
Knowledge,attitude and practice of healthcare workers concerning Crimean-Congo hemorrhagic fever in Western Iran
2016-06-14 02:41:45MojtabaSalimiAbbasAghaeiAfsharMojtabaLimoeeSorayaBabakhaniOmidChatrabgounAhmadAliHanafiBojdGidigloGodwinNutifafaDepartmentofMedicalEntomologyVectorControlSchoolofPublicHealthTehranUniversityofMedicalSciencesTUMSTehranIran
Mojtaba Salimi,Abbas Aghaei Afshar,Mojtaba Limoee,Soraya Babakhani,Omid Chatrabgoun,Ahmad Ali Hanafi-Bojd,Gidiglo Godwin NutifafaDepartment of Medical Entomology & Vector Control,School of Public Health,Tehran University of Medical Sciences(TUMS),Tehran,IranDepartment of Health Promotion and Network Expansion,Health Deputy,Kermanshah University of Medical Sciences,Kermanshah,IranLeishmaniasis Research Center,Kerman University of Medical Sciences,Kerman,IranDepartments of Public Health and Health Research Center,Kermanshah University of Medical Sciences,Kermanshah,IranDepartment of Mathematical,Statistics and Probability,Malayer University,IranDepartment of Medical Entomology & Vector Control,School of Public Health,International Campus,Tehran University of Medical Sciences,Tehran,Iran
ABSTRACT
Knowledge,attitude and practice of healthcare workers concerning Crimean-Congo hemorrhagic fever in Western Iran
Mojtaba Salimi1,2,Abbas Aghaei Afshar3*,Mojtaba Limoee4,Soraya Babakhani2,Omid Chatrabgoun5,
Ahmad Ali Hanafi-Bojd1,Gidiglo Godwin Nutifafa61Department of Medical Entomology & Vector Control,School of Public Health,Tehran University of Medical Sciences
(TUMS),Tehran,Iran
2Department of Health Promotion and Network Expansion,Health Deputy,Kermanshah University of Medical Sciences,
Kermanshah,Iran
3Leishmaniasis Research Center,Kerman University of Medical Sciences,Kerman,Iran
4Departments of Public Health and Health Research Center,Kermanshah University of Medical Sciences,Kermanshah,Iran5Department of Mathematical,Statistics and Probability,Malayer University,Iran
6Department of Medical Entomology & Vector Control,School of Public Health,International Campus,Tehran University of Medical Sciences,Tehran,Iran
ABSTRACT
Keywords:
Crimean-Congo hemorrhagic fever
Healthcare worker
Knowledge
Iran
ARTICLE INFO
Article history:
Received 15 Jan 2016
Received in revised form 12 Feb,2nd revised form 19 Feb 2016
Accepted 23 Mar 2016
Available online 22 Apr 2016
Original article http://dx.doi.org/10.1016/j.apjtb.2016.04.007
Tel: +98 341 3224616
E-mail: afshara2@yahoo.com
Thestudyprotocolwasapprovedbythe Ethic CommitteeofKermanshahUniversity of Medical Sciences which approved the investigations. Informed written consent was obtained from all participants in this study. Confidentiality on the content of the records was kept by the investigators and information was only utilized for the research purpose.
Foundation Project: Supported by Kerman University of Medical Sciences,Kerman,Iran(Grant No. 94251).
Peer review under responsibility of Hainan Medical University. The journal implements double-blind peer review practiced by specially invited international editorial board members.
1. Introduction
Crimean-Congo hemorrhagic fever(CCHF)is an acute hemorrhagicfevercausedbysegmented,negative-stranded RNAvirus belonging to the family Bunyaviridae,genus Nairovirus,which is the second most widespread of all medically important arboviruses,after dengue virus. Basically,this disease is transmitted to humans by domestic animals and bite of an infected tick or via aerosolgeneratedfrominfectedanimals'excreta.Humantohuman transmission occurs following contact with an infected person's blood,tissue or fluid discharge. The vectors of this arthropodborne disease are generally hard ticks of Ixodidae family,including some species of Rhipicephalus,Boophilus,Dermacentor and Hyalomma(in particular Hyalomma marginatum). Somespeciesof ArgasandOrnithodorosin Argasidaefamilyhave been reported to be infected[1-5]. The virus of the disease can be transmitted via transovarial transmission through the eggs of tick vectors to their next generation and can pass through different stages of their life cycle. Therefore,if a tick bites an infected vertebrate,it will be infected in all its life and can transmit the disease to humans by bites.
