
The effectof shoe type on gait in forefootstrike runners during a 50-km run
2014-03-21 02:33MrkKsmerNicholsKetchumXueChengLiu
Mrk E.Ksmer,Nichols C.Ketchum,Xue-Cheng Liu
aDepartment of Physical Medicine and Rehabilitation,Medical College of Wisconsin,M ilwaukee,WI 53226,USA
bDepartmentof Orthopedic Surgery,Medical College of Wisconsin,Milwaukee,WI 53226,USA
The effectof shoe type on gait in forefootstrike runners during a 50-km run
Mark E.Kasmera,*,Nicholas C.Ketchuma,Xue-Cheng Liub
aDepartment of Physical Medicine and Rehabilitation,Medical College of Wisconsin,M ilwaukee,WI 53226,USA
bDepartmentof Orthopedic Surgery,Medical College of Wisconsin,Milwaukee,WI 53226,USA
Purpose:To observe the relative change in foot-strike pattern,pressure characteristics,surface electromyography(sEMG)recordings,and stride characteristics in forefoot strike runners wearing both m inimalist and traditional shoes during a 50-km run.
Methods:Four experienced m inimalist runners were enrolled in this study.Each runner ran a 50-km simulated run in both m inimalistshoes and traditional shoes.Pressure data,sEMG recordings,and lim ited 3D motion capture data were collected during the initial0.8 km and final0.8 km for each trial.
Results:Three runners in the traditionalshoe type condition and one runner in the m inimalistshoe type condition demonstrated a more posterior initial contact area(m idfootstrike(MFS)pattern)after the 50-km run,which was supported by increased activity of the tibialis anterior in the pre-contactphase(as per rootmean square(RMS)values).In addition,in both pre-and post-run conditions,there were increased peak pressures in the m inimalist shoe type,specifically in the medial forefoot.Muscle fatigue as defined by a decreased median frequency observed in isometric,constant force contractions did notcorrespond w ith our hypothesis in relation to the observed footstrike change pattern.Finally,step rate increased and step length decreased after the 50-km run in both shoe type conditions.
Conclusion:More runners adopted a more posterior initial contact area after the 50-km run in the traditional shoe type than in the m inimalist shoe type.The runners who adopted a more posterior initialcontactarea were more closely associated w ith an increased median frequency of the medialgastrocnemius,which suggests there may be a change in motorunit recruitmentpattern during long-distance,sustained velocity running. The increased peak pressures observed in the medial forefoot in the m inimalist shoe type may predispose to metatarsal stress fractures in the setting of improper training.
CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved.
Endurance;Fatigue;Foot-strike pattern;Running;Surface electromyography(sEMG)
1.Introduction
In 1989,Robbins etal.1suggested that runners may modify running form based on“impact moderating behavior(s)”.In 2010,Lieberman et al.2observed an impact transient,or sudden force of loading at initial contact,among different foot-strike patterns and shod conditions.The reduction of this impact transient in barefoot runners,as well as“m inimalist”runners in Vibram Five Fingers,through adaptation of footstrike pattern has been previously observed by Squadrone and Gallozzi,3as well as Divert et al.4In addition to a more forefoot strike(FFS)pattern,barefoot or m inimalist runners have demonstrated reduced stride length,increased stride rate (or frequency),and decreased contact time.3—6In studies in which barefoot or minimalist runners did not alter foot-strike pattern,whether by instruction5,7or significant cushioning of the“m inimalist”shoe,6this same reduction of impact transient has not been observed.
Aside from barefoot and m inimalist runners,another population theorized to benefi t from a reduction of impact force are long-distance runners.8Laboratory studies,through the implementation of varying fatigue protocols,as well as“in-race”studies,have investigated this theory,mostofwhich have suggested that impact force decreases w ith fatigue. Gerlach et al.9and W illson and Kernozek10have demonstrated a reduction in peak force,peak loading rate,peak pressure and pressure time integral under the heel after completion ofa fatigue protocol.These findings are sim ilar to the study ofMorin etal.11during a 24-h treadm illprotocol,as well as M illet et al.12during an 8500-km run by one runner over 161 days(52.8 km/day).Both“in-race”studies to date, which have been completed in marathon runners,13as wellas ultramarathon runners,14have demonstrated a reduction in impact force.
Possible explanations for the reduction of impact force observed in long-distance runners after fatigue include change in foot-strike pattern and change in stride characteristics. Change in foot-strike pattern during race conditions has been studied previously in a marathon by Larson et al.15and an ultramarathon by Kasmeretal.16In both studies,more runners utilized a rearfoot strike(RFS)pattern near the m iddle or end of the race than at the beginning,suggesting that these longdistance runners were more likely to adopt an RFS pattern w ith presumed muscle fatigue.In the study by Kasmeretal.,16non-RFS runners were associated with an increased blood creatinine phosphokinase(CPK)level compared to RFS runners,suggesting that the change in foot-strike pattern from non-RFS to rear foot-strike may be influenced by muscle fatigue of the plantar flexors associated w ith non-rearfoot striking.Based on the study of Lieberman et al.,2who observed a greater impact transient w ith an RFS,this footstrike change pattern would not support a decrease in impact force.
