
胃癌患者手术前后外周血D-二聚体与CA724水平测定及意义
2016-03-07 05:37彭方兴袁三英吴宸陈进罗亮陈汇
海南医学 2016年22期
彭方兴,袁三英,吴宸,陈进,罗亮,陈汇
(绵阳市四〇四医院川北医学院附属第二医院胃肠外科,四川 绵阳 621000)
胃癌患者手术前后外周血D-二聚体与CA724水平测定及意义
彭方兴,袁三英,吴宸,陈进,罗亮,陈汇
(绵阳市四〇四医院川北医学院附属第二医院胃肠外科,四川 绵阳 621000)
目的 测定胃癌患者手术前后外周血中D二聚体(D-D)、糖类抗原724(CA724)表达水平,并探讨其临床意义。方法选择2014年1月至2015年3月在我院胃肠外科接受治疗的56例胃癌患者作为胃癌组,另选取56例胃良性病变患者和56例健康体检者分别纳入胃良性病变组及健康对照组。比较各组受检者的D-D及CA724水平,分析胃癌患者病理指标与D-D及CA724水平的关系,以及影响胃癌患者D-D及CA724水平升高的相关因素。结果治疗前,胃癌组及胃良性病变组患者的D-D及CA724水平均明显高于健康对照组,且胃癌组患者的D-D及CA724水平明显高于胃良性病变组,差异均有统计学意义(P<0.05);治疗后,胃癌组患者的D-D及CA724水平仍明显高于健康对照组,差异均有统计学意义(P<0.05),而胃良性病变组患者的D-D及CA724水平与健康对照组相比,差异均无统计学意义(P>0.05);胃癌浆膜层浸润的患者D-D及CA724水平均明显高于固有层及肌层浸润者,有淋巴结转移的患者D-D及CA724水平均明显高于无淋巴结转移者,低分化者D-D及CA724水平均明显高于中、高分化者,差异均有统计学意义(P<0.05);将胃癌患者D-D及CA724水平升高作为因变量,将浆膜层浸润和有淋巴结转移,以及低分化作为自变量,实施Logistic回归分析发现,浆膜层浸润和有淋巴结转移,以及低分化均为胃癌患者D-D及CA724水平升高的相关因素(P<0.05)。CA724以6.90 U/mL为临界值时,单独CA724监测胃癌的敏感度、准确度均为83.93%,D-D以0.50 mg/L为临界值时,单独CA724监测胃癌的敏感度、准确度均为82.21%,当D-D及CA724联合监测时,其敏感度及准确度均为96.43%(54/56),提示D-D及CA724联合监测对于胃癌的诊断价值明显高于单独D-D及CA724监测,差异有统计学意义(χ2单独D-D=5.973,χ2单独CA724=4.940,均P<0.05)。结论胃癌患者手术前后监测外周血D-D及CA724指标水平可较好地反映其疾病情况,值得临床推荐。
胃癌;外周血;D二聚体;糖类抗原724;测定;临床意义
胃癌是一种十分常见的恶性肿瘤,由其导致的死亡率在癌症中位居首位。对于胃癌标志物的研究,以往较为注重癌胚抗原(CEA)等指标,虽然亦可在一定程度上反映患者的病情,但敏感度仍有待提高[1]。近年来,国外有报道称,外周血中D二聚体(D-D)及糖类抗原724(CA724)联合检测可能对胃癌诊断鉴别更具价值[2]。鉴于国内在此方面的报道极少,本文展开研究,旨在为胃癌的治疗提供参考依据。
1 资料与方法
