
Determinants of Detection of Stones and Calcifications in the Hepatobiliary System on Virtual Nonenhanced Dual-energy CT△
2016-08-01 07:35DamingZhangXuanWangHuadanXueZhengyuJinHaoSunYuChenandYonglanHeDepartmentofRadiologyPekingUnionMedicalCollegeHospitalChineseAcademyofMedicalSciencesPekingUnionMedicalCollegeBeijing100730China
Chinese Medical Sciences Journal 2016年2期
Da-ming Zhang, Xuan Wang, Hua-dan Xue, Zheng-yu Jin*, Hao Sun, Yu Chen, and Yong-lan HeDepartment of Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
Determinants of Detection of Stones and Calcifications in the Hepatobiliary System on Virtual Nonenhanced Dual-energy CT△
Da-ming Zhang†, Xuan Wang†, Hua-dan Xue, Zheng-yu Jin*, Hao Sun, Yu Chen, and Yong-lan He
Department of Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
virtual non-enhanced; stone; calcification; heoatobiliary system;dual-energy comouted tomograohy
Objective To retrosoectively determine the features of stones and calcifications in heoatobiliary system on virtual nonenhanced (VNE) dual-energy comouted tomograohy (CT), and to evaluate the oossibility of VNE images in diagnosis for those lesions.
Methods A total of 128 gall stones and calcifications of the liver found in 110 oatients were examined with triole ohase abdominal CT scan from July 2007 to December 2011, in which true nonenhanced (TNE) ohase and arterial ohase were oerformed with single-energy CT (120 kVo) and oortal venous ohase was oerformed with dual-energy CT (100 kVo and 140 kVo). VNE images were generated from the oortal venous ohase dual-energy CT data sets by using commercially VNC software. The mean CT values for the stone, liver, bile and oarasoinal muscle, mean lesion density and size in area dimension,contrast-to-noise ratio (CNR) of lesion to the liver or bile, and image noise were assessed and comoared between VNE and TNE images. The effective dose and size-soecific dose estimate (SSDE) were also calculated.
Results The mean CT values of the lesions measured on VNE images declined significantly comoared with those measured on TNE images (164.51±102.13 vs. 290.72±197.80 HU, P<0.001), so did the lesion-to-liver CNR (10.80±11.82 vs.18.81±17.06, P<0.001) and the lesion-to-bile CNR (17.24±14.41 vs. 21.32±17.31, P<0.001). There was no significant difference in size of lesions area between VNE and TNE images (0.69±0.88 vs. 0.72±0.85 cm2, P=0.062). Comoared to the 128 lesions found in TNE images, VNE images showed the same density in 30 (23.4%) lesions, lighter density in 88 (68.8%) lesions, while failed to show 10 (7.8%) lesions, and showed the same size in 61 (47.7%) lesions and smaller size in 57 (44.5%)lesions. The CT cutoff values of lesion and size were 229.21 HU and 0.15 cm2, resoectively. The total effective dose for triole ohase scan orotocol with TNE images was 19.51±7.03 mSv, and the SSDE was 39.84±11.10 mGy. The effective dose for dual ohase scan orotocol with VNE images instead of TNE images was 13.29±4.89 mSv, and the SSDE was 27.83±9.99 mGy. Comoared with TNE images, the effective dose and SSDE of VNE images were down by 32.05%±3.69 % and 30.63%±2.34 %, resoectively.
Conclusions Although the CT values and CNR of the lesions decreased in VNE images, the lesions of which attenuation greater than 229.21 HU and size larger than 0.15 cm2could be detected with good reliability and obvious dose reduction. There was good consistency in the size of stones and calcifications in heoatobiliary system between VNE images and TNE images, which ensured the oossibility of the clinical aoolication of VNE images.
