
中-重型颅脑损伤患者血钠异常与损伤类型的相关性研究
2016-03-06 07:03:34李海蒙赵耀东侯典琦顾勤倪春明
海南医学 2016年5期
李海蒙,赵耀东,侯典琦,顾勤,倪春明
(1.上海健康医学院附属周浦医院神经外科,上海 201318;2.上海交通大学附属上海市第一人民医院神经外科,上海 200080)
中-重型颅脑损伤患者血钠异常与损伤类型的相关性研究
李海蒙1,赵耀东2,侯典琦2,顾勤1,倪春明1
(1.上海健康医学院附属周浦医院神经外科,上海 201318;2.上海交通大学附属上海市第一人民医院神经外科,上海 200080)
目的 探讨中-重型颅脑损伤患者的血钠异常与颅脑损伤类型之间的相关性。方法上海健康医学院附属周浦医院神经外科2014年3~12月收治中、重型颅脑损伤97例,根据CT表现,诊断为硬膜外血肿19例、硬膜下血肿28例、蛛网膜下腔出血27例、脑内血肿32例及弥漫性轴索损伤8例。所有患者在急诊室及入院后定期测量血钠,血钠<130 mmol/L或>145 mmol/L者为血钠异常。通过配对χ2检验,比较各类型颅脑损伤与血钠异常之间的相关性。结果97例患者中41例(42.3%)出现血钠异常,其中18例(18.6%)出现高钠血症,23例(23.7%)出现低钠血症;在各类型颅脑损伤的血钠异常中急性硬膜外血肿6例(26.3%),急性硬膜下血肿11例(39.3%),脑内血肿12例(44.4%),蛛网膜下腔出血14例(43.8%),弥漫性轴索损伤5例(62.5%),颅脑损伤的类型与血钠异常发生率之间比较差异无统计学意义(P>0.05)。结论血钠异常在中、重型颅脑损伤中发生率较高,但与颅脑损伤类型无相关性。在各类型中、重型颅脑损伤治疗过程中,应当早期和全程检测血钠水平,并及时纠正,有利于提高患者预后。
颅脑损伤;高钠血症;低钠血症;相关性
颅脑损伤患者的预后与伤后内环境稳定有着密切的关系。血钠异常是颅脑损伤后最常见的电解质紊乱的类型,它分为低钠血症及高钠血症。目前对两者在颅脑损伤后的发生机制了解并不确切,以往研究主要着眼于分析颅脑损伤后血钠异常的发生机制及治疗方法,而对不同类型颅脑损伤与血钠异常之间的关系研究甚少。本研究旨在探索中-重型颅脑损伤患者中血钠异常发生率及其与不同颅脑损伤类型之间的相关性。
1 资料与方法
1.1 一般资料 上海市周浦医院神经外科2014年3~12月共收治各型颅脑损伤患者457例,所有患者入院时进行神经系统检查、格拉斯哥昏迷评分(GCS),入院时及伤后8 h内均行头颅CT检查,并行颈部、胸腹部检查,所有患者均未使用高渗盐水治疗。排除标准:有肾功能不全、代谢性疾病、服用利尿剂等病史;胸腹脏器损伤及骨损伤(因常致血流动力学不稳,需晶体液抗休克治疗)。其中中型颅脑损伤86例,入院时GCS评分为9~13分;重型颅脑外伤40例,入院时GCS评分为3~8分。有8例患者因慢性肾功能不全或长期服用利尿剂而排除出组,有21例患者因合并严重胸腹外伤或长干骨、脊柱及骨盆骨折而被排除出组。共有97例患者入选本组研究,其中男性70例,女性27例;年龄8~78岁,平均42.4岁。
1.2 损伤分类 入院当时及伤后8 h、24 h及3 d进行CT检查,根据CT表现将颅脑损伤分为硬膜外血肿、硬膜下血肿、蛛网膜下腔出血、脑内血肿及弥漫性轴索损伤(DAI)。其中DAI的诊断标准为伤后持续昏迷大于6 h,伴有中线附近的局灶性小血肿。
1.3 实验室检查 所有患者血样采自上肢或下肢浅表静脉,患者在急诊室进行第一次采血。血钠异常标准<130 mmol/L或>145 mmol/L,入院后血钠异常者每日复查,血钠正常者每3 d复查一次。所有患者血钠至少随访至伤后3周。