1.1 一般资料 选择2014年1月至2015年3月在我院胃肠外科接受治疗的56例胃癌患者作为研究对象。所有患者均符合WHO关于胃癌的临床诊断标准[3],并经影像学手段检测证实。56例患者中男性34例,女性22例;年龄38~68岁,平均(62.3±3.6)岁;管状腺癌8例,乳头状腺癌26例,黏液腺癌15例,印戒细胞癌7例。所有患者均接受胃癌根治术治疗,术后4周后开始行化疗治疗,化疗时间为4~8周。另选56例胃良性病变患者和56例健康体检者分别纳入胃良性病变组及健康对照组。其中胃良性病变组中男性32例,女性24例;年龄35~66岁,平均(61.9±2.8)岁;胃炎46例,胃溃疡10例。健康对照组中男性30例,女性26例;年龄35~67岁,平均(61.7±3.2)岁。各组受检者在性别和年龄等方面比较差异均无统计学意义(P>0.05),具有可比性。
1.2 研究方法 各组受试者在治疗前及治疗后12周(健康对照组在体检时测定)采集血液标本6 mL,使用产于德国的罗氏E170型电化学发光仪测定CA724指标水平。所用试剂均是罗氏原装试剂,其中CA724的正常参考值范围为<6.90 U/mL。使用Sysmex CA-7000全自动血凝分析仪(日本希森美康公司)检测D-D水平,其中D-D的正常参考值范围为<0.50 mg/L。将手术病理检查作为金标准,分析胃癌患者D-D及CA724水平监测价值,计算联合监测的敏感度及准确度。
1.3 观察指标 比较各组受试者的D-D及CA724水平,分析胃癌患者病理指标与D-D及CA724水平的关系,以及影响胃癌患者D-D及CA724水平升高的相关因素。
1.4 统计学方法 应用SPSS13.0统计软件进行数据分析,计数数据比较采用χ2检验,计量数据以均数±标准差(±s)表示,组间比较采用t检验,采用Logistic回归法分析影响因素,以P<0.05为差异有统计学意义。
2 结果
2.1 各组受检者的D-D和CA724水平比较 治疗前胃癌组及胃良性病变组的D-D及CA724水平均显著高于健康对照组,且胃癌组的D-D及CA724水平显著高于胃良性病变组,差异均有统计学意义(均P<0.05),治疗后胃癌组的D-D及CA724水平显著高于健康对照组,差异有统计学意义(P<0.05),而胃良性病变组的D-D及CA724水平与健康对照组比较差异无统计学意义(P>0.05),见表1。
表1 各组受检者D-D和CA724水平比较(±s)

表1 各组受检者D-D和CA724水平比较(±s)
注:与治疗前比较,t胃癌组D-D=142.76,t胃癌组CA724=26.32,t胃良性病变组D-D=44.56,t胃良性病变组CA724=7.07,aP<0.05;与健康对照组比较,t胃癌组D-D治疗前=157.90,t胃癌组D-D治疗后=22.83,t胃良性病变组D-D治疗前=54.88;t胃癌组CA724治疗前=54.77,t胃癌组CA724治疗后=38.59,t胃良性病变组CA724治疗前=8.59,bP<0.05。
组别 时间D-D(mg/L)CA724(U/mL)胃癌组(n=56)胃良性病变组(n=56)健康对照组(n=56)治疗前治疗后治疗前治疗后-2.05±0.08b0.42±0.03ab1.13±0.11b0.32±0.08a0.31±0.02 29.46±3.68b14.25±2.27ab3.65±1.02b2.46±0.74a2.42±0.33