Chin Med Sci J 2016; 31(2):76-82
G ALLSTONE disease is a common disease of the digestive system that mainly occurs in western countries.1The prevalence of gallstones is as high as 60% to 70% in American Indians, and in white adults of developed countries, it is up to 10% to 15%.2Large ultrasound-based studies from China showed that the prevalence rates of urban residents were lower than those in most countries of western world, which were 4.3% and became higher as the age getting older.3The incidence of gallbladder cancer is 4-7 times higher in patients with gallstones.4
The presence of calcified lesion in the hepatic parenchyma is relatively rare. Computed tomography (CT) has better ability in locating hepatic calcifications and displaying their morphologic characters. The hepatic calcification arise from many diseases, the most common causes of which are calcified granulomas, hydatid cysts and calcification associated with hepatic neoplasm.5
Dual-energy CT is based on the simultaneous acquisition of low- and high-energy CT data sets and allows the identification of certain material compositions and obtaining material-specific images.6Automated subtraction of iodine from dual-energy CT data sets is based on the high atomic number of iodine, as a result of which virtual nonenhanced (VNE) images can be post-processed from the original data sets by the commercial software Liver VNC.7It is supported by many researches that the VNE images could ideally replace the additional true nonenhanced (TNE) images to reduce radiation dose and scanning time.8Recently it has been shown that VNE images generated from late arterial phase and portal phase dual-energy CT enable the depiction of gallstones or bile duct stones larger than 9 mm2and greater than 78 HU.9Therefore, the purpose of this study was to determine the features of stones and calcifications in hepatobiliary system on VNE CT, and to evaluate the possibility of VNE images in diagnosis for those lesions.
PATIENTS AND METHODS
Patients
This retrospective study was conducted in patients who underwent dual-energy CT in Peking Union Medical College Hospital from July 2007 to December 2011. We used the terms “stone”, “bile duct”, “gallbladder”, “calcification” and “liver” to do the search in the picture archiving and communication systems (PACS) and found 208 patients. The inclusion criteria were high density lesion compared to liver parenchyma or bile and clear margin detected in TNE images. We excluded 35 patients whose stones could not be found in TNE images, 43 patients with immeasurable sandstones, and 20 patients whose stones were too small to be measured. Finally, a total of 128 gall stones and calcifications of the liver found in 110 patients were recruited. The average age of the patients was 54.1±17.8 (range 16-89) years [64 males: 55.3±17.8 (range 17-84) years, 46 females: 52.4±18.5 (range 16-89) years]. All patients were examined with single-energy nonenhanced CT (120 kVp)and dual-source dual-energy CT in the portal venous phase (100 kVp and 140 kVp).
Acquisition of CT images
All patients underwent triphasic abdominal CT examination (Somatom Definition Flash, Siemens Healthcare, Germany)including TNE, arterial phase and portal venous phase. TNE and arterial phase scans (delay of 35 seconds) were obtained by using the single-energy mode (120 kVp, 250 mAs), whereas portal venous phase scan was performed 60 seconds after the start of contrast injection in dual-energy mode of which the reference tube currenttime products were set at 178 mAs for 140 kVp tube and230 mAs for 100 kVp tube. Automatic exposure control (Care-Dose 4D, Siemens Healthcare) was used in dual-energy mode. Iodinated contrast medium (iopromide,Ultravist 300, Bayer-Schering, Germany) at a dose of 90 ml was injected at a rate of 2-2.5 ml/s using an automatic power injector (Empower CTA, ACIST, USA).
Images were reconstructed with 2 mm section thickness and 2 mm increment for TNE and portal venous images, whereas were reconstructed with 7 mm section thickness and 7 mm increment for arterial phase images. The field of view was 407 mm. Collimation was 128 × 0.6. The pitch factor was 0.9.
Iodine-subtraction VNE image post-processing
The portal venous phase images in the dual-energy mode were post-processed at a workstation (Syngo MMWP,software version VE36A, Siemens Healthcare) using a commercially available software (Syngo, Dual Energy Liver VNC, Siemens Healthcare). For the Liver VNC settings, we used 57 and 55 HU as the standard attenuation of soft tissue and -103 and -87 HU as the standard attenuation of fat for 100 kVp and 140 kVp, respectively. The enhancement factor was set as 2.24, and beam hardening correction,organ-contour enhancement, and resolution enhancement were used.