Change in stride characteristics follow ing fatigue has likew ise been studied.The majority of studies have suggested that step rate increases w ith fatigue while step length decreases w ith fatigue,as demonstrated by Willson and Kernozek10after a fatigue protocol,by Kyrolainen et al.17and Haussw irth etal.18after a marathon run,and by Morin etal.11after a 24-h treadm ill run.The runner in the study by M illet et al.12also increased step rate after 161 days and approximately 8500 km.However,in contrast to these studies, Gerlach et al.9observed a decreased step rate and increased step length after a fatigue protocol,and Kasmer et al.16observed a decreased step rate and step length at the 90.3 km mark of a 161-km run.In the study by Kasmeretal.,16the authors also observed an increased number of“shufflers”, defined by runners observed to be lacking the double float phase,at the 90.3 km fi lm ing site.The authors speculate thata decrease in step length w ith or without the incorporation of this“shuffl ing”pattern may reduce the impact force.
To the authors’know ledge,no study has attempted to analyze kinetic characteristics or stride characteristics in the combined setting,i.e.,barefoot or m inimalist runners after a long-distance run.This study attempted to fi ll this void by analyzing the kinetic and stride characteristics of runners in m inimalist,as well as traditional shoes,both at the beginning and end of a 50-km run.
We hypothesized that experienced m inimalist runners would transition from an FFS pattern to a more posterior footstrike pattern due to plantar flexor muscle fatigue or damage, as previously demonstrated by significantly higher blood CPK values among non-RFS runners compared to RFS runners during an ultramarathon,16thus increasing the peak pressure over the heel in both shoe types.Furthermore,we predicted that surface electromyography(sEMG)recordings would demonstrate evidence of fatigue in the plantar flexors,associated w ith increased work w ith FFS,supportive of the transition to a more posterior foot-strike pattern.Finally,we hypothesized that stride rate would increase and stride length decrease during the run.
Therefore,the main objectives of this study are to(1) determ ine the relative change in foot-strike pattern and pressure characteristics in runners wearing both m inimalist and traditional shoes after a 50-km run;(2)determ ine if sEMG demonstrates a fatigue pattern thatcorresponds to the observed change in foot-strike pattern in both shoe type conditions;and (3)determ ine the change in stride characteristics in runners wearing both m inimalist and traditional shoes after a 50-km run.
2.M aterials and methods
2.1.Participants
Four participants were successfully recruited for this study. Each participantmetall inclusion/exclusion criteria:male<45 years old or female<55 years old;American College of Sports Medicine(ACSM)criteria for low-risk classification for coronary artery disease(CAD)19based on questions from participant’s pre-protocol questionnaire;asymptomatic for cardiovascular/pulmonary disease;at least 1 year experience primarily running in m inimalistshoes;run greater than 50-km in m inimalist shoes w ithin the past 12 months or run greater than 64.4 km(40 m iles)per week and have the ability to run 50 km at 2.7 m/s;no injuries w ithin the past 1 year as defined by medical treatmentor stoppage of training for greater than 1 week due to injury;no current injury;and have the ability to follow study protocol,including the ability to wear the dynam ic measuring system insoles.The study was approved by the institutional review board at Medical College of W isconsin and each participant provided informed consent prior to enrollment in the study.
2.2.Data collection
Prior to data collection,each runner completed a questionnaire,including demographic information,running history, and injury history(Table 1).Participants were then randomized to either the m inimalist shoe(New Balance M inimus Zero Trail;New Balance,Boston,MA,USA),w ith a heel-toe drop of zero m illimeters,or traditional shoe(per runnerpreference)and were instructed to train for 4 weeks solely in the assigned shoe type prior to the initial data collection.
