宫外发育迟缓早产儿早期体格发育与IGF-I相关性分析*
2015-05-02 08:44:16葛晓风
贵州医科大学学报 2015年7期
葛晓风,王 鉴
(1.贵州医科大学 儿科教研室,贵州 贵阳 550004;2.贵州医科大学附院 儿科,贵州 贵阳 550004)
宫外发育迟缓早产儿早期体格发育与IGF-I相关性分析*
葛晓风1**,王 鉴1,2***
(1.贵州医科大学 儿科教研室,贵州 贵阳 550004;2.贵州医科大学附院 儿科,贵州 贵阳 550004)
目的: 探讨宫外发育迟缓(EUGR)早产儿的早期体格发育与胰岛素样生长因子(IGF-I)的关系。方法: 早产儿60例,分为EUGR组及非EUGR组,以同期收治的足月并正常出生的新生儿30例为对照组,所有新生儿于出生后7 d与2周时测量体格发育指标(体重、头围、身长),同时采集外周血测定血清中IGF-I水平;随访3月后测量2组早产儿体格发育指标,记录体重、身长及头围发育落后例数和计算体格发育指标增长情况,同时测定血清IGF-I水平,分析体格发育指标增长与IGF-I水平相关性。结果:早产儿7d、14d时体重、头围、身长、IGF-I水平均低于对照组(P<0.05), EUGR组早产儿7d、14d时体重较非EUGR组低(P<0.05);随访3月发现EUGR组早产儿体重、头围、身长及IGF-I水平低于非EUGR组(P<0.05),体重、身长及头围发育落后例数高于非EUGR组(P<0.01、P<0.01、P<0.05),体重增长速度、头围及身长增长均低于非EUGR组(P<0.05);EUGR组和非EUGR组IGF-I水平与体重增长速度、头围及身长增长均呈正相关(r=0.399、0.453、0.377、0.615、0.443、0.435,P<0.05)。结论:IGF-I水平变化与早产儿体格发育相关, EUGR早产儿更明显。
早产儿;宫外发育迟缓;早期体格发育;胰岛素样生长因子-I;发育
宫外生长发育迟缓(extrauterine growth retardation,EUGR)指早产儿出院时生长参数在同胎龄平均生长参数的第十个百分位以下[1]。EUGR发病率较高,除会影响早产儿近期体格发育外,还对远期健康有一定影响[2]。本研究对2014年4~10月收治的60例早产儿体格发育指标(体重、头围、身长)进行测量,同时检测血清胰岛素样生长因子-I (insulin-like growth factor-I,IGF-I)水平,分析2者的相关性,报告如下。
1 资料与方法
1.1 一般资料
2014年4~10月新生儿科收治的60例早产儿,按入院时体重分为EUGR组(31例)及非EUGR组(29例),并以同期收治的足月、正常出生体重高胆红素血症新生儿(排除感染、溶血病)为对照组(30例),三组患儿性别相比,差异无统计学意义(P>0.05)。排除标准:母亲患有甲状腺功能减退症、甲状腺功能亢进症、糖尿病等代谢性疾病,排除如先天性心脏病、食管闭锁、肠闭锁,两性畸形等先天性畸形、先天性遗传代谢疾病患儿。本研究经医院伦理委员会同意,所有对象家属签署知情同意书。
1.2 方法