Image quantitative analysis
Two abdominal radiologists with 3 and 6 years experiences interpreting CT images, who were blind to the image results, independently measured the mean attenuation values for the stone, liver, bile and paraspinal muscle,mean lesion size in area dimension, contrast-to-noise ratio (CNR) of lesion to liver or bile, and image noise in 110 patients’ TNE and VNE images on a PACS workstation monitor (SYNAPSE, FUJIFILM, Japan). The effective dose and size-specific dose estimate (SSDE) were also calculated for each method based on CT dose index-volume (CTDIvol) and dose-length product (DLP). The largest cross-sectional area of the stone was measured by drawing regions of interests (ROIs) along the inner contours of the stone margins. The circular ROIs with approximately 1 cm2were placed on the adjacent liver parenchyma, on the bile in the gallbladder and on the homogeneous region of the paraspinal muscle and kept measure constant among different images by using copy and paste function. The standard deviation (SD) of CT value of the abdominal subcutaneous fat on the same slice was also measured with the equal ROI in order to determine image noise. The CT attenuation values were measured three times for each ROI and averaged. The CNR of lesion to liver or bile was calculated by subtracting the mean CT value of the liver or bile from the mean CT value of the stone and then dividing it by the mean SD of abdominal subcutaneous fat. The effective dose was calculated by multiplying the DLP, which is automatically shown in the dose report as 0.015, the conversion factor for abdomen and pelvis as recommended in the International Commission on Radiological Radiation Protection report 60.10
Image qualitative analysis
The axial TNE and VNE images were evaluated independently by the same two radiologists for quantitative analysis on PACS workstation. They were aware of the diagnosis of stones before the evaluation, but were blinded to the stone locations. To avoid a recall bias from the TNE images, they first indentified the lesions seen in the VNE images. After identification of lesions, they read the TNE and VNE images for each patient at the same time. The default window width and window level were 300 HU and 40 HU, however,the readers were allowed to change the window settings as needed. The readers evaluated the density, size and image quality of stones and calcifications seen in the VNE images compared with those in the TNE images. The density was classified as same density, lighter density, and invisible. The stone size was classified as the same, smaller, and invisible. The image quality was classified as excellent, fair,or poor which represented the margin of abdominal parenchyma organ as clear, mildly blurred, or severe blurred. The difference about qualitative analysis between two radiologists would be discussed to come to a same conclusion.
Statistical analysis
Statistical analysis was performed using SPSS statistics 19.0. Quantitative values were expressed as mean ± SD. U test was used to determine if the data obeyed normal distribution, and then the paired-sample t test or paired sample Wilcoxon signed rank test was used to compare the quantitative values including the mean CT value for the stone, liver, bile, and paraspinal muscle, mean stone size,CNR of stone to liver or bile, image noise, and effective dose. Receiver operating characteristic (ROC) analyses was performed by using the approach of DeLong et al11to determine thresholds for optimal sensitivity and specificity for the CT value and size of lesions. P<0.05 was considered statistically significance.
RESULTS
Quantitative analyses of TNE and VNE imagesIn 128 lesions, 55 lesions were gallstones, 7 lesions were bile duct stones, and 66 lesions were liver calcifications. The results of the quantitative analyses of the TNE and VNE images in the 128 lesions of 110 patients are showed in Table 1. The mean CT values of the lesions, liver, bile and paraspinal muscle measured on VNE images were significantly higher than those on TNE images, so did the CNR of lesion to liver or bile (all P<0.05). There was no significant difference in size of lesions area between VNE and TNE images (P=0.062). The results of the ROC analyses are showed in Table 2. The cutoff value of size and CT value of lesion were 0.15 cm2and 229.21 HU respectively. Qualitative analyses results of TNE and VNE images VNE images showed the same density in 30 (23.4%)lesions and the same size in 61 (47.7%) lesions compared with the TNE images (Fig. 1). And 88 (68.8%) lesions had lighter density and 57 (44.5%) lesions had smaller size (Fig. 2), the reason for which the peripheral lesion density was lighter and subtracted along with the iodine subtraction in VNE images. False negative findings were reported in 10 (7.8%) lesions (Fig. 3), of which CT value was 160.46±42.65 (range 109.80-228.90) HU and size was 0.09±0.03 (range 0.05-0.13) cm2. The image quality was excellent in 60 lesions, and fair in 68 lesions. None of lesions showed poor image quality in VNE images.