1.4 治疗方法 患者出现高钠血症后均予禁钠,补充低渗或等渗液体治疗。严重高钠者,给予鼻饲大量白开水1 000~1 500 ml/d,以及改用白蛋白、速尿等利尿药物。低钠血症患者给予高渗盐水治疗,辅以限制入水量及糖皮质激素治疗。
1.5 统计学方法 应用SPSS19.0统计软件进行数据分析,计数资料比较采用χ2检验,以P<0.05为差异有统计学意义。
2 结 果
本组97例患者中48例行手术治疗,其中行开颅血肿清除术41例,行单纯颅内压探头置入术7例。共有41例(42.3%)患者出现血钠异常,其中18例(18.6%)患者出现高钠血症,23例(23.7%)患者出现低钠血症。在血钠异常患者中,15例(36.6%)患者在第一次采血时发现,23例(63.4%)患者在入院后复查血钠时发现。按损伤部位分类,19例次诊断为急性硬膜外血肿,6例次(31.6%)出现血钠异常;28例次诊断为急性硬膜下血肿,11例次(39.3%)出现血钠异常;27例次诊断为脑内血肿,12例次(44.4%)出现血钠异常;32例次诊断为蛛网膜下腔出血,14例次(43.8%)出现血钠异常;8例次诊断为弥漫性轴索损伤,5例次(62.5%)出现血钠异常。
在各类型颅脑损伤中,脑内血肿、蛛网膜下腔出血及弥漫性轴索损伤的血钠异常发生率较高,分别为44.4%、43.8%及62.5%。经χ2检验,不同类型颅脑损伤患者的血钠异常发生率比较差异均无统计学意义(P>0.05),见表1。
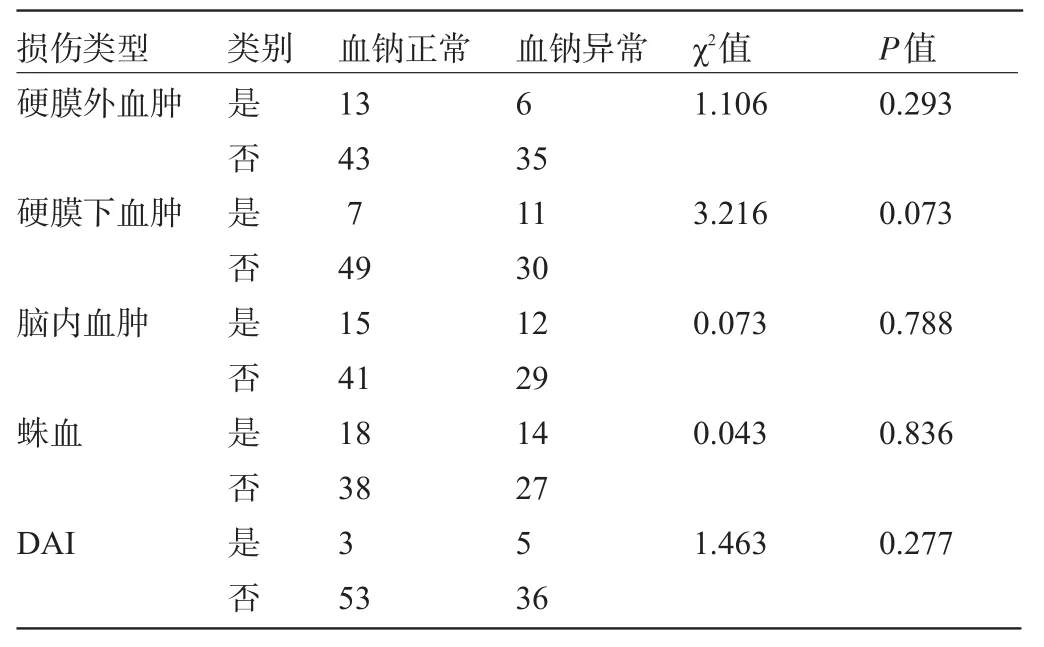
表1 不同损伤类型患者血钠异常情况(例次)
3 讨论
血钠异常在中重型颅脑损伤患者中较为常见,本组结果和文献报道相近[1-2]。各类型颅脑损伤间的血钠异常发生率差异无统计学意义,本组低钠血症发生率更高。下丘脑功能损害与血钠异常相关已成共识,但是下丘脑损害引起血钠异常的特点及机制尚未明了[3]。生理条件下机体通过复杂的神经内分泌调节实现水钠平衡,其中下丘脑的作用重大。下丘脑受损引起高钠血症的原因是位于下丘脑前部的渴觉中枢和(或)渗透压感受器受损而导致的渴觉减退性高钠血症。其机制是渴觉中枢和(或)渗透压感受器损伤,导致血浆渗透压的升高不能引起渴感饮水和(或)抗利尿激素(Antidiuretic hormone secretion,ADH)释放,表现为高血钠伴渴感减退或缺失。
目前认为脑性盐耗综合征(Cerebral salt wasing syndrome,CSWS)是中枢神经系统疾病合并低钠血症的一种常见的病理机制[4]。最新研究发现血浆脑尿钠肽(Brain natriuretic peptide,BNP)的分泌紊乱和脑性盐耗关系密切,BNP具有强有力的排钠、排尿和舒张血管的作用[5-6],它的增高最常见于在蛛网膜下腔出血、下丘脑出血及第三脑室出血的病例中[7-9]。Wijdicks等[10]证实BNP和SAH后尿钠排出增多引起的低血钠呈相关关系,后者认为下丘脑直接受损及下丘脑穿通血管痉挛或损伤引起下丘脑缺血性损害能够引起下丘脑释放BNP。由于检测条件受限,本研究没有检测ADH及BNP水平,无法分析血钠异常的可能机制,这需要进一步设计研究来完善。
据文献报道,与血钠正常的患者相比,颅脑损伤合并血钠异常的患者病死率较高[11-14]。严重的高钠血症会导致脑细胞水肿[12];严重的低钠血症会引起抽搐,导致昏迷、呼吸困难及脑干受压[11,13],二者均可导致严重后果。本研究证实血钠异常在中、重型颅脑损伤中发生率较高,各损伤类型之间发生率差异无统计学意义,因此在各类型中、重型颅脑损伤治疗过程中,应当早期和全程检测血钠水平,并及时纠正,有利于提高患者预后。