将早产儿的出院体重按照胎龄或纠正胎龄与中国15个城市不同胎龄新生儿体重百分位数标准进行对照[3],以体重低于相应胎龄第十个百分位数作为判断EUGR或生长迟缓的标准。以早产儿出生后3月随访时测量体重、身长、头围,≤P10界定为体重、身长、头围发育落后。所有婴儿于生后第7天、2周及3月时抽取空腹外周静脉血2 mL,采用化学发光免疫分析法测定IGF-I水平,同时测量体格发育指标(体重、头围、身长),计算体重增长速度、头围增长、身长增长。日均体重增长,根据下公式进行计算:A=1 000×[(Wt′/Wt)1/n-1],A为日均体重增长速度[g/(kg·d)],Wt′为生后3月时体重(kg),Wt为出生体重(kg),n为天数(d)[4]。
1.3 观察指标
记录新生儿于出生后7 d与2周时体格发育指标(体重、头围、身长),同时采集外周血测定血清中IGF-I水平;记录出生 3月时早产儿体格发育指标、体重、身长及头围发育落后例数、计算体格发育指标增长情况(体重增长速度、头围增长、身长增长),同时测定血清IGF-I水平。
1.4 统计学分析
2 结果
2.1 一般资料
EUGR组和非EUGR组胎龄、住院时间比较差异无统计学意义(P>0.05),出生体重差异有统计学意义(P<0.05);见表1。
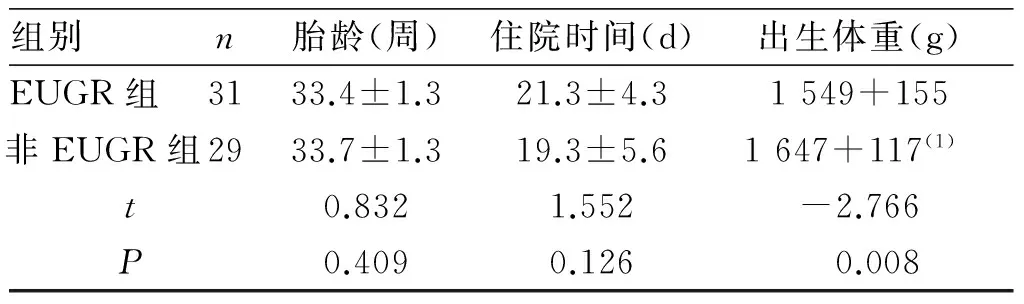
表1 两组早产儿胎龄、住院时间及出生体重比较Tab.1 Comparison of the gestational age, length of stay and birth weight between two group infants.
(1)与EUGR组比较,P<0.05
2.2 新生儿7d及14d时体格指标及IGF-I
EUGR组及非EUGR组在7 d、14 d时体重、头围、身长、IGF-I水平均低于对照组,差异有统计学意义(P<0.05);EUGR组7 d、14 d时体重较非EUGR组低,差异有统计学意义(P<0.05),而头围、身长及IGF-I水平比较,差异无统计学差异(P>0.05)。见表2。
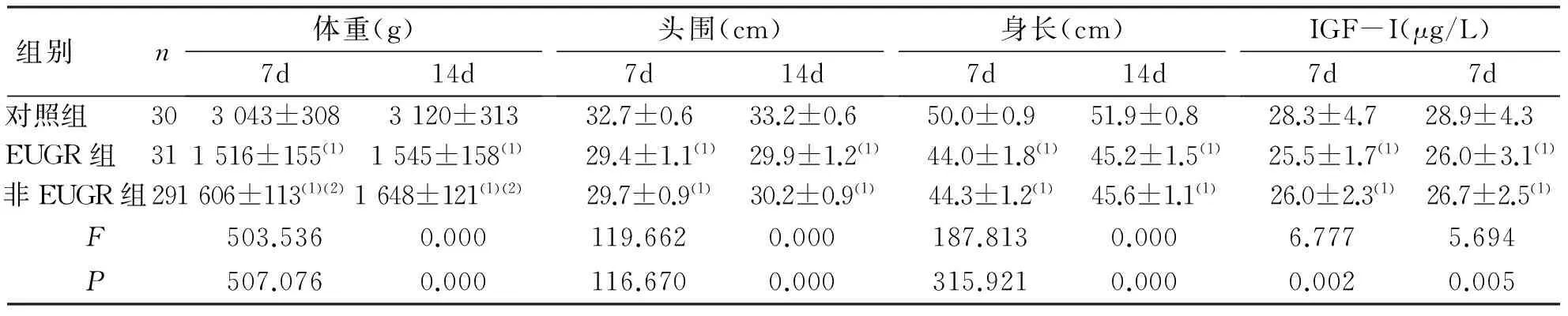
表2 3组新生儿出生7d及14d时体格指标及IGF-I比较Tab. 2 Comparison of physical development indexes and IGF-I level between the three groups at 7thday and 14thday
(1)与足月儿比较,P<0.05;(2)与EUGR组比较,P<0.05
2.3 两组早产儿生后3月时体格指标、IGF-I水平及发生体格发育落后情况
EUGR组早产儿在3月时体重、头围、身长及IGF-I水平明显低于非EUGR组早产儿,差异有统计学意义(P<0.05),见表3。EUGR组早产儿体重、身长及头围发育落后例数高于非EUGR组(P<0.01、P<0.01、P<0.05),见表4。

表3 两组早产儿出生3月时体格指标及IGF-I比较Tab. 3 Comparison of physical development indexes and IGF-I level between two groups at 90th day
