
Implantable Cardiac De fibrillators: Who Needs Them and Who Does Not?
2016-05-22 02:35:41RichardContiMDMACC
C. Richard Conti, MD, MACC
Cardiologists who see patients on a general cardiology service are beginning to see an increasing number of patients who have received a primary prevention implantable cardiac de fibrillator (ICD) but have never had it fire. There are additionally a number of patients who have inappropriate firing of ICDs. Inappropriate shocks occur in up to 40% of patients with an ICD. The main cause is supraventricular tachyarrhythmia , including sinus tachycardia, atrial fibrillation, and other rapid supraventricular arrhythmias.
An important question relates to whether one should ever turn off the ICD. Many elderly and/or feeble patients who have declared themselves DNR and should be considered for hospice care(e.g., end-stage renal disease, severe chronic lung disease, malignancy) are admitted to the hospital for reasons not related to ventricular arrhythmias. I think that anyone who is a candidate for a heart hospice should have the ICD turned off and be given comfort care only. This is not easy to do, particularly when relatives are making decisions.
Heart Hospice Instead of ICD
As far as a heart hospice is concerned, there comes a time when a cardiologist and the family must come to an agreement that it is time to focus on comfort care for the patient. In many instances, cardiologists will not give up even though aggressive medical or even surgical therapy is not prolonging a pleasant useful life. Instead it is prolonging death. This is true not only for the surgical procedures but also for the use of ICDs.
One of the goals we should be trying to attain is to de fine who might not need the ICD in the first place and to make the decision about comfort care before any device implantation. This decision requires the physician to spend a lot of time with the patient and the patient’s family when they are seen in the clinic.Since heart failure is a major reason that ICDs are implanted, it is useful to refer to what has been proposed by Stevenson and Desai [1]. They outline a method for selecting patients with heart failure for discussion about implantation of an ICD for primary prevention of sudden cardiac death (Figure 1).
When aggressive medical care or surgical therapy is futile, it is time for comfort care of the patient;however, it is sometimes very hard to convince families of the futility of aggressive treatment in patients who will soon die of chronic cardiac conditions. This is particularly true in patients with multiple arrhythmias being treated with amiodarone and devices such as ICDs.
An example of a symptomatic patient in whom an ICD might not be useful is the heart failure patient who has been treated appropriately with drugs and a biventricular pacer, yet whose quality of life has not improved and who remains bed-ridden. In this case, an ICD will not make the patient feel better, despite what the patient or the relatives think. In contrast, if medical therapy and biventricular pacing improve quality of life, then the addition of an ICD seems appropriate.
Determining End of Life
Keep in mind that all guideline-based recommendations for ICD implantation discourage implanta-tion in patients with a life expectancy of less than 1 year due to cardiac or noncardiac conditions.
No physician can predict the future for any individual patient, whether it be the cancer patient or the cardiac patient; however, it does seem to be much easier to predict the end of life for the former rather than for the latter. It is possible to use population data only when one is trying to predict end of life.These data can be useful to explain to the patient or family members but the physician should be honest with the patient and explain that population data may not apply to the individual.
