社, 2012:75-76.
Wang MQ. Oral anatomy and physiology[M]. 7th ed. Beijing: People’s Medical Publishing House, 2012:75-76.
[4] Kan JY, Roe P, Rungcharassaeng K, et al. Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study[J]. Int J Oral Maxillofac Implants, 2011, 26(4):873-876.
[5] 朱一博, 邱立新. 上颌切牙解剖分型与种植方案的选择[J]. 中华口腔医学杂志, 2013, 48(4):223-225.
Zhu YB, Qiu LX. Anatomical classification of maxillary incisors and options of implant strategy[J]. Chin J Stomatol, 2013, 48(4):223-225.
[6] 孙婷婷, 潘瑾, 崔明军, 等. 基于CT影像的牙种植模板相关的颌骨解剖学研究[J]. 口腔颌面外科杂志, 2007, 17(3): 252-255.
Sun TT, Pan J, Cui MJ, et al. Observation and measurement of maxilla alveolar data related to dental implant template [J]. J Oral Maxillofac Surg, 2007, 17(3):252-255.
[7] 王艳辉, 赵保东, 陈秀娟, 等. 上颌前牙倾斜度测量在种植义齿中的应用[J]. 山东医药, 2008, 48(31):93-94.
Wang YH, Zhao BD, Chen XJ, et al. Application of measuring the inclination of the maxillary anterior teeth in implant dentures[J]. Shandong Med J, 2008, 48(31):93-94.
[8] Gracco A, Gemelli S, Lombardo L, et al. Upper incisor intrusion: an anatomical analysis via CBCT[J]. Int Orthod, 2011, 9(2):210-223.
[9] 周慧, 王洋, 曹阳. 不同垂直骨面型尖牙区牙槽骨形态的锥形束CT研究[J]. 中华口腔医学研究杂志: 电子版, 2011, 5(6):621-627.
Zhou H, Wang Y, Cao Y. A cone beam computed tomography study of canine alveolar morphology in different vertical skeletal types[J]. Chin J Stomatol Res: Electron Ed, 2011, 5(6):621-627.
[10] 孙伟, 周力, 白丁, 等. 不同垂直骨面型正常人切牙区颌骨形态结构正常值的建立[J]. 实用口腔医学杂志, 2005, 21(1):124-127.
Sun W, Zhou L, Bai D, et al. Cephalometric standards for incisal jaw morphology in the subjects with normal occlusion and different vertical facial skeletal types[J]. J Pract Stomatol, 2005, 21(1):124-127.
[11] 韩科. 种植义齿: 背景·选择·计划·操作[M]. 北京: 人民军医出版社, 2007:244-250.
Han K. Implant denture: background·option·treatment plan· operation[M]. Beijing: People’s Military Medical Press, 2007: 244-250.
[12] Kim JH, Lee JG, Han DH, et al. Morphometric analysis of the anterior region of the maxillary bone for immediate implant placement using micro-CT[J]. Clin Anat, 2011, 24(4): 462-468.
[13] Lau SL, Chow J, Li W, et al. Classification of maxillary central incisors-implications for immediate implant in the esthetic zone[J]. J Oral Maxillofac Surg, 2011, 69(1):142-153.
[14] Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog[J]. J Clin Periodontol, 2005, 32(2):212-218.
[15] Kao HC, Gung YW, Chung TF, et al. The influence of abutment angulation on micromotion level for immediately loaded dental implants: a 3-D finite element analysis[J]. Int J Oral Maxillofac Implants, 2008, 23(4):623-630.
[16] Buser D, Chen ST, Weber HP, et al. Early implant placement following single-tooth extraction in the esthetic zone: biologic rationale and surgical procedures[J]. Int J Periodontics Restorative Dent, 2008, 28(5):441-451.
[17] Kohal RJ, Hürzeler MB, Mota LF, et al. Custom-made root analogue titanium implants placed into extraction sockets. An experimental study in monkeys[J]. Clin Oral Implants Res, 1997, 8(5):386-392.
[18] Tomasi C, Sanz M, Cecchinato D, et al. Bone dimensional variations at implants placed in fresh extraction sockets: a multilevel multivariate analysis[J]. Clin Oral Implants Res, 2010, 21(1):30-36.