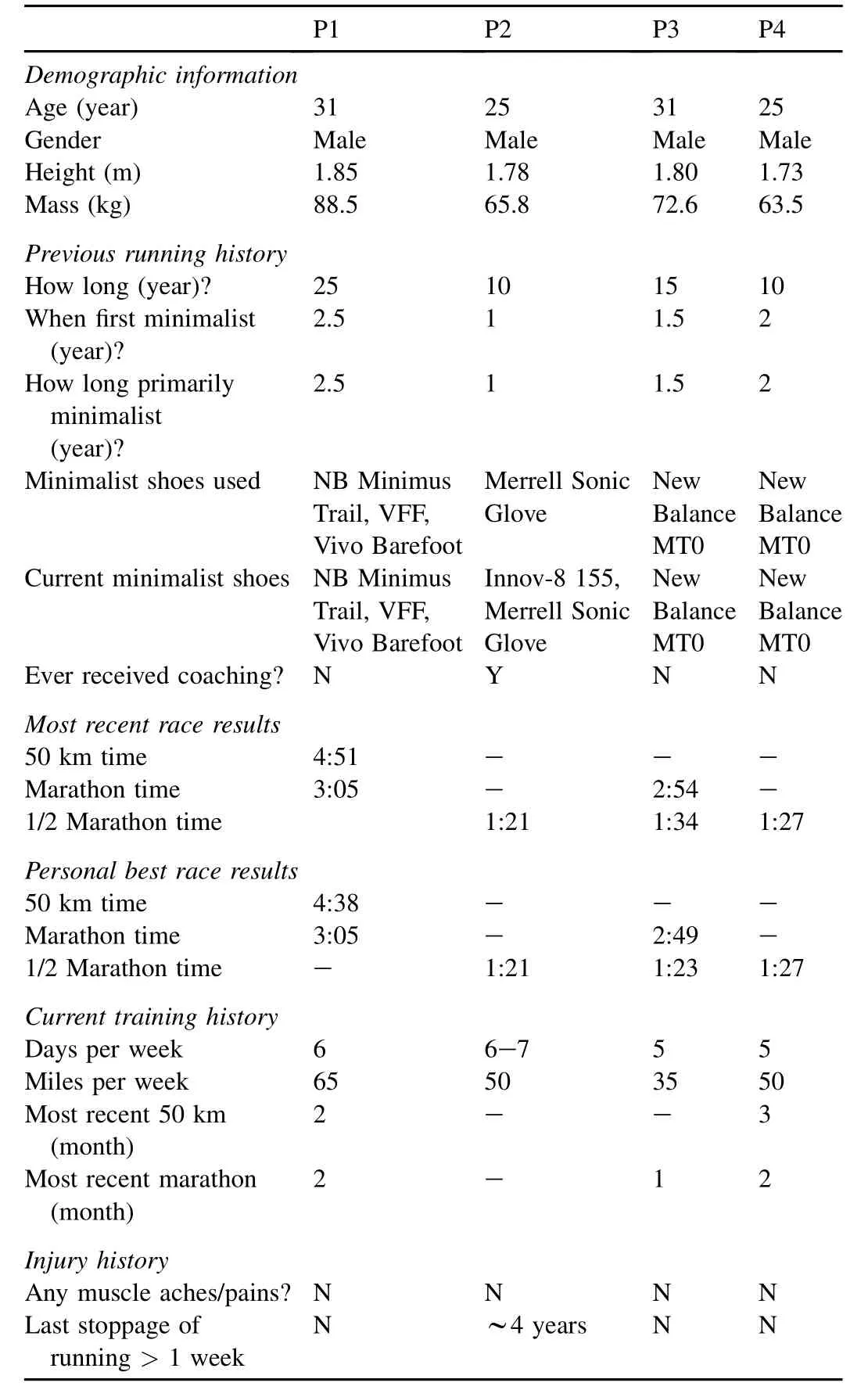
Table 1 Information about study participants.
At the initial data collection,each runner received verbal instructions on the protocol.Warm-up was completed by individual preference.Height and body mass were collected.A heart rate monitor(Garm in Forerunner 910XT;Garm in International Inc.,Olathe,KS,USA)was attached.Skin near anticipated electrode placement was prepped by shaving any body hair,abrading the skin w ith sandpaper,and cleansing w ith alcohol w ipes to minimize impedance.Self-adhesive, disposable,Ag/AgCl snap electrodes(Noraxon USA Inc., Scottsdale,AZ,USA,interelectrode distance=3.8 cm)were placed over the muscle belly according to SENIAM(Surface EMG for Noninvasive Assessment recommendations)20on the follow ing muscles of the right leg:gluteus medius,rectus femoris,biceps femoris,anterior tibialis,and medial gastrocnemius.EMG signals were recorded ata frequency of1500 Hz using a bipolar sEMG recording system(Noraxon USA Inc.). Follow ing placement,each electrode was marked w ith indelible ink marker,and secured w ith ACE w raps.A Biodex System 3 Dynamometer(Biodex Medical Systems,Shirley, NY,USA)was used to perform maximum voluntary contractions(MVCs)for hip abduction,knee extension,knee flexion, ankle dorsiflexion,and ankle plantar flexion.Three trials,each 5 s duration,were conducted foreach muscle on the dominant side only.Follow ing MVC collection,PEDAR dynam ic measuring system insoles(novel GmbH,Munich,Germany) were properly fi t into each shoe and calibrated by zeroing each insole while off-loaded.Reflective markers were placed on participant’s heel and toe of the right leg.A Vicon T-Series Electromagnetic Motion Tracking System(Polhemus Inc., Cochester,VT,USA)was used to capture the movementof the reflective markers at a sampling rate of 60 Hz for determ ination of initial contactand toe-off.Each participantcompleted a 0.8-km treadmill(Landice L8;Landice,Randolph,NJ,USA) run at 2.7 m/s.Heart rate recordings were documented every 0.16 km.Motion capture,PEDAR,and sEMG recordings were collected for 10 consecutive seconds at 0.32-km and 0.64-km distances.Each participant also volunteered a rating of perceived exertion(RPE)score via the Borg RPE index,21as well as subjective identification of any specific muscle group(s)that felt“fatigued”,at0.32 km and 0.64 km distances. Following completion of the 0.8-km treadm ill run,skin markings were verified and sEMG electrodes were removed, as well as the PEDAR insoles,reflective markers,and heart rate monitor.Each participant then completed a 7-loop, 48.4-km outdoor run at an approximate speed of 2.7 m/s.The runner’s course was mapped throughout suburban M ilwaukee, W isconsin,USA,mostly on sidewalks,during late fall (ambient temperature ranged from 0 to 16°C)w ith an overall elevation change of approximately 500 m(max elevation of 250 m).Fluid and nutrition replacement was set-up prior to beginning the outdoor run by each individual at one location, which the runner passed on each loop,or seven times,during the course of the run.Follow ing completion of the 48.4-km run,each participant’s skin was wiped offw ith a dry toweland sEMG electrodes,PEDAR insoles,reflective markers,and heart rate monitor were all replaced.Mean time for replacing measuring equipment and starting the treadm ill run was approximately 2 m in,similar to that reported by Kellis etal.22Each participant then completed another 0.8-km treadm ill run,w ith heart rate recordings documented at 0.16-km intervals and motion capture,PEDAR,and sEMG recordings collected at 0.32-km and 0.64-km distances,as well as postrun MVCs,in sim ilitude w ith pre-50-km run methods.Upon completion,each participantwas crossed over to the opposite shoe type and instructed on re-training in the opposite shoe type for 4 weeks.Follow ing crossover and re-training,data collection was repeated for each participant in the opposite shoe type.