(1)与EUGR组比较,P<0.01

表4 两组早产儿出生3月时体格发育落后情况Tab. 4 The physical development retardation situation of two groups at their 90th days
(1)与EUGR组比较,P<0.01,(2)P<0.05
2.4 两组早产儿的体格发育指标增长情况比较
EUGR组早产儿的体重增长速度、头围及身长增长均明显低于非EUGR组早产儿,差异有统计学意义(P<0.05)。见表5。
2.5 体格指标增长指标与IGF-I相关性
两组早产儿出生3月时体重增长速度、头围及身长增长与IGF-I呈正相关。见表6。

表5 两组早产儿出生3月时的体格发育指标Tab. 5 The physical development indexes of two group at their 90th day
(1)与EUGR组比较,P<0.01,(2)P<0.05
3 讨论
早产儿EUGR的主要临床表现以生长迟缓为主,在身长、头围、体重等方面受到明显影响。其中对体重的影响更为显著。IGF-I结构与胰岛素类似,是生长激素产生生理作用过程中必须的一种活性蛋白多肽物质,是胎儿及新生儿早期生长发育的重要调节因子[5]。IGF-I能刺激RNA、DNA的合成和细胞增殖,特别是对细胞的有丝分裂具有重大意义,其对骨、肌肉、脂肪组织、肝、肾及脑的生长都有重要作用[6]。在婴儿期IGF-I的分泌主要受营养因素及胰岛素的调控[7]。胎儿血IGF-I的水平随胎龄的增加而增加,并与胎儿的出生体重、身长呈正相关[8]。
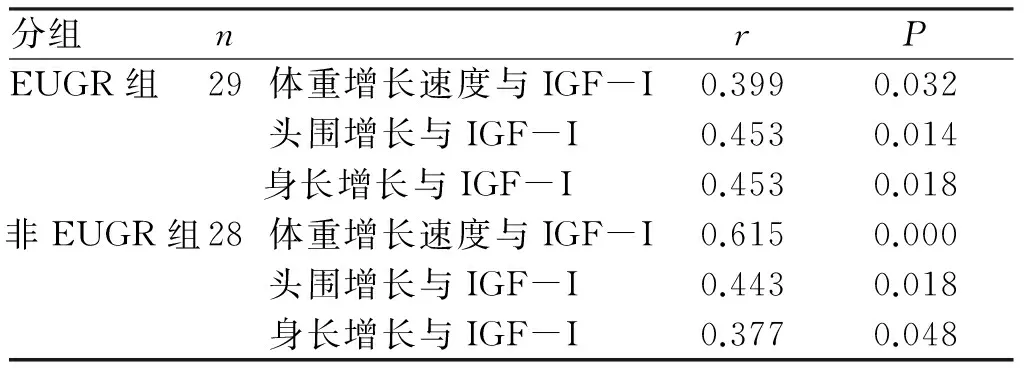
表6 两组早产儿出生3月时体格发育指标的增长与IGF-I相关性 Tab. 6 The correlation between physical development situation and IGF-I level at 90th day
本研究结果显示EUGR组及非EUGR组早产儿的体重及IGF-I的水平较足月儿低,可能与早产儿过早离开母体,缺乏母体来源的IGF-I及某些病理情况导致IGF-I进一步减少有关[9-11]。另母乳中含一定量的IGF-I,能经肠道吸收入血,早产儿因母亲疾病因素或自身疾病,母乳摄入量少,亦可导致IGF-I降低。本研究结果中EUGR组在7 d、14 d时体重低于非EUGR组(P<0.05),而身长、头围、IGF-I水平无差异(P>0.05),可能是EUGR多为非EUGR的延续,胎儿出生后适应环境能力更差,生理性体重下降后恢复时间更长所致。3月随访时,两组早产儿IGF-I水平较生后7 d、14 d时明显升高,提示IGF-I在生后3月内有随早产儿年龄增长而升高的趋势,说明随着机体的发育,病理状态的解除,营养的摄入增加,且生长激素-胰岛素样生长因子-I(GH-IGF-I)轴发育逐渐成熟,IGF-I水平逐渐升高。