Climate has also been found as important predictor of CCHF risk;areas regularly experiencing long period of low rainfall and humiditywereassociatedwithincreasedincidenceof CCHFin Iran and Senegal,and higher temperatures were indicators of CCHF occurrence in Turkey,Bulgaria,and Iran[6,7]. Outbreak of the disease occurs in warm seasons when ticks are more active and questing hosts for blood feeding. Most cases were reported between April and September. Increasing mean temperature,normalized difference vegetation index,savannah-type land coverage or habitat fragmentation increased significantly the incidence of CCHF in the CCHF-affected areas[7]. Climate,environmental factors and human behavior that may influence CCHF epidemiology and spread should be further studied. Facilitated tick reproduction and global warming which are mainly attributed to climatic changes should be considered in the potential changing epidemiology of CCHF[8].
Hosts of the disease include a range of domestic and wild animals such as cattle,sheep and goat. The birds are resistant to infection but ostrich is sensitive. In endemic areas where human infection is the source,the disease is of high prevalence. There are no clinical symptoms in animals,and this increases the risk of infection in humans when slaughter the infected animal or contact animal's skin or carrion shortly after slaughtering. CCHF has been ranked as one of the most important nosocomial infections and hospitalized patients could infect others,for which reason they must be isolated. CCHF virus is on the US list of select agent consideredtohavebioterrorismpotentialbecauseofitsassociation with rapid-onset of hemorrhagic fever and 30%case fatality rate [5,8-10]. There is considerable difference among mortality rates of the disease in different parts of the world. The difference is not only related to that of diagnostic services-medical care,but also to virulence and pathogenicity of different virus strains across the world. For example,the disease is milder in South Russia with a mortalityrateof5%-10%,butin South Africaand Middle Eastthe mortality rates were reported as 35%and 35%-50%,respectively. It should be noted that the mortality was higher in hospital epidemics[11]. The World Health Organization has listed CCHF among the emerging diseases for which control and prevention measures should be renewed and intensified. According to our consensus measure,the five countries currently having the strongest evidence for presence of CCHF are Turkey,Iran,Afghanistan,Tajikistan,and Pakistan[12,13].
The disease has been reported in several countries from Africa (Senegal,Nigeria,South Africa,Kenya,Tanzania,Ethiopia,Mauritania,Congo,and Uganda),Europe(Bulgaria,Turkey,Albania,Kosovo,Greece,Yugoslavia,Hungary,Russia and Ukraine)and Asia(Iraq,Pakistan,India,Afghanistan,Oman,Iran,Chinaand United Arabic Emirates)[13,14],andimportedCCHFhas never been reported in Northern Europe or in America[15]. CCHF in Iran was first reported in 1970,when virus antibodies were identified in the sera of 45 sheep sent from Tehran to Moscow [16]. After that antibodies of the virus were detected in 13%of people who were living in Caspian Sea littoral from East Azerbaijan Province[17]. Mortality rate approaching 20%in 2 000 remarkably dropped to 6%in 2007. CCHF,however,is an emerging disease in the country. The disease exists in almost all parts of Iran according to the epidemiological evidences and confirmed cases[18]. In recent decades,confirmed human cases that resulted in death were reported in provinces of Sistan-va-Baluchestan,Khuzestan,Chaharmahal-va-Bakhtiari,Azerbaijane-Gharbi,Bushehr,Yazd,Kerman,Tehran,Esfahan,Golestan,Fars,Qom and Khorasan in Iran[6,14,18].
CCHF is an occupational disease for butchers,slaughter house workers,livestock workers,animal husbandry workers,veterinarians and healthcare workers who belong to the group of people at high risk of the disease in the endemic areas of CCHF[12]. In a survey conducted in south of Iran,livestock was identified as the source of infection and CCHF outbreak occurred via two routes: contact with tissue and blood of infected livestock,as well as nosocomial transmission[16]. Hence,the knowledge of people whoareincontactwiththediseaseshouldbeevaluatedperiodically.
