双极电凝镊与超声吸引刀在肝叶切除术中应用的对照研究
2014-12-05 06:36:12曹东亮
成都医学院学报 2014年5期
程 瑜,孙 云,曹东亮
1.重庆医科大学附属大学城医院 手术麻醉科(重庆 401331);2.成都医学院第一附属医院(成都 610500);3.成都医学院检验医学院(成都 610500)
超声吸引刀(cavitron ultrasonic surgical aspirator,CUSA)是20世 纪90年代问世的一种兼有凝固和切割功能的新型手术器械,在一定程度上促进了肝脏外科技术的发展,为精细肝脏外科的形成提供了一个可靠平台。很多临床研究[1-3]中,CUSA在切割、止血方面确实具有传统手术方法无可比拟的优势,被证明可以减少术中出血。但CUSA刀头较粗大、切割时间长等固有的局限性也不可忽视。双极电凝镊(bipolar coagulation forceps,BC)对于细小血管具有很好的凝闭止血功能,且其镊电极很细,非常适合离断处理肝脏[4-7]。本研究旨在对CUSA与BC行肝叶切除手术进行比较,为该手术技术应用推广提供理论依据,现报道如下。
1 资料与方法
1.1 临床资料
选取2010年7月~2012年7月肝叶切除术手术患者68例为研究对象。其中,采用BC行肝叶切除术的患者32例为A组;采用CUSA行肝叶切除术的患者36例为B组。纳入标准:1)病灶位于肝脏一叶,不累及第一、第二肝门及下腔静脉;2)良性肿瘤直径<15cm,恶性肿瘤<10cm;3)不合并有门静脉主干癌栓,无肝内转移及远处转移;4)无心、肺、肝、肾等重要脏器功能和凝血功能障碍。排除标准:手术中行肝三叶、肝中叶切除病例;肝硬化失代偿期;腹腔镜中转开腹病例;病灶累及肝门、下腔静脉,肿瘤较大,直径>15cm。由于瘤体大,翻动暴露困难,即使勉强切除,也难免在操作中弄破肿瘤;有上腹腔手术史、腹腔黏连严重等相对禁忌症。
1.2 手术方法
采用强生公司生产的超声切割止血系统,刀头型号为Focus,刀头宽度2mm。采用ValleyBC,镊尖直径0.6mm。A组及B组均由同一主刀医生行肝叶切除术。
手术在全麻下,取右上腹反L形切口进腹,解剖肝门,充分游离半肝,根据术前检查准确判断病肝部位、肝癌侵及范围、胆管狭窄、结石分布范围及术中所见肝脏纤维化范围,切除相应肝叶,切肝时术者将肝脏切除线健侧肝组织握于手中,这样可明显减少术中出血量;A组和B组分别用BC和CUSA分离肝实质,逐渐由浅层向肝实质深部分离,2mm以上血管则需结扎止血,两组均阻断肝门或肝脏血管分支血流,主要脉管配合钳夹、结扎、切断、缝扎,移除病肝,肝断面胆管用丝线和prolene线间断缝闭,再用网膜包被,肝断面置管引流以便于术后观察出血情况[7,8]。
1.3 观测指标
观察并比较A组和B组术前年龄、性别比例、肝功能Child-Pough分级评分、肝储备功能评分(ICG score)、肝硬化比例[9,10]、手术时间、术中出血量、术中输血量以及不同器械离断肝脏对手术的影响。评估两组患者术后恢复情况,包括术后3d谷丙转氨酶比较、是否并发腹腔感染、是否合并胆漏、术后监护室恢复时间和术后住院时间。评估两种不同方法对患者恢复的影响。
1.4 统计学方法