2.3.Data processing
Mean PEDAR insole pressure data(inclusive of instant of peak pressure,peak pressure,maximum force,pressure timeintegral,and contact area)were calculated by PEDAR X software for each runner for each shoe type in both pre-and post-run conditions for each of the 8-footsegments(Fig.1),as previously defined by Liu etal.23Initial foot segment contact was determined by examination of footpressure patterns using PEDAR X software for each foot of each runner.Initial contactand toe-offwere determ ined for each runner by analysis of the reflective markers,from which mean step rate and mean step length were calculated.The raw sEMG signals were fi ltered using MATLAB signal processing tool box(The Mathworks,Natick,MA,USA).A Butterworth fi lter w ith a low-pass frequency of 20 Hz and high-pass frequency of 400 Hz was applied.The median frequency of the fi ltered sEMG signal was calculated w ith custom MATLAB code that utilized MATLAB’s power spectral density function for each muscle group sampled in each runner.Custom MATLAB software was utilized to calculate the rootmean square(RMS) of the fi ltered sEMG signal using a 50-ms w indow for each muscle group sampled in each runner during the follow ing three phases as defined by Kellis et al.:21pre-contact(defined as 100 ms prior to initial contact),initial loading response (defined as the 50-ms interval immediately follow ing initial contact),and main loading response(defined as the period between 50 and 200 ms after initial contact).
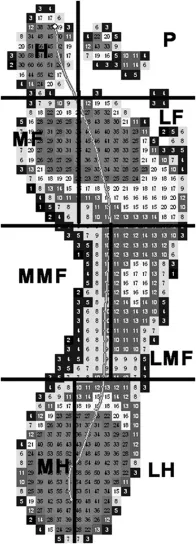
Fig.1.Insole pressure mapping.MH=medial heel;LH=lateral heel; MMF=medial midfoot;LMF=lateral midfoot;MF=medial forefoot; LF=lateral forefoot;H=hallux;P=phalanges.
2.4.Statistical analysis
Pairedttests were used to compare pressure characteristics, stride characteristics,sEMG data,RPE,heart rate,and body mass among differentshoe type and pre-vs.post-run condition using R version 2.12(R Foundation for Statistical Computing, Vienna,Austria).Significance was set atp<0.05.
3.Results
Instant of peak pressure,as a percentage of the gait cycle, and peak pressure are reported by foot segment for each shoe type in both pre-and post-run conditions in Fig.2.There were no significant differences in instant of peak pressure by shoe type.There were no significant changes in instant of peak pressure between pre-and post-run conditions,except for an earlier instant of peak pressure in the lateral forefoot in the m inimalist shoe type and in the hallux in the traditional shoe type in the post-run condition(p< 0.05).There was a significantly greater peak pressure in the minimalistshoe type compared to the traditional shoe type in the medial forefoot (p< 0.05)and lateral forefoot(p< 0.01)in the pre-run condition and in the lateral heel and lateral forefoot in the post-run condition(p< 0.05).There was a significantly greater peak pressure in the post-run compared to pre-run condition in the medial heel and lateral heel(p<0.05)in the m inimalist shoe type;whereas,there was a significantly lower peak pressure time in the post-run compared to pre-run condition in the lateral m idfoot,lateral forefoot,and hallux (p<0.05)in the minimalist shoe type,as well as the medial midfoot(p< 0.01)and medial forefoot(p<0.05)in the traditional shoe type.There were no significant differences in contact area by shoe type except in the medial m idfoot in the post-run condition(p<0.05),where contactarea was smaller in the m inimalistshoe type as compared to the traditionalshoe type.There was a significantly greater pressure time integral observed in the m inimalist shoe type compared to the traditional shoe type in the medial heel post-run(p<0.05),and lateral forefoot both pre-(p<0.01)and post-run(p<0.05). There was a significantly greater pressure time integral in the post-run compared to pre-run condition in the medial heel (p<0.05)in the m inimalist shoe type;whereas,there was a significantly lower pressure time integral in the post-run compared to pre-run condition in the lateral forefoot (p<0.01),and hallux(p<0.05)in the m inimalistshoe type, as well as the medial m idfoot(p<0.05)and medial forefoot (p< 0.05)in the traditional shoe type.There was also a significantly greater maximum force between the pre-and post-run conditions in the medial heel in the minimalist shoe type(p<0.01).