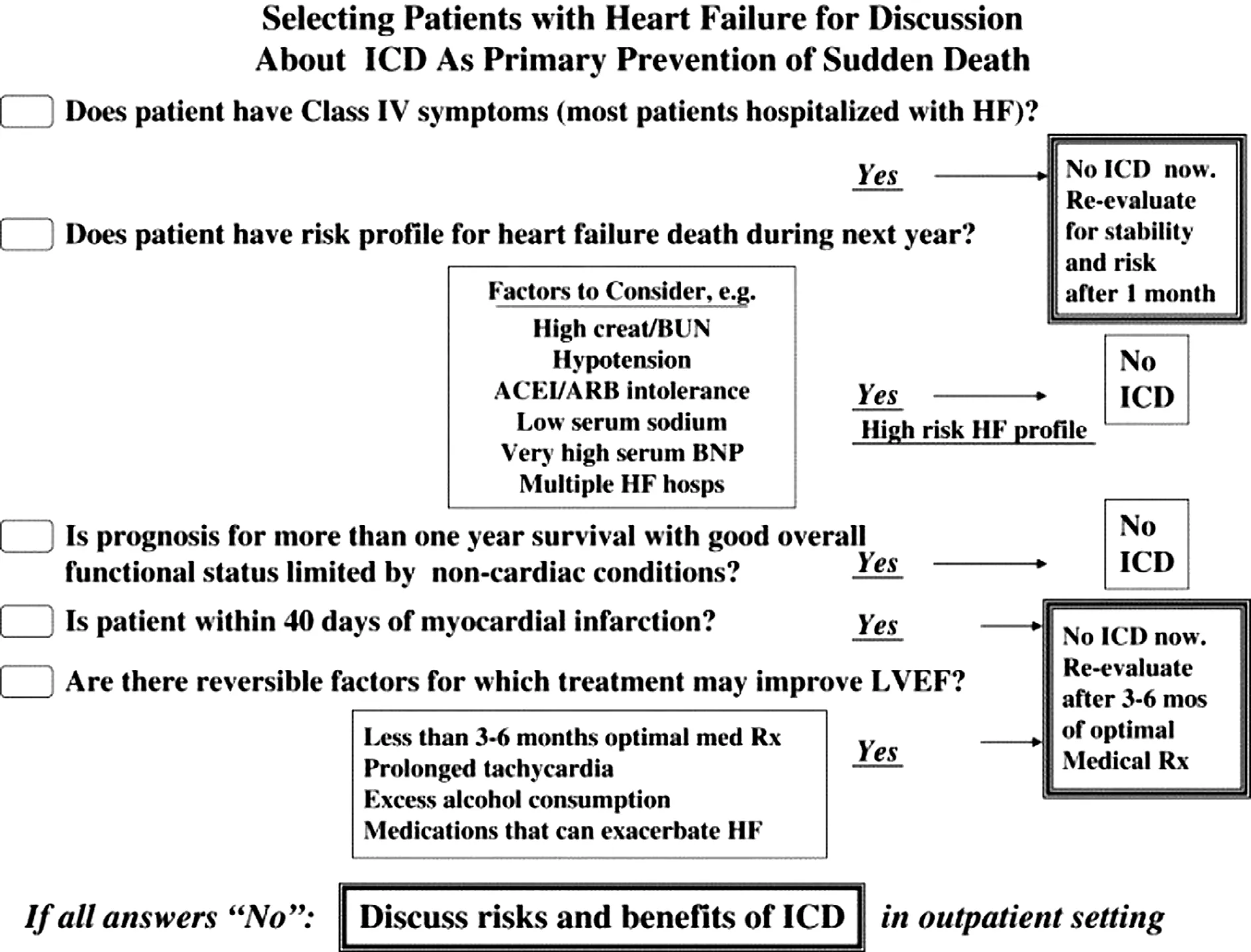
Figure 1 Method of Selecting Patients with Heart Failure for Discussion about Implantation of an ICD for Primary Prevention of Sudden Cardiac Death. Reprinted with Permission from [1].ACEI, Angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; BNP, brain natriuretic factor; BUN, blood urea nitrogen; HF, heart failure; ICD, implantable cardiac de fibrillator; LVEF, left ventricular ejection fraction.
Cost of Device Implantation
The cost of implanting a device is not trivial (the initial ICD implantation costs range from about$29,000 to $55,000, with annual follow-up costs ranging from $4800 to $17,000 total). The United States is the only country in which ICDs are used for primary prevention of sudden cardiac death in patients whose only risk factor is a decreased ejection fraction. This approach may be related to reimbursement in the United States. This approach is not the same in other countries. Worldwide, decisions to implant an ICD may not be left up to the physician.
Current Indications for ICD Implantation
What follows are the current indications for implantation of an ICD. It is important for the patient and the referring physician to understand the level of evidence for these recommendations.