2.2 胃癌患者病理指标与D-D及CA724水平的关系 胃癌浆膜层浸润的患者D-D及CA724水平均显著高于固有层及肌层浸润者,有淋巴结转移的患者D-D及CA724水平均显著高于无淋巴结转移者,低分化者D-D及CA724水平均显著高于中、高分化者,差异均有统计学意义(均P<0.05),见表2。
表2 胃癌患者病理指标与D-D及CA724水平的关系(±s)
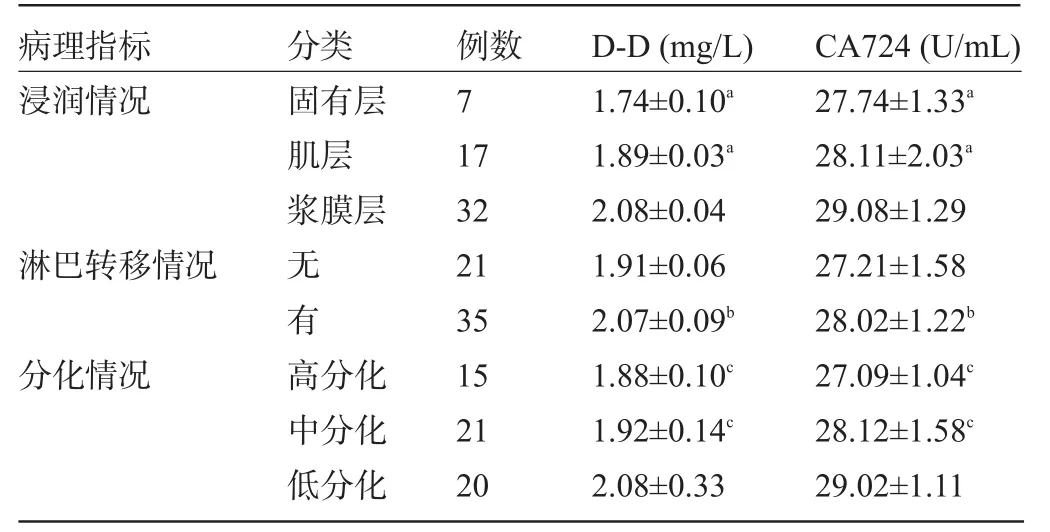
表2 胃癌患者病理指标与D-D及CA724水平的关系(±s)
注:a表示与浆膜层比较,t固有层D-D=14.97,t肌层D-D=17.16,t固有层CA724=2.48,t肌层CA724=2.04;b表示与无淋巴转移比较,t淋巴转移D-D=7.23,t淋巴转移CA724= 2.15;c表示与低分化相比较,t高分化D-D=2.26,t中分化D-D=2.04,t高分化CA724= 5.23,t中分化CA724=2.10。
病理指标CA724(U/mL)分类 例数D-D(mg/L)浸润情况27.74±1.33a28.11±2.03a29.08±1.29 27.21±1.58 28.02±1.22b27.09±1.04c28.12±1.58c29.02±1.11固有层肌层浆膜层淋巴转移情况 无有分化情况 高分化中分化低分化7 17 32 21 35 15 21 20 1.74±0.10a1.89±0.03a2.08±0.04 1.91±0.06 2.07±0.09b1.88±0.10c1.92±0.14c2.08±0.33
2.3 影响胃癌患者D-D及CA724水平升高的相关因素 将胃癌患者D-D及CA724水平升高作为因变量,将浆膜层浸润和有淋巴结转移,以及低分化作为自变量,实施Logistic回归分析发现,浆膜层浸润和有淋巴结转移,以及低分化均为胃癌患者D-D及CA724水平升高的相关因素,见表3。
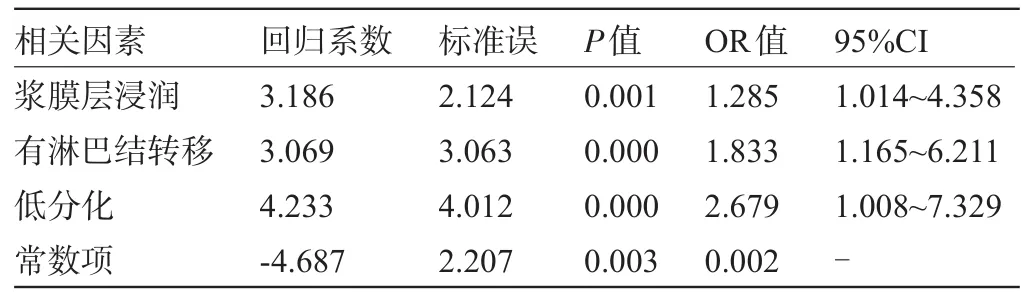
表3 影响胃癌患者D-D及CA724水平升高的相关因素分析
2.4 胃癌患者D-D及CA724水平监测价值 CA724以6.90 U/mL为临界值时,单独CA724监测胃癌的敏感度、准确度均为83.93%,D-D以0.50 mg/L为临界值时,单独CA724监测胃癌的敏感度、准确度均为82.21%,当D-D及CA724联合监测时,其敏感度及准确度均为96.43%(54/56),提示D-D及CA724联合监测对于胃癌的诊断价值明显高于单独D-D及CA724监测,差异有统计学意义(χ2单独D-D=5.973,χ2单独CA724= 4.940,均P<0.05),但单独D-D及CA724监测对于胃癌的诊断价值基本相同,差异无统计学意义(χ2= 0.063,P>0.05),见表4~表6。
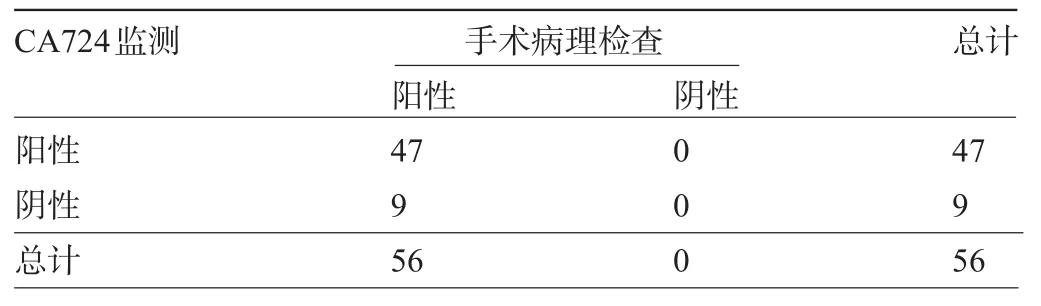
表4 胃癌患者CA724水平监测价值(例)

表5 胃癌患者D-D水平监测价值(例)