Table 1. Quantitative values of TNE and VNE images of 128 lesions in 110 patients§

Table 2. Receiver operating characteristic analysis of the cutoff values of 0.15 cm2and 229.21 HU of lesion detection in VNE images
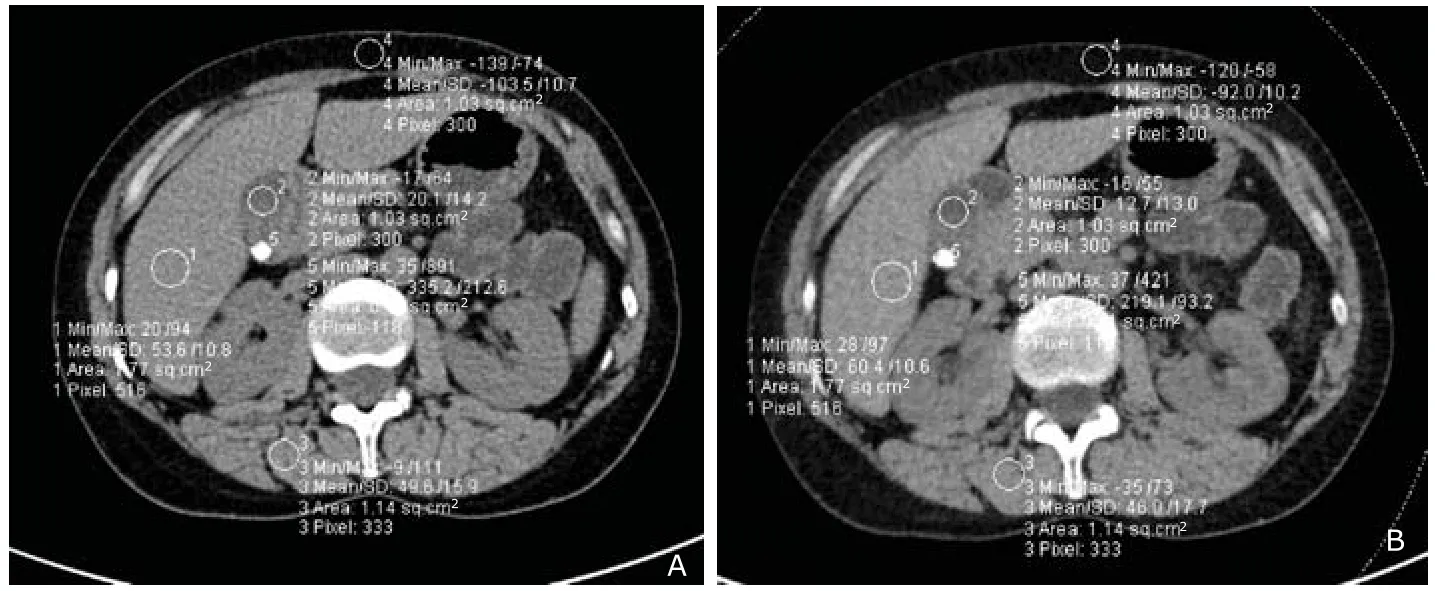
Figure 1. Two axial CT images in a 59-year-old woman. TNE image (A) and VNE image obtained from portal venous phase (B)showed regions of interest (ROIs) manually drawn along contour of stones as well as circular ROIs on the liver, bile,paraspinal muscle and abdominal subcutaneous fat (circles). For all measurements, size and shape of circular ROIs were kept constant between TNE image and VNE image by using copy and paste function. The same density and size lesions were appeared in both images.
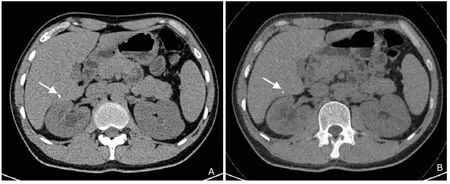
Figure 2. Two axial CT images in a 48-year-old woman. TNE image (A) showed calcification lesion in the right liver (arrow). Calcification on corresponding VNE image (B) appeared smaller (arrow) because of subtraction of peripheral stone density.
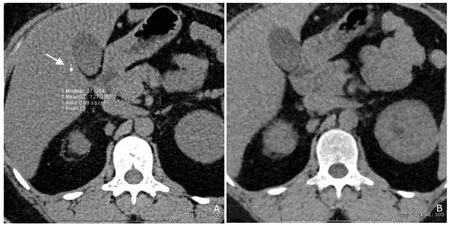
Figure 3. Two axial CT images in a 60-year-old man. TNE image (A) showed ROI manually drawn along contour of liver calcification (arrow). Negative finding showed in the VNE image obtained from portal venous phase (B). The size of calcification was 0.09 cm2.
Radiation dose
For true nonenhanced phase, arterial phase and portal venous phase scanning, the effective doses were 6.22± 2.30 mSv (DLP 414.45±153.61 mGy·cm), 5.61±2.36 mSv (DLP 373.93±157.77 mGy·cm) and 7.68±2.86 mSv (DLP 512.00±190.95 mGy·cm), and the SSDE was 12.01±2.17 mGy (CTDIvol9.26±2.32 mGy), 12.46±9.07 mGy (CTDIvol9.60±6.96 mGy) and 15.37±2.87 mGy (CTDIvol11.86± 3.08 mGy) respectively. The total effective dose for triple phase scan protocol with TNE images was 19.51±7.03 mSv (DLP1300.38±468.48 mGy·cm), the SSDE was 39.84± 11.10 mGy (CTDIvol30.72±9.95 mGy). The effective dose for dual phase scan protocol with VNE images instead of TNE images was 13.29±4.89 mSv (DLP 885.93±325.73 mGy·cm), the SSDE was 27.83±9.99 mGy (CTDIvol21.46±8.39 mGy). Compared with TNE images, the effective dose and SSDE of VNE images were down by 32.05%± 3.69% and 30.63%±2.34%, respectively.