与非EUGR组早产儿相比,EUGR组早产儿IGF-I较低,同时在体重增长速度、身长及头围增长方面EUGR组均低于非EUGR组(P<0.05),且IGF-I与体重增长速度、头围及身长增长呈正相关,进一步证实IGF-I是调节生长发育速度的重要因子,在婴幼儿生长发育中起着重要的作用。而EUGR组早产儿发生生长落后的例数明显高于非EUGR组,这可能与EUGR组早产儿易发生风险性疾病,累积的能量、蛋白质及矿物质的缺失较非EUGR组更为显著,导致短期内EUGR早产儿追赶生长速度低于非EUGR早产儿有关,提示IGF-I水平可作为反映体格发育的指标。
综上,IGF-I水平变化与早产儿体格发育相关,EUGR早产儿更明显。提示对于早产儿特别是EUGR早产儿出生后应给予合理科学的喂养以保证营养摄入,尤其是母乳喂养,提高IGF-I的水平,减少早产儿生长发育落后的发生。
[1] Clark RH,Thomas P,Peabody J.Extrauterine growth restriction remains a serious problem in prematurely bornneonates[J].Pediatrics,2003(5):986-990.
[2] 陈文,廖翎帆,李秋红,等.早产儿及足月儿蛋白质水平差异的研究[J].重庆医学,2010,(13):1707-1708.
[3] Fenton TR,Kim JH.A systematic review and meta-analysis to revise the Fenton growth chart for perterm infants[J].BMC Pediatr,2003(3):13.
[4] 吴繁,崔其亮,张慧,等.极低出生体重儿院内生长发育状态多中心回顾性研究[J].中华儿科杂志,2013(51):4-11.
[5] Castell AL,Sadoul JL,Bouvattier C. Growth hormone-insulin growth factor I (GH-IGF-I) axis and growth [J].Ann Endocrinol (Paris),2013(Suppl 1):33-41.
[6] Klover P,Hennighausen L.Postnatal body growth is dependent on thetranscription factors signal I ransducers and activators of transcription 5a/b in muscle:A role for autocrine/paracrine isulin-like growth factorq[J].Endocrinology,2007(4):1489-1497.
[7] Laron Z.Insulin-like growth for 1(IGF-I):a growth hormone[J].Mol Pathol,2001(5):311-316.
[8] 卢燕玲.生长素、瘦素及胰岛素样生长因子-I在小于胎龄儿生长追赶中的作用[J].中国现代医药杂志,2013(3):30-32.