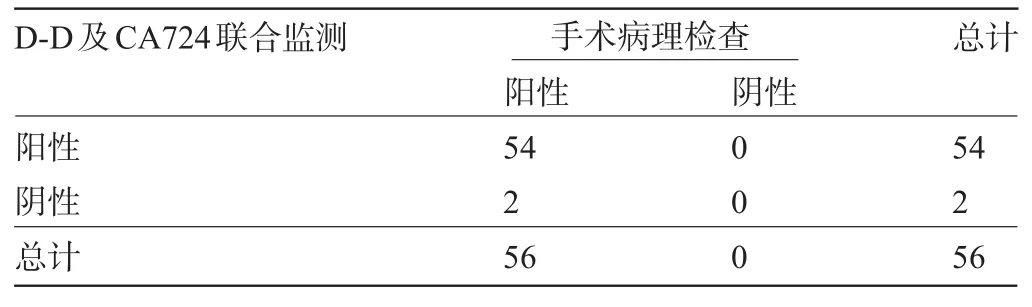
表6 胃癌患者D-D及CA724水平监测价值(例)
3 讨论
临床上,胃癌标志物主要用于辅助进行胃癌诊断或病情监测,以往使用较多的是CA125及CA199等指标。国外有报道指出,二者的敏感性及特异性仍不够理想[4]。近年来,临床发现,CA724可能对胃癌病情的反映效果更佳,而D-D水平亦逐渐受到人们关注。鉴于此,本文通过测定胃癌患者的外周血D-D及CA724水平,通过探索其临床意义以期为更好地监测并治疗胃癌患者提供数据参考支持。
CA724是高分子量的糖蛋白抗原,广泛存在于机体的胃部和结肠以及胰腺等肿瘤中,因此对于监测胃癌进展情况具有较大价值[5]。D-D是交朕纤维蛋白形成的一种特异性降解产物,其生成或者增高均反映出凝血及纤溶系统的激活,目前其应用巳深入至弥散型血管内凝血及心血管疾病亦或是恶性肿瘤等领域[6]。
本文经过研究发现,治疗前胃癌组及胃良性病变组的D-D及CA724水平均显著高于健康对照组,且胃癌组的D-D及CA724水平显著高于胃良性病变组;治疗后胃癌组的D-D及CA724水平显著高于健康对照组,而胃良性病变组的D-D及CA724水平与健康对照组相比,差异无统计学意义。提示D-D与CA724指标可较好地呈现胃部病变的严重情况[7]。同时,胃部病变尤其是胃癌患者经过治疗后,D-D及CA724水平均明显下降,这说明CA724及D-D指标水平含量变化可能与胃癌病变机制具有紧密联系,符合Lai等[8]的报道结果。此外,本文研究发现,胃癌浆膜层浸润的患者D-D及CA724水平均显著高于固有层及肌层浸润者,有淋巴结转移的患者D-D及CA724水平均显著高于无淋巴结转移者,低分化者D-D及CA724水平均显著高于中、高分化者。表明D-D及CA724水平均与癌症浸润情况和淋巴转移情况以及分化情况呈现出明显的相关联系[9],进一步将胃癌患者D-D及CA724水平升高作为因变量,将浆膜层浸润和有淋巴结转移,以及低分化作为自变量,实施Logistic回归分析发现,浆膜层浸润和有淋巴结转移,以及低分化均为胃癌患者D-D及CA724水平升高的相关因素。究其原因,笔者认为在浆膜层浸润及低分化方面,肿瘤组织朝器官外不断浸润的过程当中损伤了正常组织,随着分化程度的严重,发生一系列生化改变,进而导致D-D及CA724水平增高[10-11]。在有淋巴结转移方面,主要是因为癌症转移导致机体正常组织的破坏,而免疫细胞发挥作用时,在免疫反应的过程中影响了D-D与CA724的表达水平。唐菁等[12]亦报道指出,D-D及CA724联合检测对于胃癌疾病的鉴别价值较高。本文研究结果亦显示,CA724以6.90 U/mL为临界值时,单独CA724监测胃癌的敏感度、准确度均为83.93%,D-D以0.50 mg/L为临界值时,单独CA724监测胃癌的敏感度、准确度均为82.21%,当D-D及CA724联合监测时,其敏感度及准确度均为96.43%(54/56),提示D-D及CA724联合监测对于胃癌的诊断价值明显高于单独D-D及CA724监测,基本与之报道相符。
综上所述,为胃癌患者监测外周血D-D及CA724指标水平,可较好地反映其疾病情况,意义重大,值得临床推荐。