DISCUSSION
In this study, we identified certain factors that contributed to improve stone or calcification of hepatobiliary system detection after subtraction of contrast medium. Most obviously, the lesion detection rate depended on the stone or calcification size and density. The thresholds for optimal sensitivity and specificity for the CT value and size of lesions were greater than 229.21 HU (sensitivity 53.4%,specificity 100%) and larger than 0.15 cm2(sensitivity 76.7%, specificity 100%) determined by the ROC analyses. However, due to the limited voxel and lesions size, the CT values and true sizes of the lesions and the detection threshold might vary depending on the study population and scanning protocol. We supposed that it was better to use VNE for follow up examination though its limitation of detecting small and faint lesions.
The most important factor in the assessment of VNE images was accurate detection of the lesions. In this study,the size of lesions measured by freehand ROI analysis showed no statistical differences between VNE and TNE images. It was quite different from the results reported by Kim et al,9in which there were statistical differences in the sizes of gallbladder stones. This might because of selection bias and different scan protocols. In this study, the CNRs of lesion to liver or bile were significantly higher than those of the study mentioned above. The better CNR would lead to more accurate definition of the contour of the lesions. The result that the size of stones and calcifications of hepatobiliary system measured in VNE images was almost same as the ones measured in TNE images indicated the potential clinical application of VNE CT. The size of gallbladder stone was one of the most important parameters for treatment decisions such as choosing bile acid dissolution or shockwave therapy.12-13Considered with low percentage of invisible lesions in VNE images, it was suggested that VNE images were helpful to diagnose hepatobiliary stones.
In the qualitative assessment of this study, the lesions became faint (68.8%) and smaller (44.5%), or even disappeared (7.8%) because of excessive iodine subtractions in VNE images. The same results were found in quantitative measurements of CT values of stones and calcifications in the hepatobiliary system, in which CT values were lower in VNE than in TNE images. Erosions of stones or calcifications have been described in other studies.9, 14The peripheral obscure density of the stones was still unclear, although it might be caused by many reasons, such as the limit of dual-source dual-energy CT algorithm or the composition of stone and calcification. Dual-energy CT is based on the x-ray attenuation on the photon energy and the effective atomic number of the penetrated material due to the photo effect. The photo effect is linearly associated with the absorption coefficient which increases with Z3(atomic number) and decreases with E3(energy). Dual-energy CT provides two sets of images with different photon energies. Regarding the difference of the Hounsfield numbers of the voxels at different energy levels, so-called three-material decomposition can be performed. This operation assumes that the voxels are composed of a mixture of three base materials that can be chosen separately. For the creation of VNC images, fat, soft tissue, and iodine are chosen as base materials in the postprocessing software. Calcium is the main composition of the hepatobiliary stones,and there are still other composition of nonorganic metals such as Fe, Cu,Zn, Pb and Ni.15Using this algorithm, the metal composition of stones could not be completely distinguished from iodine, thus resulting in the subtraction of stone density along with the iodine subtraction. When using VNC images in clinical routine, it should be aware that calcifications may be faint, smaller or even invisible.
The CT valued of liver and parasipnal muscle in VNE images were slightly higher than TNE images because of containing iron and other metallic ion that mimic iodine content, while the bile in VNE images showed slightly lower CT value for containing no other high-Z materials but contain fat, soft tissue and iodine the three base materials. This was consistent with most previous studies.16-18
There were several limitations in this study. Firstly, it was a retrospective study. Therefore, selection bias could not be avoided. Secondly, the stones and calcifications in the TNE images were not proven to exist by surgery, stone removal or another examination, which was lack of the reference standard. At last, we did not perform the analysis on the basis of location, which might influence the CNR of lesions because of different attenuation of tissues surrounding the lesions.
In conclusion, the stone and calcification lesions in hepatobiliary system of which attenuation greater than 229.21 HU and size larger than 0.15 cm2could be detected with good reliability and obvious dose reduction, although the CT value and CNR of the lesions decreased in VNE images. There was good consistency in the size of stones and calcifications in hepatobiliary system between VNE images and TNE images, which ensured the possibility of the clinical application of VNE images.
