血管内超声和血流储备分数测定在冠状动脉临界病变治疗中的作用*
2016-12-16 03:22李伯艳赵庆霞史苏娜曾春燕贾风顺张艳丽
重庆医学 2016年33期
李伯艳,赵庆霞,史苏娜,曾春燕,李 霞,李 虎,贾风顺,张艳丽,纪 征△
(1.华北理工大学研究生院,河北唐山 063000;2.河北省唐山工人医院心内科 063000)
血管内超声和血流储备分数测定在冠状动脉临界病变治疗中的作用*
李伯艳1,赵庆霞2,史苏娜1,曾春燕1,李 霞2,李 虎2,贾风顺2,张艳丽1,纪 征2△
(1.华北理工大学研究生院,河北唐山 063000;2.河北省唐山工人医院心内科 063000)
目的 比较血管内超声检查(IVUS)和血流储备分数测定(FFR)在指导冠状动脉临界病变治疗中的临床效果。方法 将94例行冠状动脉造影提示冠状动脉临界病变的患者分为IVUS组和FFR组,分别接受IVUS或FFR检查,并以此为依据指导冠状动脉介入治疗。在IVUS组中,如MLA<4 mm2或冠状动脉狭窄虽不足,但 IVUS 显示为不稳定斑块,则行冠状动脉介入治疗(PCI);在FFR组中,以FFR<0.75作为行冠状动脉支架置入术的指征。术后随访6个月,比较两组患者心血管不良事件的发生情况。结果 (1)两组患者病史等一般信息及冠状动脉造影情况差异无统计学意义(P>0.05)。(2)IVUS组行介入治疗的比例高于FFR组(P<0.01)。(3)两组间不良事件的发生情况差异无统计学意义(P>0.05)。结论 IVUS和FFR检查均可用于指导冠状动脉临界病变的介入治疗,受准确性的限制IVUS不能取代FFR检查的地位。
血管内超声;血流储备分数测定;冠状动脉临界病变
冠状动脉临界病变指在冠状动脉造影中提示中等程度的病变,多认为其管腔狭窄程度为50%~70%[1],在冠状动脉造影以及冠状动脉介入治疗中均常见。研究显示,6%的临界病变会在1年之内发展为急性冠状动脉事件而需要冠状动脉介入治疗,需要介入治疗的冠状动脉病变中87%是先前冠状动脉造影小于60%的病变[2]。正确的评价冠状动脉临界病变对冠状动脉血供的影响至关重要。仅通过冠状动脉造影或冠状动脉造影定量分析判断冠状动脉的狭窄程度不能满足临床决策的需要。血管内超声检查(IVUS)和血流储备分数测定(FFR)的出现和发展给冠状动脉临界病变的临床决策提供了依据。本研究旨在比较二者在指导冠状动脉临界病变治疗中的临床效果,现报道如下。
1 资料与方法