Fig.2.Instantof peak pressure(%gait cycle)(A)and peak pressure(kPa)(B)by foot segment.MH=medial heel;LH=lateral heel;MMF=medialm idfoot; LMF=lateralm idfoot;MF=medial forefoot;LF=lateral forefoot;H=hallux;P=phalanges.*p<0.05,**p<0.01,compared between different shoe types;#p<0.05,##p<0.01,compared between pre-and post-run conditions.
Median frequency of the sEMG recordings was reported by foot segment for each shoe type in both pre-and post-run conditions in Fig.3.There were no significant differences in median frequency in the pre-run compared to post-run condition,except in the rectus femoris(p< 0.05)in the m inimalistshoe type,where the median frequency was greater in the post-run condition.There were no significantdifferences in median frequency by shoe type except in the hip abductor in the post-run condition(p< 0.05),where the median frequency was less in the traditional shoe type.During the precontact phase,there was a significantly greater RMS value during the post-run condition as compared to the pre-run condition in the tibialis anterior in both shoe types (p<0.05).During the initial loading response,there were no significant differences in RMS values.During the main loading response,there was a significantly greater RMS value in the post-run than the pre-run condition in the hip abductors in the minimalist shoe type(p<0.05),as well as a significantly greater RMS value in traditional shoe type compared to the m inimalist shoe type in the tibialis anterior in both pre-(p<0.01)and post-run(p<0.05)conditions.Median frequency of the sEMG recordings of the medial gastrocnem ius for individual runners,as well as change in median frequency of the medial gastrocnem ius in the pre-run compared to postrun condition,subjective fatigue post-run,and change in initial contactarea in the pre-run compared to post-run condition,by shoe type is reported in Fig.4.
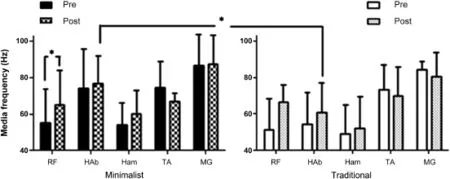
Fig.3.Median frequency.RF=rectus femoris;HAb=hip abductors;Ham=medialhamstrings;TA=tibialis anterior;MG=medialgastrocnem ius.*p<0.05.

Fig.4.Median frequency(Hz)of medial gastrocnem ius,subjective fatigue,and change in initial foot segment contact(i.e.,foot-strike change pattern)by participantin the m inimalist(A)and the traditionalshoe type(B)conditions.P2 had an asymmetric foot-strike post-run in the traditionalshoe type.LF/LMF refers to right foot/left foot.*p<0.05,**p<0.01.
Comparison of step rate and step length by shoe type in preand post-run conditions is demonstrated in Fig.5.RPE values significantly increased between pre-and post-run conditions in both m inimalist(p<0.05)and traditional(p<0.05)shoe types.Heart rate also significantly increased between pre-and post-run conditions in both shoe types(p<0.05).Body mass reduction ranged from 0.4 to 3.6 kg per runner,averaging between 1.4 and 3.4 kg per runner,but did not represent a significant difference between pre-and post-run conditions in either shoe type.RPE,heart rate,and body mass did not vary significantly by shoe type in either the pre-or post-run conditions.Two of the four runners reported fatigue in the gastrocnem ius in the post-run condition in m inimalist shoe type;two of the four runners also reported fatigue in the gastrocnemius in the post-run condition in the traditional shoe type.
4.Discussion
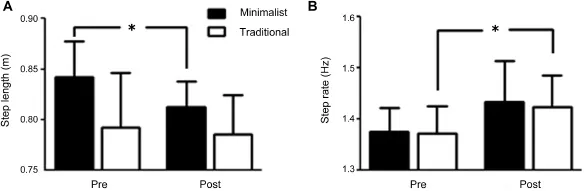
Fig.5.Comparison of step length(A)and step rate(B)by shoe types.*p<0.05.
As initially hypothesized,experienced m inimalist runners did alter gait pattern between pre-and post-run conditions,as previously observed by Larson etal.15and Kasmeretal.16The observed foot-strike pattern from an FFS to a more posteriorfootstrike(MFS)was more common among runners in the traditional shoe type.There were four runners who demonstrated a shift in initial contact area from lateral forefoot to lateral m idfoot after the 50-km run:one runner(both feet)inthe m inimalist shoe type condition and three runners(2 runners both feet,1 runner 1 foot)in the traditional shoe type condition(Fig.4).The observed foot-strike change pattern was further supported by the increased muscle activity,as per the observed increased RMS values,during the pre-contact phase in the tibialis anterior in both shoe type conditions post-run compared to pre-run,sim ilar to previous results of Cheung et al.,24as well as a trend noted by Kellis et al.,22suggesting a more dorsiflexed foot preparatory to initial contact.Of note,given the traditionally accepted foot-strike classifications as described by Lieberman et al.,2this shift in initial contactarea represents a shift from an FFS classification to an MFS classification,but not an RFS classification.