Kermanshah Province is important from CCHF point of view because of cattle trafficking with infected areas,illegal slaughtering in the area and confirmed cases of disease and death in the neighboring provinces[11,12,19]. Therefore,it is necessary to evaluate the knowledge of at-risk occupational groups. The aim of this study was to evaluate the knowledge,attitude and practice of the healthcare staff as one of the high risk occupational groups of people towards CCHF.
2. Materials and methods
Kermanshah Province,located at the extreme west of Iran shares border with Iraq,and is located at the coordinates of 33.36-35.15°N and 45.24-48.30°E(Figure 1). The weather is moderate and both cold and warm regions can be found in the province. Annual mean temperature is reported as 15.4°C and the mean annual rainfall is recorded between 300 and 800 mm. The capital city is Kermanshah and 13 other cities are located in this province. There are many livestock farms in this province and CCHF virus has been detected from ticks and patients in recent years.

Figure 1. Mapof Iranandlocationof Kermanshah Provincein Western Iran.
2.1. Study population and sample size
This descriptive cross-sectional study was conducted on healthcare staff of Kermanshah Province in 2014 to determine their knowledge,attitude and practice concerning CCHF. A total of 367 healthcare workers were selected using cluster random sampling fromdifferent citiesof the provinceforinterview,based on the number of people employed in each occupational group.
2.2. Data collection and analysis
Data were collected by the use of a pre-designed questionnaire and interviews were conducted on healthcare staff in different occupational categories(physicians,nurses,midwives,laboratory staff and health network personnel). Questions covered demographic information,as well as knowledge(7 questions),attitudes(5 questions)and practice(4 questions)of the respondents about CCHF. Reliability of the questionnaire was examined based on a few staff members in occupational groups of health service providers. The collected data were analyzed using SPSS 16.0,Chi-square test,One-way ANOVA and least significant difference tests to find the correlation of knowledge,attitude and practice of the respondents with their job categories.
2.3. Ethical consideration
The study protocol was approved by Ethic Committee of Kermanshah University of Medical Sciences which approved the investigations. Informed written consent was obtained from all participants in this study. Confidentiality on the content of the records was kept by the investigators and information was only utilized for the research purpose.
3. Results
A total of 367 individuals were interviewed including 85 physicians,116 nurses,65 midwives,72 laboratory staff and 29 health network personnel. Among the interviewed population,49%of physicians,94%of nurses,17%of midwives and 91%of laboratory staff were employed in hospitals and other health centers. Academic education is the main source of knowledge acquisition about CCHF for physicians(62%),midwifes(53%)and health staff(33%);job training and press and media are the main sources of knowledge acquisition about CCHF for nurses(45%)and laboratory workers(39%),respectively(Figure 2).
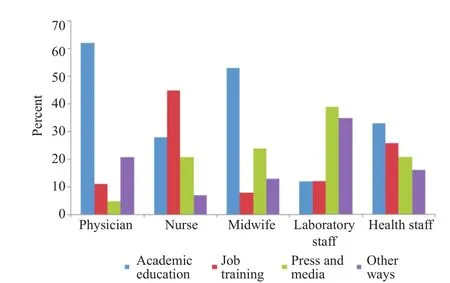
Figure 2. Main source of knowledge acquisition about CCHF in healthcare workers.
Regarding knowledge of the studied community,76%of physicians,78%of nurses,77%of midwives and 58%of laboratory staff believed that CCHF is treatable. The level of knowledge about transmission,reservoir host,treatment,dealing with patients and personal protection in physicians,nurses,midwives and laboratory staff in hospitals was lower than that of staff in health centers. Many occupational groups particularly in the private sector have not had enough information on their occupational hazards yet. By using Chi-square test,there was no significant relationship between job and level of knowledge (P>0.05),but with respect to One-way ANOVA there was significant relationship between the levels of knowledge in different occupational groups. This difference was significant between physician and nurse,nurse and laboratory worker,as well as nurse and health workers(P<0.05). The knowledge and awareness of occupational groups were compared as binary by least significant difference test. It was found that there is a significant difference between occupational groups(nurses and physicians,and laboratory staff and nurses). Level of knowledge in laboratory staff and physicians was higher than that in nurses (Table 1). In this study,there was no significant relationship between the place of work(urban or rural)and the level of their knowledge(P = 0.08). Concerning attitude,overall 88%of physicians,93%of nurses,97%of midwives and 92%of laboratory staff believed that CCHF patients must be isolated in the hospital(Table 1). About the prevention,95%of physicians,93%of nurses,92%of midwives and 96%of laboratory staff believed that prevention is essential for CCHF and control can avoid or minimize the exposure to the virus.