采用SPSS 13.0软件对所得数据进行分析,计量资料采用均数±标准差(±s)表示,组间比较采用独立样本t检验,率的比较采用χ2检验,以P<0.05为差异有统计学意义。
2 结果
2.1 两组患者术前基本参数比较
比较两组术前年龄、肝功能Child-Pough分级评分、ICG score、性别比例和肝硬化比例,结果提示,两组患者术前基本参数比较,差异无统计学意义(见表1)。

表1 两组患者术前基本参数比较
2.2 两组患者术中参数比较
两组行肝叶切除术中失血量和术中输血量比较,差异无统计学意义;但手术时间A组短于B组,差异有统计学意义(P<0.05)(见表2)。
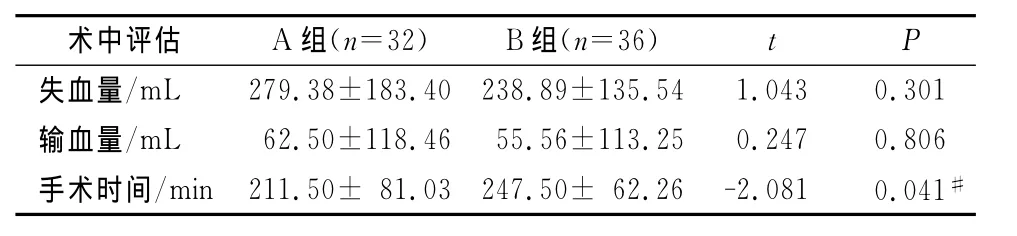
表2 术中参数的比较
2.3 两组患者术后恢复比较
两组患者术后恢复各项指标包括术后3d谷丙转氨酶以及是否并发腹腔感染、是否合并胆漏、术后监护室恢复时间和术后住院时间比较,差异无统计学意义(见表3)。
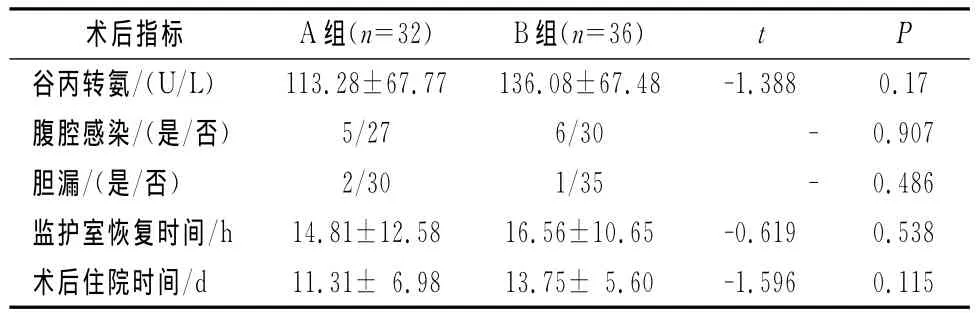
表3 术后恢复情况
3 讨论
目前切断肝脏组织的工具有许多,如高频电刀、水喷刀、微波刀、直线切割闭合器、BC以及CUSA等。CUSA原理是将电能转换为机械能,使金属探头产生超声频率的机械震荡带动组织振动继而使组织水汽化,蛋白氢键断裂分解重组使细胞内蛋白变性形成凝块从而形成胶状封闭血管达到止血效果[11-14]。使用BC时,从镊子的一端有电流发出,经夹持的组织通过镊子另一端回流到主机,低密度电流使组织脱水,蛋白凝固,血管、胆管皱缩;另一方面,在电凝过程中产热使血管内蛋白质变性、变稠,导致血液凝固,达到止血目的[4,15,16]。
本研究术前评估中ICG score即吲哚氰绿排泄实验,采用患者注射吲哚氰绿15min后的储留率[17-19],该指标和 Child-Pough分级评分综合可全面反应患者肝脏功能[20,21]。本研究结果提示,两组术前年龄、性别比例、肝硬化比例、肝功能Child-Pough分级评分和ICG score比较,差异无统计学意义。
两组手术中均出血量少,仅少数患者需输血,故平均输血量较少,但手术时间A组短于B组(P<0.05),可能是由于BC对细小血管可以直接止血,节约了部分时间。而两组术后恢复情况比较,差异无统计学意义。
BC具有止血效果确切、操作简单和购置价格便宜等优点,但BC在操作时产生的烟雾是其至今仍然不能克服的弊端,导致术野不够清晰,如果电凝的组织未完全干燥则导致凝固不全,止血不确切。因此,术后仍需密切观察生命体征及腹腔引流量[22-26]。
综上所述,运用BC是肝叶切除术一种实用且有效的技术,这种止血方法具有设备易得、操作简单、省时省力、效果确实和并发症少等优点,值得临床推广。
[1]Bodzin AS,Leiby BE,Ramirez CG,etal.Liver resection using cavitron ultrasonic surgical aspirator(CUSA)versus harmonic scalpel:a retrospective cohort study[J].Int J Surg,2014,12(5):500-503.