[1]高凤云,陶永明,郑嫦娟,等.肿瘤标志物联合检测在胃癌诊断及预后评估中的价值[J].肿瘤研究与临床,2014,26(3):183-186.
[2]Zou L,Qian J.Decline of serum CA724 as a probable predictive factor for tumor response during chemotherapy of advanced gastric carcinoma[J].Chin J Cancer Res,2014,26(4):404-409.
[3]史向军,黄新余,汪昱,等.胃液α1-抗胰蛋白酶、CEA、Ca199和Ca724检测在胃癌诊断中的价值[J].中国现代普通外科进展, 2014,17(9):737-739.
[4]Zhu Z,Chen Z,Chen C,et al.Opposite variation tendencies of serum CA724 levels in patients with colon and rectal carcinoma[J].Mol Clin Oncol,2014,2(1):139-145.
[5]付明生,潘淑贤,朱金水,等.血清胃蛋白酶原比值和CA724对胃癌的诊断价值及相关性分析[J].胃肠病学和肝病学杂志,2014,23 (3):256-258.
[6] Chen XZ,Zhang WK,Yang K,et al.Correlation between serum CA724 and gastric cancer:multiple analyses based on Chinese population[J].Mol Biol Rep,2012,39(9):9031-9039.
[7]朱剑峰,李志辉,朱红静,等.CEA、CA199、CA724、CA242、CA125、 CA50对消化道肿瘤的诊断价值[J].实用癌症杂志,2014,1(5): 501-502.
[8]Lai H,Jin Q,Lin Y,et al.Combined use of lysyl oxidase,carcino-embryonic antigen,and carbohydrate antigens improves the sensitivity of biomarkers in predicting lymph node metastasis and peritoneal metastasis in gastric cancer[J].Tumour Biol,2014,35(10): 10547-10654.
[9]高勇,李治国.血清肿瘤标志物在老年胰腺癌患者诊断中的应用[J].中华老年医学杂志,2013,32(8):840-842.
[10]Wang W,Li Y,Zhang X,et al.Evaluating the significance of expression of CEA mRNA and levels of CEA and its related proteins in colorectal cancer patients[J].J Surg Oncol,2014,109(5):440-444.
