
Impact shock frequency components and attenuation in rearfoot and forefoot running
2014-03-21 02:33AllisonGruerKtherineBoyerTimothyDerrickJosephHmill
Allison H.Gruer,Ktherine A.Boyer,Timothy R.Derrick,Joseph Hm ill,*
aBiomechanics Laboratory,University of Massachusetts Amherst,Amherst,MA 01003,USA
bBiomechanics Laboratory,Iowa State University,Ames,IA 50011,USA
Impact shock frequency components and attenuation in rearfoot and forefoot running
Allison H.Grubera,Katherine A.Boyera,Timothy R.Derrickb,Joseph Ham illa,*
aBiomechanics Laboratory,University of Massachusetts Amherst,Amherst,MA 01003,USA
bBiomechanics Laboratory,Iowa State University,Ames,IA 50011,USA
Background:The forefoot running footfall pattern has been suggested to reduce the risk of developing running related overuse injuries due to a reduction of impact related variables compared w ith the rearfoot running footfall pattern.However,only time-domain impact variables have been compared between footfall patterns.The frequency contentof the impactshock and the degree to which it is attenuated may be of greater importance for injury risk and prevention than time-domain variables.Therefore,the purpose of this study was to determ ine the differences in head and tibial acceleration signal power and shock attenuation between rearfoot and forefoot running.
Methods:Nineteen habitual rearfoot runners and 19 habitual forefoot runners ran on a treadmillat3.5 m/s using their preferred footfallpatterns while tibial and head acceleration data were collected.The magnitude of the fi rst and second head acceleration peaks,and peak positive tibial acceleration were calculated.The power spectral density of each signal was calculated to transform the head and tibial accelerations in the frequency domain.Shock attenuation was calculated by a transfer function of the head signal relative to the tibia.
Results:Peak positive tibialacceleration and signalpower in the lower and higher ranges were significantly greater during rearfoot than forefoot running(p<0.05).The fi rst and second head acceleration peaks and head signal power were not statistically different between patterns (p>0.05).Rearfoot running resulted in significantly greater shock attenuation for the lower and higher frequency ranges as a result of greater tibial acceleration(p<0.05).
Conclusion:The difference in impact shock frequency content between footfall patterns suggests that the primary mechanisms for attenuation may differ.The relationship between shock attenuation mechanisms and injury is notclearbutgiven the differences in impact frequency content, neither footfall pattern may be more beneficial for injury,rather the type of injury sustained may vary w ith footfall pattern preference.
CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.All rights reserved.
Frequency domain;Impact shock;Running footfall patterns;Shock attenuation;Tibial acceleration
1.Introduction
Vertical impactvariables,such as the magnitude and rate of the vertical impact peak and impact shock,have long been at the center of the running injury debate.The forefoot(FF)and m idfoot(MF)running footfall patterns have recently been associated w ith lower rates of running injuries compared w ith rearfoot(RF)running.1,2The absence or reduction of the vertical ground reaction force(GRF)impact peak in FF and MF running has been the suggested explanation for these findings.However,impact variables,such as characteristics of the vertical GRF and impactshock,have been related to injury in some studies(e.g.,Refs.3—5)but not others(e.g.,Refs. 6—8).For example,one study found a lower relative injury frequency in those considered to have high vertical impact force magnitudes or loading rates compared w ith individualsconsidered to have low vertical impact force magnitudes or loading rates.9Other vertical GRF variables,such as the active peak magnitude,may also be related to the development of running injuries10—12but this aspecthas been virtually ignored in the running injury debate.One thing remains clear:running injuries develop because of complex interactions between many variables,regardless of footfall pattern.Further exam ination of impact related variables may reveal that the joints or tissues susceptible to injury may differ between footfall patterns.
The events surrounding the foot-ground collision during running are the main source of the impact shock that is transm itted through the leg and the rest of the body.This impact shock is closely related to vertical GRF characteristics and running kinematics.13—17Anything that affects segment velocity the instant before initial contact,such as running speed,stride frequency,and joint orientation,w ill determ ine the change in momentum of the foot and leg at initial contact and thus the magnitude and rate of the vertical impact peak and impactshock.14,18—20The frequency contentof the impact shock w illdepend on the magnitude and timing of the vertical GRF.13Given the differences in vertical GRF characteristics and kinematics between footfall patterns,the impact shock resulting from each footfall pattern may exhibit different frequency content.The frequency content of impact parameters may be a significant contributor to running related injuries because the capacity of different tissues and mechanisms to transmit and attenuate the impact shock may be frequency dependent.21
The frequency content and signal power of the impact shock and tibial acceleration during stance are determined primarily by the acceleration of the leg segments and whole body center of mass(COM).13Specifically,the tibial acceleration profi le in RF running contains a lower frequency range (4—8 Hz)representing voluntary lower extrem ity motion and the vertical acceleration of the COM during the stance phase and a higher frequency range(10—20 Hz)representing the rapid deceleration of the foot and leg at initial ground contact.13—15,17,22These lower and higher frequency ranges are also representative of the active peak and impact peak of the vertical GRF,respectively.13,17In the time domain,the existence of a prom inent impact peak in RF running buta greater active peak magnitude in FF running10,23,24suggest that the signal power contained in these lower and higher frequency ranges may differ between footfall patterns and may also affect how these frequencies are attenuated.