[9] Engstom E,Niklasson A,Wikland KA,et al.The role of maternal factors,postnatal nutrition,weight gain,and gen-der in regulation of serum IGF-I among preterm infants[J].Pediatr Res,2005(4):605-610.
[10]Lo HC,Tsao LY,Hsu WY,et al.Changes in sernm in.sulin-like growth factors,not leptin,are associated with postnatal weight gain in preterm neonates[J].JPEN JParenter Enteral Nutr,2005(2):87-92.
[11]Gronbek H,Th ogersen T,Frystyk J,et al.Low free and total insulin-like growth factor I (IGF-I) and IGF bin-ding protein-3 levels in chronic inflammatory bowel disease:partial normalization during prednisolone treatment[J].Am J Gastroenterol,2002(3):673-678.
(2015-04-02收稿,2015-06-03修回)
中文编辑: 吴昌学; 英文编辑: 刘 华
Analysis of Relevance between Physical Development of Premature Infants with Extrauterine Growth Retardation and IGF-I
GE Xiaofeng1,WANG Jian1,2
(DepartmentofPediatric,GuizhouMedicalUniversity,Guiyang550004,Guizhou,China;DepartmentofPediatric,AffiliatedHospitalofGuizhouMedicalUniversity,Guiyang550004,Guizhou,China)
Objective: To investigate the relationship between early-stage physical development of premature infants with extrauterine growth retardation and IGF-I level. Methods: Sixty premature infants were divided into extrauterine growth retardation group (EUGR group, 31 cases) and non extrauterine growth retardation group (non-EUGR group, 29 cases), meanwhile 30 full-term normal infants hospitalized during the same period were selected as control group. The physical development indexes(weight, head circumference, height) were measured 7 days and 14 days after birth. Meanwhile, the peripheral blood was collected and the IGF-I level of serum was determined. 3 months after birth, the physical development indexes of premature infants in 2 groups were measured again, the retardation cases were recorded in terms of weight, head circumference and height and the growth of physical development index were calculated. Meanwhile, the IGF-I level of serum was determined and the relevance between growth of physical development indexes and IGF-I level was analyzed. Results: The weight, head circumference, height and IGF-I level of premature group infants were lower than their counterparts of full-term infants on their 7thday, 14thday after birth.(P<0.05). The weight of EUGR group was lower than that of non-EUGR group on their 7thday, 14thday after birth (P<0.05). The weight, head circumference, height and IGF-I level of EUGR group were significantly lower than their counterparts of non-EUGR group on their 90thday(P<0.05). The growth rate of weight, head circumference and height of EUGR group were lower than those of non EUGR group. There was a positive correlation between IGF-I level and development speed of weight, head circumference, height(r=0.399, 0.453, 0.377, 0.615, 0.443, 0.435,P<0.05). Conclusion: IGF-I level is relevant to physical development of EUGR premature infants.
premature infant;extrauterine growth retardation;early physical development;insulin-like growth factor-I;development
贵州省科技厅科学技术基金[黔科合J字(2009)2160号]
时间:2015-7-1
http://www.cnki.net/kcms/detail/52.5012.R.20150701.2010.019.html
R722.6
A
1000-2707(2015)07-0730-04
**贵阳医学院2012级硕士研究生
***通信作者 E-mail:378314357@qq.com
猜你喜欢
中华养生保健(2020年10期)2021-01-18 06:46:06
当代水产(2019年11期)2019-12-23 09:03:04
参花·青春文学(2019年2期)2019-09-10 07:22:44
中国生物医学工程学报(2019年4期)2019-07-16 08:04:04
恋爱婚姻家庭·青春(2019年1期)2019-01-25 01:34:46
中国实用医药(2016年12期)2016-05-04 12:03:12
食品与健康(2014年7期)2014-08-15 09:21:23
筑路机械与施工机械化(2014年8期)2014-03-01 03:01:27
学与玩(2009年5期)2009-07-14 09:54:42
学与玩(2009年2期)2009-03-09 04:05:42