Table 1Results of the interview with various occupational groups in Kermanshah Province,Iran.%.

Table 1(continued)
4. Discussion
Transmission of CCHF through infected secretions and blood has put it as one of the most important nosocomial infections,and reports of outbreak of the disease in the hospital have ranked it as one of the main sources of infection among service providers and staff in health centers. Thus helping the healthcare providers to prevent the spread of the disease in a community and hospital setting has significant roles. The first priority and necessity in this regard is to assess the knowledge,attitude and practice of related staff as one of the high risk groups in order to find their weaknesses,so that essential steps can be taken to overcome the disease by designing a proper educational plan with assistance from related authorities at different educational and executive levels. This study refers to the role of education in promoting the knowledge of healthcare staff in the face of CCHF. According to the results,there was no significant relationship between job and level of knowledge. The results of this study confirmed those of previous studies conducted in other areas[13,16,20-24].
Despite results of Gozel et al. showing that CCHF virus is not easily transmitted from person to person through respiratory or physical contact,use of equipments to prevent transmission of this disease,including gloves,face masks,face visors and box coats,should be introduced to emergency room health care workers,and encouragement should be provided for using these equipments[15]. In this study we identified the use of personal protective equipment in some occupational groups,particularly those have direct contact with the disease. Some occupational groups,especially nurses,have direct contact with hospitalized patients. Therefore,their low level of knowledge about the disease is regarded as one of the important risk factors to the spread of this disease in the community. Another important point in these results is that most occupational groups did not consider their occupations as risk factors of the disease,and treatment with ribavirin in suspected cases and post-exposure prophylaxis for healthcare workers who potentially exposed to CCHF virus should be considered.
We found that level of knowledge in laboratory staff and physicians was higher than that in nurses. This finding is contrary to other studies which have assessed the knowledge of nurses at a high level[20,25,26]. Some other studies on healthcare workers concluded that educational programs,especially for nurses,plays a major role in prevention of disease transmission[12,27]. In Kermanshah Province,due to insufficient training of staff especially in the health sector where most of the selected nurses were from,their knowledge about CCHF was inadequate,and educational programs must be codified for them. Here,the role of insufficient job training,especially for high-risk groups is visible and should be considered by the relevant authorities. In conclusion,it is recommended that specific training courses be conducted for healthcare staff to recognize early symptoms of CCHF and include the disease in their initial differential diagnosis,thereby ensuring early detection of the disease. Strengthening national and regional surveillance is necessary to provide a clearer feature of CCHF in its geographically distributed area. Isolation facilities should be available in hospitals and strict adherence to safety measures must be learned and practiced by healthcare workers.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Acknowledgments
The authors are grateful to president of the health center of Kermanshah for his support as well as personnel of Kermanshah University of Medical Science for cooperation in this study. This study has received financial grant from Kerman University of Medical Sciences(Grant No. 94251).
References
[1]Duh D,Saksida A,Petrovec M,Ahmeti S,Dedushaj I,Panning M,et al. Viral load as predictor of Crimean-Congo hemorrhagic fever outcome. Emerg Infect Dis 2007;13(11): 1769-72.
[2]Messina JP,Pigott DM,Golding N,Duda KA,Brownstein JS,Weiss DJ,et al. The global distribution of Crimean-Congo hemorrhagic fever. Trans R Soc Trop Med Hyg 2015;109(8): 503-13.
[3]Tahmasebi F,Ghiasi SM,Mostafavi E,Moradi M,Piazak N,Mozafari A,et al. Molecular epidemiology of Crimean-Congo hemorrhagic fever virus genome isolated from ticks of Hamadan Province of Iran. J Vector Borne Dis 2010;47(4): 211-6.
[4]Telmadarraiy Z,Ghiasi SM,Moradi M,Vatandoost H,Eshraghian MR,Faghihi F,et al. A survey of Crimean-Congo haemorrhagic fever in livestock and ticks in Ardabil Province,Iran during 2004-2005. Scand J Infect Dis 2010;42(2): 137-41.