The impact shock must be attenuated to prevent the disruption of the vestibular and visual systems as a result of excessive head acceleration.14,15,22,25,26Attenuation occurs primarily through energy absorption from active muscles, changes in joint geometry,and deformation of passive tissues.27—31The body responds to greater impactmagnitudes by increasing attenuation through a combination of active and passive mechanisms.12,30The reliance on certain shock attenuation mechanisms may depend on the frequency content of the impactshock.Passive mechanisms,such as deformation of the heel fatpad,the running shoe,ligaments,bone,muscle oscillation,and articular cartilage are responsible for attenuating the higher frequency waveforms generated at initial ground contact.27—31Pre-activation of muscle w ill change to increase damping of impact shock frequencies greater than 40 Hz.32However,muscle contractions specifically responding to the impact stimulus and some other attenuation mechanisms may only be effective atattenuating frequencies below 10 Hz because of muscle latency periods.29,33Active shock attenuation mechanisms include eccentric muscle contractions,increased muscle activation,changes in segment geometry,and adjustments in joint stiffness.14,32,34—38However, the body may have a reduced capacity for attenuating lower frequency components.14,26The capacity and degree of attenuation w ill be dictated by the frequency content of the impactshock and the mechanisms available forattenuation.A reduced capacity for attenuation by some tissues or mechanisms may result in a greater reliance on other tissues or mechanisms and could potentially result in a tissue becom ing overloaded.28,39,40
Differences in impact parameters between RF and FF running have only been exam ined in the time domain to our know ledge.However,itmay be important to examine impact parameters in the frequency domain because differences in the frequency content of the impact shock may alter the reliance on specific shock attenuation mechanisms in RF versus FF running and the degree of attenuation that occurs.A recent study found that RF running resulted in a greater percent difference in peak acceleration between the head and tibia signals in the time domain than FF running.41That study was an excellent fi rst step investigating shock attenuation between footfall patterns using a transfer function in the time domain determine shock attenuation.However,given that frequency content dictates shock transm issibility,21important information may be lost regarding attenuation of specific frequency components and the mechanisms used for attenuation when using a time domain analysis.
Time domain differences in kinematics and vertical GRF characteristics between footfall patterns suggest that the impact shock may contain different frequency domain characteristics that are dictated by these kinematic and kinetic events.Specifically,the presence of the vertical GRF impact peak in RF running and greater verticalGRF active peak in FF running may result in differences in signalpowerof the higher and lower frequency ranges of the impactshock and the degree that shock is attenuated.Therefore,the purpose of this study was to determ ine the difference in the frequency contentof the impact shock and its subsequent attenuation between footfall patterns.Itwas hypothesized that RF running would result in greater peak tibialacceleration and signal power in the higher frequency range,representative of the vertical GRF impact peak,compared w ith FF running whereas tibial acceleration power in the lower frequency range,representative of the vertical GRF active peak,would be greater in FF than in RF running.Although RF running results in greater tibial acceleration than FF running,23head acceleration may be sim ilar because shock attenuation increases in response to greater impact loads to maintain head stability for proper vestibularand visual function.14,17,22,26Therefore,it was hypothesized that peak head acceleration and signal power in the lower and higher frequency ranges would not differ between footfall patterns.As a result of the previous observation that impact shock was greater w ith RF than FF running,23it was hypothesized that RF running would result in greater shock attenuation of the higher range frequency components than FF running.However,previous studies have indicated a reduced capacity for attenuation of lower frequency components,14,26therefore it was hypothesized that no difference would be observed in the degree of attenuation of the lower frequency components between footfall patterns.
2.M aterials and m ethods
2.1.Participants
Nineteen habitual RF runners and 19 habitual FF runners participated in this study(Table 1).Sample size estimation determ ined that12 runners per group were required to achieve a powerof0.8 and an alpha levelof0.05.Allparticipants were healthy,experienced runners and did not have a history of cardiovascular or neurological problems.Inclusion criteria required thatparticipants completed a m inimum of16 km/week at a m inimum preferred running speed of 3.5 m/s and had not developed an injury to the lower extrem ity or back w ithin the past year.
Participants were divided into an RF group or an FF group based on the footfall pattern habitually performed when distance running.The participants’habitual footfall pattern was determ ined by assessing the strike index,vertical GRF profi le, and sagittal plane angle ankle at touchdown while the participants ran at his or her preferred speed over a force platform (OR6-5;AMTI,Watertown,MA,USA).42Given that approximately 20%—25%of runners are either MF or FF runners,participants classified as either MF or FF were place in the FF group to ensure appropriate statistical power.All participants read and completed an informed consent document and questionnaires approved by the University Institutional Review Board.