The observed foot-strike change resulted in an increased peak pressure,pressure time integral,and maximum force under the heel.These findings were only significant in the m inimalist shoe type,suggesting that when foot-strike pattern was altered,even if not noted by a clear differentiation from FFS to MFS,the resultant increased peak pressure,pressure time integral,and maximum force were more pronounced in the minimalistshoe type.This finding suggests that the driving etiology of the change in foot-strike pattern may notbe impact force,but another variable,such as muscular fatigue,which w ill be discussed later.The increased peak pressure under the heel(significant in the m inimalist shoe type)post-run is contrary to previous studies of Gerlach etal.9and Willson and Kernozek10thatnoted decreased peak pressure under the heel. The likely explanation was the contradictory change in footstrike pattern.In this study,most runners either changed from an FFS to an MFS or maintained an FFS both pre-and post-run.In the previous studies,as documented by Gerlach et al.,9the foot-strike change pattern was likely a more dorsiflexed RFS to a less dorsiflexed RFS.Thus,the change pattern in this study is in the opposite direction of the change pattern of previous studies,resulting in the exact opposite direction of change in peak pressure under the heel.
In addition to pre-and post-run differences in peak pressure,there was a significantly greaterpeak pressure in multiple footsegmentsobserved in the m inimalistshoe compared to the traditional shoe,namely the lateral heel,as well as the medial and lateral forefoot.This existed in two foot segments in the pre-run condition and two foot segments in the post-run condition.This finding is consistent with a well-known complication of transitioning to a m inimalist shoes,specifically metatarsal stress fractures,as initially described by Giuliani et al.25and more recently Ridge et al.26Thus,the finding of increased peak pressure,specifically in the medial forefoot,in the m inimalist shoe type,combined w ith an inadequate transition time to allow for bone remodeling,muscle fiber adaptations,and neuromuscular reprogramm ing may predispose m inimalist runners to an increased risk of metatarsal stress fractures.
The proposed etiology for the observed change in footstrike pattern was muscle fatigue,specifically muscle fatigue of the plantar flexors,based on work by Kasmer et al.16in ultramarathon runners.This work demonstrated significantly higher CPK values among non-RFS runners compared to RFS runners after a 161-km run,likely a result of the eccentric loading of the plantar flexors seen in an FFS pattern and absent in an MFS or RFS pattern.8,10Thus,it was hypothesized that in addition to observing a change in foot-strike pattern after a 50-km run,we would likewise observe fatigue in the gastrocnem ius,specifically by an observed decrement in median frequency in the sEMG recordings pre-to postrun.27,28However,there was no decrement in median frequency observed from pre-to post-run condition in either shoe type condition observed in the combined data of all four runners.
Further investigation of median frequency of the medial gastrocnem ius,subjective fatigue,and foot-strike change pattern by individual runner by shoe type is displayed in Fig.4.When exam ining our data on an individual basis,our hypothesis that each foot-strike change from forefoot to m idfoot would be supported by a corresponding decrease in median frequency(andvice versa)between pre-and post-run was not supported.In fact,each runner who did change footstrike pattern from forefoot to m idfoot was associated w ith a trend toward an increased median frequency.However,to the authors’know ledge,there have only been two such“longdistance”running protocols examining median frequency of various muscles during prolonged, constant speed running,24,29,30in which one study30demonstrated an increase in median frequency of the rectus femoris,biceps femoris, anterior tibialis,and medial gastrocnem ius during a constant speed,30-m in treadm ill run.Wakeling et al.30suggested the findings are the result of a change in the motor unit recruitment pattern during sustained submaximal activity,specifically that runners may increase recruitment of fast-tw itch fibers and de-recruit slow-twitch muscle fibers in a timedependent manner in order to generate the power output necessary to maintain a constant speed.In the present study, each trial in which the runner changed foot-strike pattern from an FFS in the pre-run condition to an MFS in the post-run condition(P3 in the m inimalist shoe type;P1 and P4 in the traditional shoe type)was accompanied by a trend toward an increase in median frequency of the medial gastrocnemius after the 50-km run.This finding was consistent w ith the fatigue pattern demonstrated in the experiment of Wakeling et al.,30suggesting that a sim ilar change in motor unit recruitment pattern may be contributing to the change in median frequency observed in the presentstudy.Thus,muscle fatigue of the gastrocnem ius,as well greater muscle damage, as observed as significantly greater CPK values among non-RFS runners than RFS runners after a 161-km ultramarathon,may contribute to the change of foot-strike pattern in long-distance runners.However,further investigation is warranted to support this theory,as well as alternative explanations that may contribute to the findings in the present study.