[2]Lee JH,Kwon TD,Kim HJ,etal.Multiple cerebral infarction and paradoxical air embolism during hepatectomy using the Cavitron Ultrasonic Surgical Aspirator-A case report[J].Korean J Anesthesiol,2010,59:133-136.
[3]J SH,Muirhead W,Zaitoun AM,etal.Comparison of liver parenchymal ablation and tissue necrosis in a cadaveric bovine model using the Harmonic Scalpel,the LigaSure,the Cavitron Ultrasonic Surgical Aspirator and the Aquamantys devices[J].HPB:Oxford,2012,14(12):828-832.
[4]Mulier S,Jiang Y,Wang C,etal.Bipolar radiofrequency ablation with four electrodes:ex vivo liver experiments and finite element method analysis.Influence of inter-electrode distance on coagulation size and geometry [J].Int J Hyperthermia,2012,28(7):686-697.
[5]Abouljoud MS,Arenas J,Yoshida A,etal.New application of the bipolar vapor plasma coagulation system for laparoscopic major liver resections[J].Surg Endosc,2008,22(2):426-429.
[6]Clasen S,Schmidt D,Dietz K,etal.Bipolar radiofrequency ablation using internally cooled electrodes in ex vivo bovine liver:prediction of coagulation volume from applied energy[J].Invest Radiol,2007,42(1):29-36.
[7]Corvera CU,Dada SA,Kirkland JG,etal.Bipolar pulse coagulation for resection of the cirrhotic liver[J].J Surg Res,2006,136(2):182-186.
[8]Tan J,Hunt A,Wijesuriya R,etal.Gyrus PlasmaKinetic bipolar coagulation device for liver resection[J].ANZ J Surg,2010,80(3):182-185.
[9]Vos JJ,Scheeren TW,Lukes DJ,etal.Intraoperative ICG plasma disappearance rate helps to predict absence of early postoperative complications after orthotopic liver transplantation[J].J Clin Monit Comput,2013,27(5):591-598.
[10]Li H,Li B,Wei Y.Potential factors dedicated to postoperative liver dysfunction in patients with normal preoperative ICG-15 clearance rate[J].Dig Dis Sci,2013,58(4):1163-1164.
[11]El Moghazy WM,Hedaya MS,Kaido T,etal.Two different methods for donor hepatic transection:cavitron ultrasonic surgical aspirator with bipolar cautery versus cavitron ultrasonic surgical aspirator with radiofrequency coagulator-A randomized controlled trial[J].Liver Transpl,2009,15(1):102-105.
[12]Carrabba G,Mandonnet E,Fava E,etal.Transient inhibition of motor function induced by the Cavitron ultrasonic surgical aspirator during brain mapping[J].Neurosurgery,2008,63(1):178-179.
[13]Branco BC,Sachar DB,Heimann T,etal.Adenocarcinoma complicating restorative proctocolectomy for ulcerative colitis with mucosectomy performed by Cavitron Ultrasonic Surgical Aspirator[J].Colorectal Dis,2009,11(4):428-429.