There are several class I recommendations for ICD implantation. These include
· Patients with level of evidence A
1. Patients who have a left ventricular ejection fraction less than 35% due to myocardial infarction at least 40 days previously and who have heart failure
2. Patients with left ventricular dysfunction due to myocardial infarction at least 40 days previously with a left ventricular ejection fraction less than 30% and who have New York Heart Association functional class I heart failure
3. Patients who are survivors of cardiac arrest due to ejection fraction or hemodynamically unstable sustained ventricular tachycardia (VT)after evaluation to de fine the cause of the event and to exclude any completely reversible causes
· More class I recommendations but with level of evidence B
1. Patients with nonischemic dilated cardiomyopathies with a low ejection fraction (i.e., less than 35%) who have heart failure
2. Patients with nonsustained VT due to myocardial infarction, left ventricular ejection fraction less than 40%, and inducible ventricular fibrillation (VF) or sustained VT at the time of an electrophysiologic study
3. Patients with structural heart disease and spontaneous sustained VT whether hemodynamically stable or unstable
4. Patients with syncope, undetermined cause, with clinically relevant, hemodynamically signi fi-cant, sustained VT, or VF induced at the time of an electrophysiologic study
· Class II b recommendations with level of evidence B: Patients with long QT syndrome who are receiving β-blockers but experience syncope or VT
· Class II b recommendations with level of evidence C; this category is consensus opinion
1. Unexplained syncope, “signi ficant” left ventricular dysfunction, and nonischemic cardiomyopathy
2. Sustained VT and normal or near normal left ventricular function
3. Syncope, polymorphic VT secondary to catecholamergic factors while patients are receiving β-blockers
4. Arrhythmogenic right ventricular dysplasia patients who have one or more risk factors for sudden cardiac death
5. Brugada syndrome patients without symptoms
6. Cardiac sarcoidosis, giant cell myocarditis,or Chagas disease
7. Nonhospitalized patients awaiting transplantation
ICD Implantation Not Meeting Guidelines
It has been estimated that about 23% of patients receive an ICD implant although they do not meet the guidelines. These include patients receiving the ICD
1. Immediately after a myocardial infarction.
2. In the early stages of heart failure.
3. Within 3 months of cardiac surgery.
4. Patients with advanced heart failure who are unable to perform any activity. These patients tend to be older or have other morbid disease,such as end-stage renal disease, diabetes,severe chronic lung disease, or cancer.
5. Patients with ventricular tachyarrhythmias due to a completely reversible disorder in the absence of structural heart disease (e.g., electrolyte imbalance, drugs, or trauma).
6. Patients who do not have a reasonable expectation of survival with an acceptable functional status for at least 1 year, even if they otherwise meet the ICD implantation criteria.
7. Patients with incessant VT or VF.
8. Patients with signi ficant psychiatric illnesses that may be aggravated by device implantation or that may preclude systematic follow-up.
9. Patients with New York Heart Association class IV heart failure that is refractory to optimal medical treatment and who are not candidates for cardiac transplantation or cardiac resynchronization therapy.
10. Patients with syncope without inducible ventricular tachyarrhythmias and without structural heart disease.
11. Patients with VF or VT amenable to surgical or catheter ablation (e.g., atrial arrhythmias associated with Wolff-Parkinson-White syndrome, right ventricular or left ventricular out flow tract VT, idiopathic VT. or fascicular VT in the absence of structural heart disease) [2].
When the physician is advising an individual patient about the implantation of an ICD, the patient is entitled to know the bene fits and the risks. It is also imperative that the physician knows the patient’s expectations about life expectancy and quality of life.
Closing Remark
Finally, my advice to those who implant ICDs is“think before you implant an ICD” and have the patient and the family think before an ICD is implanted.
REFERENCES
1. Stevenson LW, Desai AS. Selecting patients for discussion of the ICD as primary prevention for sudden death in heart failure. J Card Fail 2006;12(6):407-12.
2. Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA, Gettes LS, et al. ACC/AHA/HRS 2008 guidelines for devicebased therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation 2008;117(21):e350.
 Cardiovascular Innovations and Applications2016年1期
Cardiovascular Innovations and Applications2016年1期
- Cardiovascular Innovations and Applications的其它文章
- The Subcutaneous Implantable Cardioverter-De fibrillator: A Practical Review and Real-World Use and Application
- Syncope and Early Repolarization: A Benign or Dangerous ECG Finding?
- Changing the Way We “See” Scar:How Multimodality Imaging Fits in the Electrophysiology Laboratory
- Stroke Prevention in Atrial Fibrillation:Current Strategies and Recommendations
- Principles of Arrhythmia Management During Pregnancy
- Current Management of Ventricular Tachycardia:Approaches and Timing