Our final hypothesis,i.e.,that step rate would increase and step length would decrease in the post-run condition in both shoe types was consistent w ith our findings,as well as w ith previous studies,namely a high-intensity,relatively short distance fatigue protocol,10a marathon distance,17and ultramarathon distances.11,14
As expected,the completion of a 50-km run resulted in a significant increase in RPE between pre-and post-run conditions,consistent w ith a previous ultramarathon distance study of Martin et al.31Of the four runners that subjectively identified post-run gastrocnemius fatigue(1 runner in both shoe types,1 runner in only the minimalist shoe type,and 1 runner in only the traditional shoe type),two runners demonstrated an increased median frequency and altered the initial contact area from lateral forefoot to lateral midfoot. The other two runners that subjectively identified post-run gastrocnemius fatigue demonstrated a decreased median frequency and did not alter initial contact area between lateral forefoot and lateral m idfoot.In addition,heart rate elevations were observed consistently between pre-and post-run conditions,w ithin expectations for an endurance-type event. Heart rate was between 116 and 150,or 59%—77%of estimated maximum heart rate,as determ ined by 220-age.Of note,each runner experienced a reduction in body mass over the 50-km run for each trial,between 0.4 kg(0.6%)and 3.6 kg(4.3%),w ithin the range of findings observed in a recent study of marathon runners,where mean body mass reduction was 2.2%±1.2%.32
5.Conclusion
This study analyzed both kinetic and stride characteristics of runners in m inimalist,as well as traditional shoes,both at the beginning and end ofa 50-km run through the collection of pressure data,sEMG recordings,and lim ited 3D motion capture data.Of significance,the runners in this study who adopted a more posterior initial contact area after the 50-km run were those more closely associated w ith muscle fatigue of the gastrocnemius as defined by the theory of Wakeling et al.,30which may accompany long-distance,sustained velocity running.In addition,peak pressures were significantly greater in the m inimalist shoe type,specifically in the medial forefoot,which may predispose to an increased risk of metatarsal stress fractures in the setting of improper training.
Due to the limited study size of only FFS runners,the ability to generalize to all runners of varying foot-strike patterns must be cautioned.Additional studies are necessary to (a)validate the observed findings of altered gait pattern, pressure data,and stride characteristics as a resultof fatigue in both shoe type conditions;(b)further investigate the applicability of the isometric,constant force contraction theory in a dynam ic,endurance exercise,such as running;and(c)further investigate the proposed theory of change in motor unit recruitment etiology observed during sustained,submaximal activity,such as endurance running.
Acknow ledgm ent
This study was supported,in part,by the MedicalCollege of Wisconsin’s Department of Physical Medicine&Rehabilitation,as wellas by grant1UL1RR031973 from the Clinicaland Translational Science Award(CTSA)program of the National Center for Research Resources,National Institutes of Health.
1.Robbins SE,Gouw GJ,Hanna AM.Running-related injury prevention through innate impact-moderating behavior.Med Sci Sports Exerc1989;21:130—9.
2.Lieberman DE,Vedkadesan M,Werbel WA,Daoud AI,D’Andrea S, Davis IS,et al.Foot strike patterns and collision forces in habitually barefoot versus shod runners.Nature2010;463:531—6.
3.Squadrone R,GallozziC.Biomechanicaland physiologicalcomparison of barefootand two shod conditions in experience barefoot runners.J Sports Med Phys Fitness2009;49:6—13.
4.DivertC,Mornieux G,Baur H,Mayer F,Belli A.Mechanical comparison of barefoot and shod running.Int J Sports Med2005;26:593—8.
5.De Wit B,De Clercq D,Aerts P.Biomechanical analysis of the stance phase during barefoot and shod running.J Biomech2000;33:269—78.
6.Bonacci J,Saunders PU,Hicks A,Rantalainen T,Vicenzino BG, Spratford W.Running in a m inimalistand lightweightshoe isnotthe same as running barefoot:a biomechanicalstudy.Br J Sports Med2013;47:387—92.
7.Dickinson JA,Cook SD,LeinhardtTM.The measurementof shock waves follow ing heel strike while running.J Biomech1985;18:415—22.
8.M illet GY,Hoffman MD,Morin JB.Sacrificing economy to improve running performance—a reality in the ultramarathon?J Appl Physiol2012;113:507—9.
9.Gerlach KE,White SC,Burton HW,Dorn JM,Leddy JJ,Horvath PJ. Kinetic changes w ith fatigue and relationship to injury in female runners.Med Sci Sports Exerc2005;37:657—63.
10.Willson JD,Kernozek TW.Plantar loading and cadence alterations w ith fatigue.Med Sci Sports Exerc1999;31:1828—33.
11.Morin JB,Samozino P,M illet GY.Changes in running kinematics,kinetics,and spring-mass behavior over a 24-h run.Med Sci Sports Exerc2011;43:829—36.
12.M illet GY,Morin JB,Degache F,Edouard P,Feasson L,Veryney J,et al. Running from Paris to Beijing:biomechanical and physiological consequences.Eur J Appl Physiol2009;107:731—8.
13.Nicol C,Komi PV,Marconnet P.Fatigue effects of marathon running on neuromuscular performance.I.Changes in muscle force and stiffness characteristics.Scand J Med Sci Sports1991;1:10—7.