[5]W¨olfel R,Paweska JT,Petersen N,Grobbelaar AA,Leman PA,Hewson R,et al. Virus detection and monitoring of viral load in Crimean-Congo hemorrhagic fever virus patients. Emerg Infect Dis 2007;13(7): 1097-100.
[6]Chinikar S. An overview of Crimean-Congo hemorrhagic fever in Iran. Iran J Microbiol 2009;1(1): 7-12.
[7]Vescio FM,Busani L,Mughini-Gras L,Khoury C,Avellis L,Taseva E,et al. Environmental correlates of Crimean-Congo haemorrhagic fever incidence in Bulgaria. BMC Public Health 2012;12: 1116.
[8]Maltezou HC,Andonova L,Andraghetti R,Bouloy M,Ergonul O,Jongejan F,et al. Crimean-Congo hemorrhagic fever in Europe: current situation calls for preparedness. Euro Surveill 2010;15(10). 19504.
[9]Gozel MG,Bakir M,Oztop AY,Engin A,Dokmetas I,Elaldi N. Investigation of Crimean-Congo hemorrhagic fever virus transmission from patients to relatives: a prospective contact tracing study. Am J Trop Med Hyg 2014;90(1): 160-2.
[10]Vanhomwegen J,Alves MJ,ˇZupanc TA,Bino S,Chinikar S,Karlberg H,et al. Diagnostic assays for Crimean-Congo hemorrhagic fever. Emerg Infect Dis 2012;18(12): 1958-65.
[11]Sisman A. Epidemiologic features and risk factors of Crimean-Congo hemorrhagic fever in Samsun Province,Turkey. J Epidemiol 2013;23(2): 95-102.
[12]Yolcu S,Kader C,Kayipmaz AE,Ozbay S,Erbay A. Knowledge levels regarding Crimean-Congo hemorrhagic fever among emergency healthcare workers in an endemic region. J Clin Med Res 2014;6(3): 197-204.
[13]Ali Z,Kumar R,Ahmed J,Ghaffar A,Mureed S. Knowledge,attitude and practice of Crimean-Congo hemorrhagic fever among rural population of Baluchistan,Pakistan. A public health nutritional assessment of elderly in Islamabad: a mixed method study. J Publ Health 2013;3(4): 11-3.
[14]Ansari H,Shahbaz B,Izadi S,Zeinali M,Tabatabaee SM,Mahmoodi M,et al. Crimean-Congo hemorrhagic fever and its relationship with climate factors in southeast Iran: a 13-year experience. J Infec Dev Ctries 2014;8(6): 749-57.
[15]Gozel MG,Dokmetas I,Oztop AY,Engin A,Elaldi N,Bakir M. Recommended precaution procedures protect healthcare workers from Crimean-Congo hemorrhagic fever virus. Int J Infect Dis 2013;17(11): e1046-50.
[16]Izadi S,Salehi M,Holakouie-Naieni K,Chinikar S. The risk of transmission of Crimean-Congo hemorrhagic fever virus from human cases to first-degree relatives. Jpn J Infect Dis 2008;61(6): 494-6.
[17]Jabbari A,Tabasi S,Abbasi A,Alijanpour E. Crimean-Congo hemorrhagic fever: treatment and control strategy in admitted patients. Casp J Intern Med 2012;3(2): 443-4.
[18]Chinikar S,Ghiasi SM,Moradi M,Goya MM,Shirzadi MR,Zeinali M,et al. Geographical distribution and surveillance of Crimean-Congo hemorrhagic fever in Iran. Vector Borne Zoonotic Dis 2010;10(7): 705-8.
[19]Majeed B,Dicker R,Nawar A,Badri S,Noah A,Muslem H. Morbidity and mortality of Crimean-Congo hemorrhagic fever in Iraq: cases reported to the national surveillance system,1990-2010. Trans R Soc Trop Med Hyg 2012;106(8): 480-3.
[20]Ozer A,Miraloglu M,Ekerbicer HC,Cevik F,Aloglu N. Knowledge levels about Crimean-Congo hemorrhagic fever among midwifery and nursing students in Kahramanmaras,Turkey. Southeast Asian J Trop Med Public Health 2010;41(1): 77-84.