[14]Ozawa T,Nose K,Harada T,etal.Treatment of osmidrosis with the Cavitron ultrasonic surgical aspirator[J].Dermatol Surg,2006,32(10):1251-1255.
[15]Gonzalez-Suarez A,Trujillo M,Burdio F,etal.Feasibility study of an internally cooled bipolar applicator for RF coagulation of hepatic tissue:experimental and computational study[J].Int J Hyperthermia,2012,28(7):663-673.
[16]Lanna MM,Rustico MA,Dell'Avanzo M,etal.Bipolar cord coagulation for selective feticide in complicated monochorionic twin pregnancies:118consecutive cases at a single center[J].Ultrasound Obstet Gynecol,2012,39(4):407-413.
[17]Merkel C,Gatta A,Zoli M,etal.Prognostic value of galactose elimination capacity,aminopyrine breath test,and ICG clearance in patients with cirrhosis.Comparison with the Pugh Score[J].Dig Dis Sci,1991,36(9):1197-1203.
[18]Mizuno S,Isaji S.Indocyanine green(ICG)fluorescence imaging-guided cholangiography for donor hepatectomy in living donor liver transplantation[J].Am J Transplant,2010,10(12):2725-2726.
[19]Zipprich A,Kuss O,Rogowski S,etal.Incorporating indocyanin green clearance into the Model for End Stage Liver Disease(MELD-ICG)improves prognostic accuracy in intermediate to advanced cirrhosis[J].Gut,2010,59(7):963-968.
[20]Jeong JY,Sohn JH,Son BK,etal.Comparison of model for end-stage liver disease score with discriminant function and child-Turcotte-Pugh scores for predicting short-term mortality in Korean patients with alcoholic hepatitis[J].Korean J Gastroenterol,2007,49(2):93-99.
[21]Liu YX,Huang LY,Wu CR,etal.Measurement of liver function for patients with cirrhosis by 13C-methacetin breath test compared with Child-Pugh score and routine liver function tests[J].Chin Med J:Engl,2006,119(18):1563-1566.
[22]Cui Z,Luan G,Zhou J.Pure bipolar electro-coagulation on functional cortex in the treatment of epilepsy involving eloquent areas[J].Epilepsy Res,2012,99(1-2):139-146.
[23]Carus T,Rackebrandt K.Collateral tissue damage by several types of coagulation(monopolar,bipolar,cold plasma and ultrasonic)in a minimally invasive,perfused liver model[J].ISRN Surg,2011,2011:518924.
[24]Lenz L,Tafarel J,Correia L,etal.Comparative study of bipolar eletrocoagulation versus argon plasma coagulation for rectal bleeding due to chronic radiation coloproctopathy[J].Endoscopy,2011,43(8):697-701.
[25]Chen RK,Than KD,Wang AC,etal.Comparison of thermal coagulation profiles for bipolar forceps with different cooling mechanisms in a porcine model of spinal surgery[J].Surg Neurol Int,2013,4:113.
[26]Chen RK,Than KD,Park P,etal.Thermoelectrical modeling of bipolar coagulation on posterior spinal artery in a porcine spinal surgery model[J].IEEE Trans Biomed Eng,2014,61(1):182-188.
猜你喜欢
传染病信息(2022年6期)2023-01-12 08:59:04
昆明医科大学学报(2021年10期)2021-12-02 03:24:26
现代临床医学(2021年5期)2021-11-02 05:20:44
昆明医科大学学报(2021年4期)2021-07-23 01:22:12
中国临床医学影像杂志(2019年1期)2019-04-25 06:49:38
中国继续医学教育(2016年19期)2016-02-15 13:14:05
中国现代药物应用(2016年17期)2016-01-26 14:35:54
医学研究杂志(2015年5期)2015-06-10 06:43:26
中国当代医药(2015年26期)2015-03-01 02:06:57
肝胆胰外科杂志(2015年4期)2015-02-27 11:12:35