[11]孟庆松,李向东,李献忠,等.血清肿瘤标志及热休克蛋白60联合检测对胃癌早期诊断的价值[J].中华肿瘤防治杂志,2009,16(23): 1884-1886.
[12]唐菁,陈海霞,李笃军,等.CRP联合CEA、CA724检测对胃癌早期诊断及病情判断的临床应用价值[J].重庆医学,2013,42(1): 63-65.
Determination of peripheral blood D-dimmer and CA724 levels for patients with gastric cancer before and after surgery and its clinical significance.
PENG Fang-xing,YUAN San-ying,WU Chen,CHEN Jin,LUO Liang,CHEN Hui. Department of Gastrointestinal Surgery,the Mianyang No.404 Hospital of Sichuan,Mianyang 621000,Sichuan,CHINA
ObjectiveTo study the expression level of D-dimer(D-D)and carbohydrate antigen 724(CA724) before and after surgery and its clinical significance in peripheral blood of patients with gastric cancer.MethodsFifty-six patients of gastric cancer from January 2014 to March 2015 treated in our hospital were selected as the research subjects(gastric cancer group).Another 56 patients with benign gastric disease and 56 healthy subjects were included in the benign gastric disease group and healthy control group.D-D and CA724 level were compared between the three groups,and the relationship between pathological indexes of gastric cancer and D-D and CA724 levels were analyzed. The related factors of elevated D-D and CA724 levels in patients with gastric cancer were also analyzed.ResultsBefore treatment,D-D and CA724 levels in gastric cancer group and benign gastric disease group were significantly higher than those in healthy control group,and the D-D and CA724 levels in gastric cancer group were significantly higher than those in benign gastric disease group(P<0.05).After treatment,D-D and CA724 levels in gastric cancer group were significantly higher than those in healthy control group(P<0.05),while D-D and CA724 levels in benign gastric disease group showed no significant difference with those in health control group(P>0.05).D-D and CA724 levels in gastric cancer patients with serosa infiltration were significantly higher than those in patients with stroma and myometrial invasion,and the levels were also significantly higher in patients with lymph node metastasis than patients without lymph node metastasis and in patients with poor differentiation than patients with medium or high differentiation(all P<0.05). Taking elevated D-D and CA724 levels in gastric cancer patients as the dependent variable and the serosa invasion, lymph node metastasis,low differentiation as the independent variable,logistic regression analysis showed serosa invasion and lymph node metastasis,and low differentiation were the related factors of elevated D-D and CA724 levels in patients with gastric carcinoma differentiation(P<0.05).The sensitivity and accuracy of gastric cancer was 83.93%, 83.93%for CA724 alone(with CA724 of 6.90 U/mL as the critical value,)and 82.21%,82.21%for D-D alone(with0.50 mg/L as the critical value).For combined detection of D-D and CA724,the sensitivity and accuracy were 96.43% (54/56),96.43%(54/56),which were significantly higher than those for D-D or CA724 alone(χ2D-Dalone=5.973,χ2CA724alone= 4.940,P<0.05).ConclusionMonitoring of D-D and CA724 index in peripheral blood of patients with gastric carcinoma can reflect the disease situation,which is worthy of recommendation.
Gastric cancer;Peripheral blood;D-dimer;Carbohydrate antigen 724;Determination;Clinical significance
R735.2
A
1003—6350(2016)22—3648—04
10.3969/j.issn.1003-6350.2016.22.012
2016-06-13)
四川省教育厅科研项目(编号:12ZB062)
彭方兴。E-mail:pfx120@126.com
猜你喜欢
中老年保健(2022年6期)2022-08-19
清华金融评论(2022年4期)2022-04-13
现代临床医学(2021年4期)2021-07-31
现代畜牧科技(2021年4期)2021-07-21
内蒙古林业(2021年6期)2021-06-26
国际放射医学核医学杂志(2021年10期)2021-02-28
房地产导刊(2020年7期)2020-08-24
中国卫生(2016年9期)2016-11-12
中国继续医学教育(2015年1期)2016-01-06
医学研究杂志(2015年8期)2015-06-22