[1]Donati-Genet PC,Dubuis JM,Girardin E.Acute symptomatic hyponatremia and cerebral salt wasting after head injury:an importantclinical entity[J].J Pediatr Surg,2001,36(7):1094-1097.
[2]Paiva WS,Bezerra DA,Amorim RL,et al.Serum sodium disorders in patients with traumatic brain injury[J].Ther Clin Risk Manag, 2011,7:345-349.
[3]Sherlock M,O′Sullivan E,Agha A,et al.Incidence and pathophysiology of severe hyponatremia in neurosurgical patients[J].Postgrad Med J,2009,85(1002):171-175.
[4]Audibert G,Hoche J,Baumann A,et al.Water and electrolytes disorders after brain injury:mechanism and treatment[J].Ann Fr Anesth Reanim,2012,31(6):109-115.
[5]Ryu JH,Walcott BP,Kahle KT,et al.Induced and sustained hypernatremia for the prevention and treatment of cerebral edema following brain injury[J].Neurocrit Care,2013,19(2):222-231.
[6]Mukoyama M,Nakao K,Hosoda K,et al.Brain natriuretic peptide as a novel cardiac hormone in humans.Evidence for an exquisite dual natriuretic peptide system,atrial natriuretic peptide and brain natriuretic peptid[J].J Clin Invest,1991,87(4):1402-1412.
[7]John CA,Day MW.Central neurogenic diabetes insipidus,syndrome of inappropriate secretion of antidiuretic hormone,and cerebral salt-wasting syndrome in traumatic brain injury[J].Crit Care Nurse, 2012,32(2):1-7.
[8]Diringer MN,Lim JS,Kirch JR,et al.Suprasellar and intraventricular blood predict elevated plasma atrial natriuretic factor in subarachnoid hemorrhage[J].Stroke,1991,22(5):577-581.