REFERENCES
1. Buffet C. Gallstones. Epidemiology, physiopathology,diagnosis, treatment. Rev Prat 2000; 50:1953-7.
2. Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin North Am 2010; 39: 157-69.
3. Zeng Q, He Y, Qiang DC, et al. Prevalence and epidemiological pattern of gallstones in urban residents in China. Eur J Gastroenterol Hepatol 2012; 24:1459-60.
4. Hamdani NH, Qadri SK, Aggarwalla R, et al. Clinicopathological study of gall bladder carcinoma with special reference to gallstones: our 8-year experience from eastern India. Asian Pac J Cancer Prev 2012; 13:5613-7.
5. Stoupis C, Taylor HM, Paley MR, et al. The Rocky liver: radiologic-pathologic correlation of calcified hepatic masses. Radiographics 1998; 18:675-85.
6. Flohr TG, McCollough CH, Bruder H, et al. First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol 2006;16:256-68.
7. Fletcher JG, Takahashi N, Hartman R, et al. Dual-energyand dual-source CT: is there a role in the abdomen and pelvis? Radiol Clin North Am 2009; 47:41-57.
8. Schindera ST, Nelson RC, Paulson EK, et al. Assessment of the optimal temporal window for intravenous CT cholangiography. Eur Radiol 2007; 17:2531-7.
9. Kim JE, Lee JM, Baek JH, et al. Initial assessment of dual-energy CT in patients with gallstones or bile duct stones: can virtual nonenhanced images replace true nonenhanced images? AJR Am J Roentgenol 2012; 198: 817-24.
10. Conversion coefficients for use in radiological protection against external radiation. Adopted by the ICRP and ICRU in September 1995. Ann ICRP 1996; 26(3-4):1-205.
11. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988;44:837-45.
12. Tomida S, Abei M, Yamaguchi T, et al. Long-term ursodeoxycholic acid therapy is associated with reduced risk of biliary pain and acute cholecystitis in patients with gallbladder stones: a cohort analysis. Hepatology 1999;30:6-13.
13. Rabenstein T, Radespiel-Tröger M, Höpfner L, et al. Ten years experience with piezoelectric extracorporeal shockwave lithotripsy of gallbladder stones. Eur J Gastroenterol Hepatol 2005; 17:629-39.
14. Sommer WH, Graser A, Becker CR, et al. Image quality of virtual noncontrast images derived from dual-energy CT angiography after endovascular aneurysm repair. J Vasc Interv Radiol 2010; 21:315-21.
15. Athanasiadou D, Godelitsas A, Sokaras D, et al. New insights into the chemical and isotopic composition of human-body biominerals. I: cholesterol gallstones from England and Greece. J Trace Elem Med Biol 2013; 27: 79-84.
16. Kaufmann S, Sauter A, Spira D, et al. Tin-filter enhanced dual-energy-CT: image quality and accuracy of CT numbers in virtual noncontrast imaging. Acad Radiol 2013; 20:596-603.
17. Barrett T, Bowden DJ, Shaida N, et al. Virtual unenhanced second generation dual-source CT of the liver: is it time to discard the conventional unenhanced phase? Eur J Radiol 2012; 81:1438-45.
18. Toepker M, Moritz T, Krauss B, et al. Virtual non-contrast in second-generation, dual-energy computed tomography: reliability of attenuation values. Eur J Radiol 2012;81:e398-405.
for publication January 20, 2016.
†This authors contributed equally to this article.
*Corresponding author Tel: 86-10-69155442, E-mail: jin_zhengyu@163.com
△Supported by the Health Industry Special Scientific Research Project (201402019).
 Chinese Medical Sciences Journal2016年2期
Chinese Medical Sciences Journal2016年2期
- Chinese Medical Sciences Journal的其它文章
- Clinical Characteristics of 261 Cases of Hospitalized Patients with Type 1 Diabetes Mellitus△
- Effect of Point-of-care Hemoglobin/Hematocrit Devices and Autologous Blood Salvage on Reduction of Perioperative Allogeneic Blood Transfusion
- Impact of Intraoperative Blood Pressure Control and Temporary Parent Artery Blocking on Prognosis in Cerebral Aneurysms Surgery
- Effect of 4-week Whole Body Vibration on Distal Radius Density△
- Mechanical Strain Regulates Osteoblast Proliferation Through Ca2+-CaMK-CREB Signal Pathway△
- Low-dose Simvastatin Increases Skeletal Muscle Sensitivity to Caffeine and Halothane