1.1 一般资料 将2014年7月至2015年6月唐山工人医院心内一科行冠状动脉造影提示冠状动脉临界病变的患者分为IVUS组和FFR组,分别接受IVUS或FFR检查,并以此为依据指导冠状动脉介入治疗(PCI)。在IVUS组中,如MLA<4 mm2或冠状动脉狭窄虽不足,但 IVUS 显示为不稳定斑块,则行PCI 治疗[3],否则采用药物保守治疗;在FFR组中,以FFR<0.75[4]作为行冠状动脉支架置入术的指征。两组术前、术后均给予标准的冠心病药物治疗。排除标准:(1)因急性冠状动脉综合征行急诊PCI术者;(2)有左主干病变、心肌病及存在严重威胁生命的疾病;(3)既往有心肌梗死病史或曾行PCI治疗者;(4)已行冠状动脉旁路移植术者;(5)对腺苷、阿司匹林及氯吡格雷、药物涂层支架禁忌者。(6)预期寿命小于2年者。本研究共入组96例患者,其中1例随访中因胰腺癌去世,1例检查结果建议行PCI治疗患者拒绝,以上2例不符合入选标准被剔除,最终纳入统计分析的有94例患者,其中男64例,女30例;年龄41~77岁,平均(59.02±8.56)岁。IVUS组43例,FFR组51例。两组患者一般情况详见表1,两组患者性别、年龄及冠心病相关危险因素分布方面差异无统计学意义。两组冠状动脉造影所见冠状动脉狭窄程度、病变位置及单支病变和多支病变的分布无明显差异。
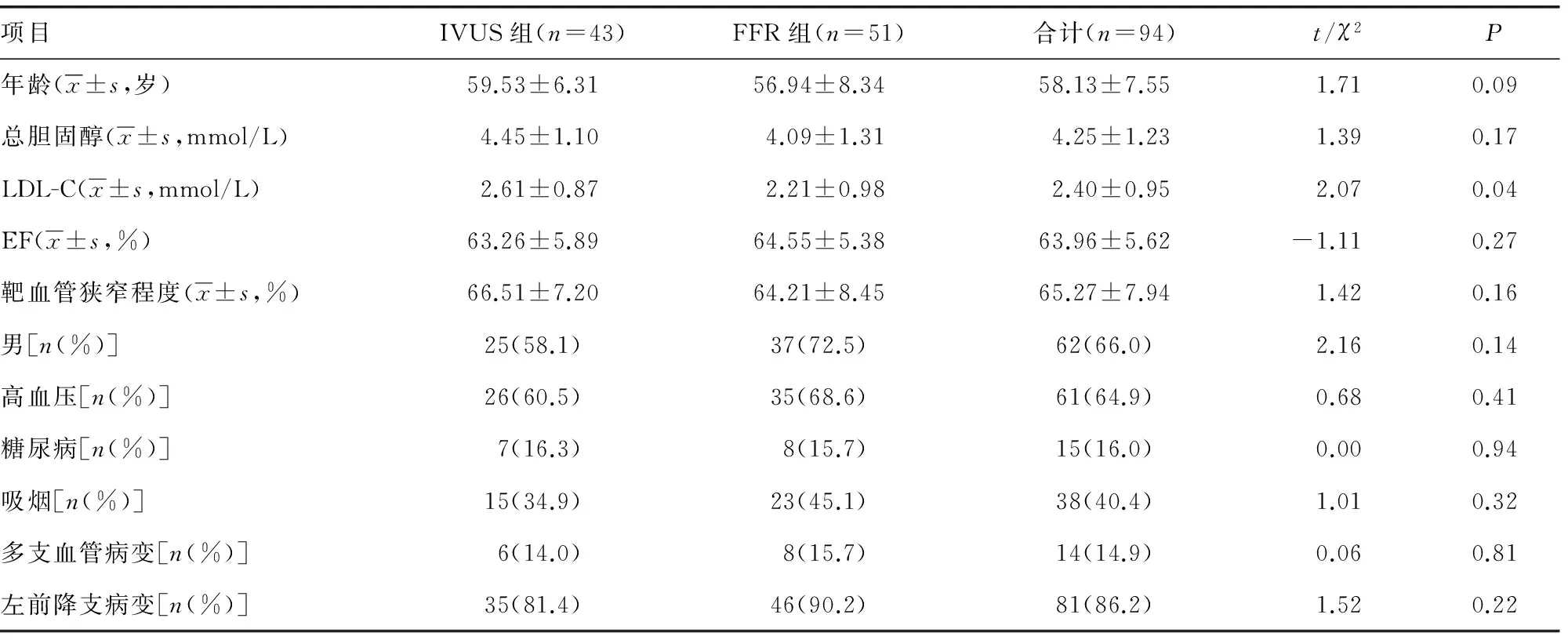
表1 患者的一般临床情况
LDL-C:低密度脂蛋白胆固醇;EF:超声心动测得左室射血分数。
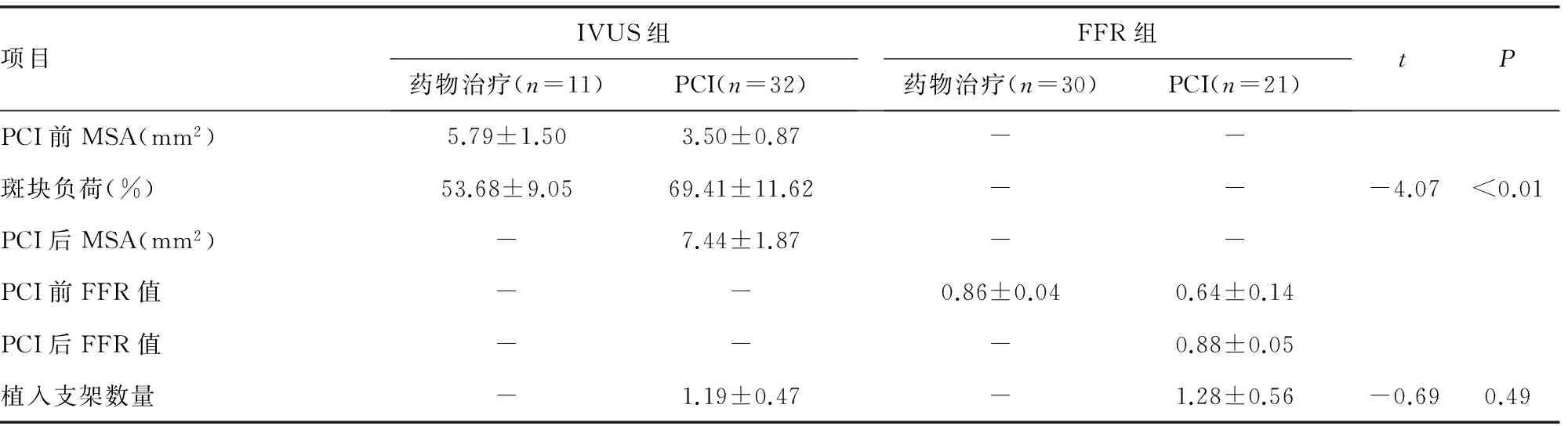
表2 两组患者的介入相关数据比较
PCI:经皮冠状动脉介入治疗;MSA:经血管内超声检查测得的最小管腔面积。
1.2 数据收集 (1)收集入组患者年龄、性别、既往病史(高血压、糖尿病、高脂血症)、吸烟情况、左室射血分数、冠状动脉造影病变情况(多支或单支、病变部位、狭窄程度)、患者PCI前后血管内超声最小管腔面积、斑块负荷情况或PCI前后FFR值以及支架数量等相关信息。(2)术后所有患者均以电话随访或门诊复查等形式随访6个月,详细记录患者术后服药情况、心绞痛发作情况、再发心肌梗死或缺血致靶病变再次血运重建、心血管全因死亡等主要心血管不良事件(MACE)。

2 结 果
IVUS组有32例(74.4%)行PCI治疗,FFR组21例(41.2%)行PCI治疗,IVUS组行介入治疗的比例高于FFR组(P<0.01)。随访期间经PCI治疗的IVUS组患者再次住院治疗的有5例(占15.63%),其中2例因病变进展行靶血管血运重建,3例症状发作频繁采用药物保守治疗;经PCI治疗的FFR组患者再次住院治疗的有2例(占9.52%),其中1例症状发作频繁采用药物保守治疗,1例因病变进展行靶血管血运重建,两组不良事件的发生情况差异无统计学意义(P=0.69)。未行PCI治疗的IVUS组患者再次住院治疗的有1例(占9.09%),因症状发作频繁采用药物保守治疗;未行PCI治疗的FFR组患者再次住院治疗的有2例(占6.67%),其中,1例症状发作频繁采用药物保守治疗,1例心源性死亡,两组不良事件的发生情况差异无统计学意义(P=0.08),见表2。