[19] Buser D, Bornstein MM, Weber HP, et al. Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: a cross-sectional, retrospective study in 45 subjects with a 2- to 4-year follow-up[J]. J Periodontol, 2008, 79(9):1773-1781.
[20] 梁晋, 姜宝岐, 兰晶, 等. 环状植骨术同期牙种植临床效果的短期观察[J]. 华西口腔医学杂志, 2014, 32(1):40-44.
Liang J, Jiang BQ, Lan J, et al. Short-term evaluation of clinical effect of bone ring grafting and immediate insertion [J]. West Chin J Stomatol, 2014, 32(1):40-44.
[21] Wang HM, Shen JW, Yu MF, et al. Analysis of facial bone wall dimensions and sagittal root position in the maxillary esthetic zone: a retrospective study using cone beam computed tomography[J]. Int J Oral Maxillofac Implants, 2014, 29(5):1123-1129.
(本文编辑 吴爱华)
The influence of angulation of maxillary anterior teeth on treatment design of dental implants
Liu Jin1, Pu Bishuang2, Xia Yulan2, Wang Chengze2, Wang Gang2, Lan Jing2. (1. Dept. of Prosthodontics, School of Stomatology, Shandong University, Jinan 250012, China; 2. Dept. of Implantology, School of Stomatology, Shandong University, Jinan 250012, China)
Correspondence: Lan Jing, E-mail: kqlj@sdu.edu.cn.
Objective This study aims to analyze the angulation of the maxillary anterior teeth relative to the alveolus to provide reference data for clinicians on the best conditions for implant placement in the esthetic zone. Methods Numerous cone beam computed tomography (CBCT) images were reviewed and screened. A total of 150 maxillary images were selected by strict adherence to the defined inclusive criteria, with 75 images each from male and female patients (between the ages of 19 and 48 years at the time of CBCT scan). The maxillary anterior teeth were gathered into the following three groups for males and females: upper canines, upper lateral incisors, and upper central incisors. Then, the long axis of each qualified tooth and its corresponding alveolar process were drawn, and the angles formed by these structures were measured. The resultant data were analyzed by SPSS 19.0. Results The long axis of the maxillary anterior teeth all inclined to the palatal side of the alveolar process. The internal angle (α) formed by the long axis of the maxillary central incisors and the long axis of the alveolar bone presented a mean value of 16.22° (range: 2.50°-28.80°) for male subjects and 15.20° (range: 2.20°-27.20°) for female subjects. The internal angle (α) of the maxillary lateral incisors exhibited a mean value of 17.50° (range: 3.80°-29.50°) for male subjects and 15.99° (range: 4.10°-33.30°) for female subjects. Finally, the internal angle (α) of the maxillary canines presented a mean value of 16.27° (range: 1.00°-31.50°) for male subjects and 15.01° (range: 3.50°-27.40°) for female subjects. Conclusion The long axis of the maxillary anterior teeth all inclined to the palatal side of the alveolar process. For implant placement, careful preoperative analysis and evaluation with CBCT may be beneficial for avoiding the risk factors and achieving a high probability of success in the esthetic region.
cone beam computed tomography; the long axis of tooth; the long axis of alveolar bone; esthetic zone; dental implant
R 783
A
10.7518/hxkq.2016.06.012
2016-05-05;
2016-09-23
刘金,住院医师,硕士,E-mail:liujinhappy@aliyun.com
兰晶,副教授,博士,E-mail:kqlj@sdu.edu.cn
猜你喜欢
装备维修技术(2022年3期)2021-12-06 17:38:01
口腔医学(2021年10期)2021-12-02 02:07:54
中学数学研究(广东)(2021年19期)2021-11-19 12:56:46
实用口腔医学杂志(2021年1期)2021-04-28 03:15:08
实用口腔医学杂志(2021年2期)2021-04-27 07:10:32
南京医科大学学报(自然科学版)(2021年1期)2021-02-26 09:30:08
中学数学研究(江西)(2019年12期)2020-01-10 06:39:02
中成药(2018年8期)2018-08-29 01:28:32
海南医学(2016年8期)2016-06-08 05:43:00
水电站机电技术(2014年4期)2014-10-13 08:30:13