[9]Tomida M.Muraki M,Uemura K,et a1.Plasma concentrations of brain natriuretie peptide in patientswith sbaraehnoid hemmzhage[J]. Stroke,1998,29(8):1584-1587.
[10]Wijdieks EFM,Schievink WI,Burnetjc JI.Natriuretiepeptide system and endothelin in aneurysmla subaraehnoid hemmzhage[J].J Neurosurg,1997,87(2):275-280.
[11]Carpenter J,Weinstein S,Myseros J et al.Inadvertent hyponatremia leading to acute cerebral edema and early evidence of herniation[J]. Neurocrit Care,2007,6(3):195-199.
[12]Harigan MR.Cerebral salt wasting syndmme[J].Crit Care Clin, 2001,17(1):125-138.
[13]Mizobata Y,Yokota J,Matsuoka T,et al.Volume supplementation with iso-sodium solution prevents hypernatremia after head injury [J].J Trauma,2001,50(5):871-877.
[14]Maggiore U,Picetti E,Antonucci E,et al.The relation between the incidence of hypernatremia and mortality in patients with severe traumatic brain injury[J].Crit Care,2009,13(4):R110.
Correlation between sodium disorders and different injury types in moderate and severe traumatic brain injuries.
LI Hai-meng1,ZHAO Yao-dong2,HOU Dian-qi2,GU Qin1,NI Chun-ming1.1.Department of Neurosurgery,Zhoupu Hospital Affiliated to Shanghai University of Medicine and Health Sciences,Shanghai 201318,CHINA;2.Department of Neurosurgery,Shanghai First People's Hospital Affiliated to Shanghai Jiao Tong University,Shanghai 200080,CHINA
ObjectiveTo determine the incidence of sodium disorders and its association with different injury types in patients with moderate and severe traumatic brain injuries(TBI).MethodsThis study was conducted in 97 patients diagnosed as moderate and severe TBI admitted in the Department of Neurosurgery,Zhoupu Hospital Affiliated to Shanghai University of Medicine and Health Sciences,including 19 cases of epidural hematoma,28 cases of subdural hematoma,27 cases of subaracnoid hemorrhage,32 cases of intracerebral hematoma and 8 cases of diffuse axonal injury. Serum sodium was detected in Emergency Department and at admission,and sodium disorders were considered as at least one serum sodium detection was<130 mmol/L or>145 mmol/L.Correlation between sodium disorders and different injury types were analyzed through chi-square test.ResultsAmong the 97 patients,41 showed sodium disorders, with the incidence of 42.3%,including 18 patients(18.6%)of hypernatremia and 23 patients(23.7%)of hyponatremia. Sodium disorders was found in 6 patients with epidural hematoma(26.3%),11 patients with subdural hematoma (39.3%),12 patients with intracerebral hematoma(44.4%),14 patients with subaracnoid hemorrhage(43.8%)and 5 patients with diffuse axonal injury(62.5%).The incidences of sodium disorders showed no significant difference between different injury types(P>0.05).ConclusionThe incidence of sodium disorders is high in moderate and severe TBI,but it has no correlation with injury types.We should pay attention to sodium level early and in the whole course in the treatment of TBI.
Brain injury;Hypernatremia;Hyponatremia;Correlation
R651.1+5
A
1003—6350(2016)05—0805—03
10.3969/j.issn.1003-6350.2016.05.041
2015-10-08)
国家自然科学基金(编号:81101909)
赵耀东。E-mail:zhaoyd@aliyun.com
猜你喜欢
中国卫生标准管理(2022年12期)2022-08-02 04:03:42
基础医学与临床(2022年7期)2022-07-11 02:19:04
临床肝胆病杂志(2020年5期)2020-12-20 13:50:12
中国医药指南(2019年5期)2019-03-22 00:36:04
山东医药(2016年17期)2016-09-05 09:28:45
中国医学创新(2015年28期)2015-12-30 13:38:10
中国当代医药(2015年22期)2015-03-01 02:05:30
河南医学研究(2014年2期)2014-02-27 14:51:33
卫生职业教育(2014年8期)2014-02-16 08:00:52
中国神经精神疾病杂志(2013年4期)2013-03-11 20:23:41