3 讨 论
IVUS检查较冠状动脉造影更能准确判断血管狭窄程度,此外该检查还能分析斑块性质以判断斑块的稳定性,指导PCI治疗。FFR检查从功能学评估血流灌注以指导介入治疗。虽然IVUS以MLA<4 mm2为诊断标准的敏感性达88%,特异性达90%,但其检查结果与心肌血流再灌注情况并不完全相符[5]。另有小型研究显示[6],对于中等程度狭窄的冠状动脉,IVUS指导下的斑块负荷提示血流灌注障碍的病变中有50%的病变FFR值大于0.75。本研究提示IVUS组PCI治疗的比例大于FFR组,与既往研究结果相符。研究[7-9]提示临界病变中IVUS的测量结果与FFR值有中等程度的相关性,其评价标准受狭窄所在血管大小及供血面积等的影响,应根据病变的不同部位制订相应的标准。此外亦有研究显示[10-11],冠状动脉临界病变的灌注不仅仅受局部部分狭窄的影响,而是由病变弥漫在传导血管中的总的斑块体积决定的,提出动脉粥样硬化斑块总体积与FFR结果有较强的相关性。本研究两种检查指导下的介入治疗的再住院率及不良事件并无差异,与此前的研究结果相似[12-13]。但本研究样本量小,随访时间尚短对预后的观察及判断有一定的影响。总之受准确性的限制,在指导临界病变的介入治疗中,IVUS不能取代FFR检查的地位。
[1]Jacobs AK,Smith SC,Anderson JL,et al.2011 ACCF/AHA/SCAI the diagnosis and treatment of hypertropnic cardiomyopathy:executive summary[J].Circulation,2011,124(24):2761-2796.
[2]Glaser R,Selzer F,Faxon DP,et al.Clinical progression of incidental,asymptomatic lesions discovered during culprit vessel coronary intervention[J].Circulation,2005,111(2):143-149.
[3]Bourantas CV,Naka KK,Garg S,et al.Clinical indications for intravascular ultrasound imaging[J].Echocardiography,2010,27(10):1282-1290.
[4]Tonino PA,De Bruyne B,Pijls NH,et al.Fractional flow reserve versus angiography for guiding percutaneous coronary intervention[J].N Engl J Med,2009,360(3):213-224.