14.Morin JB,Tomazin K,Edouard P,M illet GY.Changes in running mechanics and spring-mass behavior induced by a mountain ultra-marathon race.J Biomech2011;44:1104—7.
15.Larson P,Higgins E,Kaminski J,Decker T,Preble J,Lyons D,etal.Foot strike patterns of recreation and sub-eilite runners in a long-distance road race.J Sport Sci2011;29:1665—73.
16.Kasmer ME,W ren JJ,Hoffman MD.Foot strike pattern and gait changes during a 161-km ultramarathon.J Strength Cond Res2014;28:1343—50.
17.Kyrolainen H,Pullinen T,Candau R,Avela J,Huttunen P,Kom i PV. Effects of marathon running on running economy and kinematics.Eur J Appl Physiol2000;82:297—304.
18.Haussw irth C,Bigard AX,Guezennec CY.Relationships between running mechanics and energy cost of running at the end of a triathlon and a marathon.Int J Sports Med1997;18:330—9.
19.Thompson WR,Gordon NF,Pescatello LS,American College of Sports Medicine.ACSM’s guidelines forexercise testing and prescription.8th ed. Baltimore:Lippincott W illiams&W ilkins;2010.p.400.
20.Hermens HJ,Freriks B,Merletti R,Hagg G,Stegeman D,Blok J,et al.SENIAM 8:European recommendations for surface electromyography. Enschede,The Netherlands:Roessingh Research and Development;1999.
21.Borg G.Perceived exertion and pain rating scales.Champain,IL:Human Kinetics;1998.
22.Kellis E,Zafeiridis A,Am iridis IG.Muscle coactivation before and after the impact phase of running follow ing isokinetic fatigue.J Athl Train2001;46:11—9.
23.Liu X,Lyon R,Thometz JG,Curtin B,Tarima S,Tassone C.Insolepressure distribution for normal children in differentage groups.J Pediatr Orthop2011;31:705—9.
24.Cheung RTH,Ng GYF.Motion controlshoe delays fatigue of shank muscles in runners with overpronating feet.Am J Sports Med2010;28:486—91.
25.Giuliani J,Masini B,A litz C,Owens B.Barefoot-stimulating footwear associated with metatarsal stress injury in 2 runners.Orthopedics2011;34:e320—3.
26.Ridge ST,Johnson AW,M itchell UH,Hunter I,Robinson E,Rich BS, et al.Foot bone marrow edema after a 10-wk transition to m inimalist running shoes.Med Sci Sports Exerc2013;45:1363—8.
27.Moritani T,Nagata A,Muro M.Electromyographic manifestations of muscular fatigue.Med Sci Sports Exerc1982;14:198—202.
28.Basmajian JV,De Luca CJ.Muscle fatigue and time-dependant parameters of the surface EMG signal.In:Basmajian JV,De Luca CJ,editors.Muscles alive.5th ed.Baltimore,Maryland:W illiams and Wilkins;1985. p.201—22.
29.Cheung RTH,Ng GYF.Motion control shoe affects temporal activity of quadriceps in runners.Br J Sports Med2009;43:943—7.
30.Wakeling J,Pascual SA,Nigg BM,von Tscharner V.Surface EMG shows distinct populations of muscle activity when measured during sustained sub-maximal exercise.Eur J Appl Physiol2001;86:40—7.
31.Martin V,Kerherve H,Messonnier LA,Banfi JC,GeyssantA,Bonnefoy R, et al.Central and peripheral contributions to neuromuscular fatigue induced by a 24-h treadmill run.J Appl Physiol2010;108:1224—33.
32.Del Coso J,Salinero JJ,Abian-Vicen J,Gonzalez-M illan C,Garde S, Vega P,et al.Infl uence of body mass loss and myoglobiunuria on the development of muscle fatigue after a marathon in a warm environment.Appl Physiol Nutr Metab2013;38:286—91.
Received 20 September 2013;revised 31 January 2014;accepted 17 March 2014
*Corresponding author.Presentaddress:Departmentof Orthopaedic Surgery, Cleveland Clinic Sports Health Center,5555 Transportation Boulevard,Garfield Heights,OH 44125,USA.
E-mail address:kasmerm@ccf.org(M.E.Kasmer)
Peer review under responsibility of Shanghai University of Sport.
2095-2546/$-see front matter CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.A ll rights reserved. http://dx.doi.org/10.1016/j.jshs.2014.03.005
 Journal of Sport and Health Science2014年2期
Journal of Sport and Health Science2014年2期
- Journal of Sport and Health Science的其它文章
- Can m inimal running shoes im itate barefoot heel-toe running patterns? A comparison of lower leg kinematics
- The effect of m inimal shoes on arch structure and intrinsic foot muscle strength
- Strike type variation among Tarahumara Indians in m inimal sandals versus conventional running shoes
- Foot strike patterns and hind limb joint angles during running in Hadza hunter-gatherers
- Muscle activity and kinematics of forefoot and rearfoot strike runners
- Impact shock frequency components and attenuation in rearfoot and forefoot running