[21]Sharifi-Mood B,Mardani M,Keshtkar-Jahromi M,Rahnavardi M,Hatami H,Metanat M. Clinical and epidemiologic features of Crimean-Congo hemorrhagic fever among children and adolescents from southeastern Iran. Pediatr Infect Dis J 2008;27(6): 561-3.
[22]Sheikh NS,Sheikh AS,Sheikh AA. Knowledge,attitude and practices regarding Crimean-Congo haemorrhagic fever among healthcare workers in Balochistan. J Ayub Med Coll Abbottabad 2004;16(3): 39-42.
[23]Sharifinia N,Rafinejad J,Hanafi-Bojd AA,Biglarian A,Chinikar S,Baniardalani M,et al. Knowledge and attitudes of the rural population and veterinary and health personnel concerning Crimean-Congo hemorrhagic fever in Western Iran in 2012. Fla Entomol 2013;96(3): 922-8.
[24]Yilmaz R,Ozcetin M,Erkorkmaz U,Ozer S,Ekici F. Public knowledge and attitude toward Crimean Congo hemorrhagic fever in Tokat Turkey. Iran J Arthropod Borne Dis 2009;3(2): 12-7.
[25]Çilingiroˇglu N,Temel F,Altıntas¸H. Public's knowledge,opinions and behaviors about Crimean-Congo hemorrhagic fever: an example from Turkey. Kafkas Univ Vet Fak Derg 2010;16: S17-22.
[26]Mofleh JA,Ashgar RJ,Kakar RS,Zaidi SZ,Kazi BM. Nosocomial outbreak of Crimean-Congo hemorrhagic fever in Holy Family Hospital,Rawalpindi,Pakistan,2010. J Public Health Epidemiol 2013;5(4): 173-7.
[27]Taghdisi M,Sasooli H,Ramezani A. A study of level the nurse's knowledge of the CCHF disease in the Sistan. Zahedan J Res Med Sci 2012;13(1): 65.
Objective:To determine the knowledge,attitude and practice of healthcare workers in Kermanshah Province about Crimean-Congo hemorrhagic fever(CCHF).
Methods:This study was conducted in 2014 on healthcare personnel in different job categories including physicians,nurses,midwives,laboratory staff and network health staff of Kermanshah Province by direct interview.
Results:A total of 367 respondents who had more than 5 years of experience in their jobs were interviewed. Among them 91%of physicians and nurses,97%of midwives and health workers and 96%of laboratory staff stated that they had not been confronted with CCHF patients so far. Regarding knowledge,76%of physicians,78%of nurses,77%of midwives and 58%of laboratory staff believed that the disease is remediable. Most of the interviewed participants stated that the disease pertains to people who are in close contact with domestic animals,but they did not consider their own occupations as one of the risk factors. More than 70%of the respondents believed that the disease may exist in the province or their work field. Generally,the knowledge about CCHF was inadequate,with nurses having the lowest level of knowledge.
Conclusions:Knowledge of Kermanshah healthcare staff about CCHF was poor,especially nurses in a high risk job category. Therefore,it is necessary to conduct specific training programs for the disease identification,transmission,prevention,and treatment as well as the use of personal protection and safety devices.
*Corresponding author:Abbas Aghaei Afshar,Leishmaniasis Research Center,Kerman University of Medical Sciences,Kerman,Iran.
 Asian Pacific Journal of Tropical Biomedicine2016年6期
Asian Pacific Journal of Tropical Biomedicine2016年6期
- Asian Pacific Journal of Tropical Biomedicine的其它文章
- Epidemiological situation and molecular identification of cercarial stage in freshwater snails in Chao-Phraya Basin,Central Thailand
- Potential drug-drug interactions in pediatric wards of Gondar University Hospital,Ethiopia∶A cross sectional study
- Biofilm formation in clinical isolates of nosocomial Acinetobacter baumannii and its relationship with multidrug resistance
- Prevalence of latent eosinophilia among occupational gardeners at Babcock University,Nigeria
- Preliminary studies of acute and sub-chronic toxicity of the aqueous extract of Guibourtia tessmannii(Harms)J. Leonard stem barks(Caesalpiniaceae)in mice and rats
- Evaluation of the anticonvulsant activity of the essential oil of Myrothamnus moschatus in convulsion induced by pentylenetetrazole and picrotoxin