[5]Nishioka T,Amanullah AM,Luo H,et al.Clinical validation of intravascular ultrasound imaging for assessment of coronary stenosis severity:comparison with stress myocardial perfusion imaging[J].J Am Coll Cardiol,1999,33(7):1870-1878.
[6]Rodés-Cabau J,Candell-Riera J,Angel J,et al.Relation of myocardial perfusion defects and nonsignificant coronary lesions by angiography with insights from intravascular ultrasound and coronary pressure measurements[J].Am J Cardiol,2005,96(12):1621-1626.
[7]Waksman R,Legutko J,Singh J,et al.FIRST:fractional flow reserve and intravascular ultrasound relationship study[J].J Am Coll Cardiol,2013,61(9):917-923.
[8]Kang SJ,Ahn JM,Song H,et al.Usefulness of minimal luminal coronary area determined by intravascular ultrasound to predict functional significance in stable and unstable angina pectoris[J].Am J Cardiol,2012,109(7):947-953.
[9]Cui M,Zhu D,Guo LJ,et al.Usefulness of lumen area parameters determined by intravascular ultrasound to predict functional significance of intermediate coronary artery stenosis[J].Chin Med J(Engl),2013,126(9):1606-1611.
[10]Yang HM,Tahk SJ,Lim HS,et al.Relationship between intravascular ultrasound parameters and fractional flow reserve in intermediate coronary artery stenosis of left anterior descending artery:intravascular ultrasound volumetric analysis[J].Catheter Cardiovasc Interv,2014,83(3):386-394.
[11]Jin XJ,Tahk SJ,Yang HM,et al.The relationship between intravascular ultrasound-derived percent total atheroma volume and fractional flow reserve in the intermediate stenosis of proximal or middle left anterior descending coronary artery[J].Int J Cardiol,2015,185(1):56-61.
[12]de la Torre Hernandez JM,Lopez-Palop R,Garcia CT,et al.Clinical outcomes after intravascular ultrasound and fractional flow reserve assessment of intermediate coronary lesions[J].Euro Interv,2013,9(7):824-830.
[13]Nam CW,Yoon HJ,Cho YK,et al.Outcomes of percutaneous coronary intervention in intermediate coronary artery disease:fractional flow reserve-guided versus intravascular ultrasound-guided[J].JACC Cardiovasc Interv,2010,3(8):812-817.
Application of intravascular ultrasound and fractional flow reserve on treatment of coronary intermediate lesion*
LiBoyan1,ZhaoQingxia2,ShiSuna1,ZengChunyan1,LiXia2,LiHu2,JiaFengshun2,ZhangYanli1,JiZheng2△
(1.NorthChinaUniversityofScienceandTechnologyGraduateAcademy,Tangshan,Hebei063000,China; 2.DepartmentofCardiology,TangshanWorkers′Hospital,Tangshan,Hebei063000,China)
Objective To compare the clinical effects of intravascular ultrasound (IVUS) and blood flow reserve fraction (FFR) in guiding the treatment of critical disease of coronary artery.Methods Forty-nine patients with coronary artery disease who underwent coronary angiography were divided into IVUS group (n=43) and FFR group (n=51).In IVUS group, such as MLA <4 mm2or coronary artery stenosis was insufficient, but IVUS showed unstable plaque, and we went the PCI treatment; in the FFR group, FFR<0.75 was regarded as coronary stenting sign. The patients were followed up for 6 months. The incidence of cardiovascular adverse events was compared between the two groups. Results (1)There was no significant difference in general information and coronary angiography between the two groups(P>0.05).(2)The proportion of interventional therapy in IVUS group was higher than that in FFR group (P<0.01).(3)The incidence of adverse events between the two groups was not statistically significant (P>0.05).Conclusion IVUS and FFR examination can be used to guide the interventional treatment of critical disease of coronary artery. However, the accuracy of IVUS can not replace the status of blood flow reserve.
intravascular ultrasound; fractional flow reserve; intermediate coronary lesion
��·临床研究
10.3969/j.issn.1671-8348.2016.33.021
河北省卫计委基金资助项目(20150944)。 作者简介:李伯艳(1990-),硕士,主要从事心血管内科方面的工作。△
R543.3
A
1671-8348(2016)33-4672-03
2016-04-02
2016-07-06)
猜你喜欢
中华实用诊断与治疗杂志(2022年2期)2022-09-02
自我保健(2021年2期)2021-11-30
妇女之友(2021年9期)2021-09-26
昆明医科大学学报(2021年2期)2021-03-29
中国生殖健康(2020年8期)2021-01-18
昆明医科大学学报(2020年11期)2020-12-28
百姓生活(2019年2期)2019-03-20
中国生殖健康(2018年3期)2018-11-06
中国医学装备(2015年10期)2015-12-29
医学研究杂志(2015年6期)2015-07-01