2.2.Experimental setup
Three-dimensional kinematics of the right leg and foot were recorded using a 9-camera high-resolution motion capture system(Qualysis Inc.,Gothenburg,Sweden)at240 Hz to verify the footfall pattern performed by each participant.Kinematic data collection procedures and reflective marker placement are described elsewhere.43Low-mass(<4 grams), uniaxial,piezoelectric accelerometers(ICPⓇ;PCB Piezotronics,Depew,NY,USA)were attached to the center of the forehead and the distalanteromedialaspectof the tibia.22Each attachmentsite was chosen to reduce the effects of soft tissue vibration.44The axis of each accelerometer was aligned w ith the vertical axis of the lower leg while the participant was standing.The vertical axis of the lower leg was aligned w ith the vertical axis of the laboratory coordinate system.The accelerometers were sampled at 1200 Hz and voltage was amplified by a factor of 10.Lower extremity motion and accelerometer data were collected synchronously.
2.3.Protocol
Participants wore neutral racing flats(RC 550;New Balance,Brighton,MA,USA)provided by the laboratory.Accelerometers were secured to the head and distalanteromedial tibia by rubber straps tightened to participant tolerance.Participants warmed up for several m inutes before data were collected by running on the treadm ill(Star Trac;Unisen,Inc., Irivine,CA,USA)w ith their habitual footfall pattern.The RF group was instructed to land w ith a heel-strike and the FF group was instructed to land w ith a toe-strike to reduce any affect of treadm ill running on their footfall kinematics.The sagittal plane kinematics of all participants on the treadm ill were not statistically different than their footfall pattern performed during the over-ground screening.After the warm-up, participants ran for2 min on the treadm illat3.5 m/s with their habitual footfall pattern before accelerometer and motion capture data were recorded.Data were collected for the last 15 s of the 2-m in running period.
2.4.Data analysis
The sagittal plane ankle jointangle during the stance phase was determ ined from the processed kinematic data according to previously reported methods.43Time domain and frequency parameters from the tibia and head accelerometers were calculated using a custom MATLAB program(Mathworks, Inc.,Natick,MA,USA).Time domain parameters from the tibia and head accelerometers were determ ined from 15 stance phases performed by each participant.A least-squares best fi t line was subtracted from the raw data of each signal to remove any linear trend.17Data were then fi ltered w ith a second order Butterworth low-pass fi lter with a cut-off frequency of 60 Hz.16The fi rst(HP1)and second(HP2)peak of the head acceleration signal occurred between 1%and 30%of stance and 31%—101%of stance,respectively.Peak positive tibialacceleration(PPA)was identified as the peak occurring between 1%and 20%of stance.

Table 1 Participant characteristics of the rearfoot group(RF)and the forefoot group(FF)(mean±SD).
Unfi ltered head and tibial acceleration data from each stance phase were detrended then padded w ith zeros to equal 2048 data points,ensuring periodicity.17The power of the stance phase head and tibia acceleration in the frequency domain was determ ined by calculating the power spectral density(PSD)using a square w indow.Exam ination of the acceleration signals collected over the entire stance phase follows the periodic assumptions of Fourier analysis and allows for examination of frequencies below 15 Hz.45,46The PSD was performed on frequencies 0 to the Nyquist frequency (FN)and normalized to 1 Hz bins.14,22A fter binning,the PSD was normalized in order for the sum of the powers from 0 toFNto be equal to the mean squared amplitude of the data in the time domain.Examining the PSD results revealed two primary peaks or local maxima for the tibial and head acceleration signal power in both RF and FF running that were outside of the lower(4—8 Hz)and higher(10—20 Hz)ranges previously identified in the literature for RF running.13—15,17As a result,we expanded the lower and higher frequency ranges investigated to 3—8 Hz and 9—20 Hz,respectively,to more appropriately include the dom inating frequency components of each footfall pattern.The frequency at which peak power occurred w ithin the lower and higher frequency range of the tibial(TPFlow,TPFhigh)and head(HPFlow,HPFhigh) acceleration signal was determined.Signal power magnitude in the frequency domain was quantified by the integral of the signal power contained in the lower and higher frequency ranges in the tibial(TSMlow,TSMhigh)and head(HSMlow, HSMhigh)acceleration signals.15
A transfer function has been previously used to determine the degree of shock attenuation in human running by calculating the ratio of each frequency bin between the tibial and head signal14,15,19,22(i.e.,the transm issibility of each frequency component21).The transfer function was calculated across all frequencies from 0 toFNto determine the degree of shock attenuation occurring between the tibia to the head by:

Foreach frequency,the transfer function calculated the gain or attenuation,in decibels,between the tibia and head signals. Positive values indicated a gain,or increase in signal strength, and negative values indicated attenuation,or decrease in signal strength.A gain in lower frequency components is typically a result of changes in head vertical velocity and voluntary segment motion during the stance phase whereas negative values indicate attenuation in signalpower as the impactshock travels through the body.17,22Shock attenuation magnitude was quantified by the integral of the transfer function result w ithin the lower(ATTlow)and higher frequency ranges(ATThigh).
2.5.Statistical analysis
For the lower and higher frequency ranges,tibialand head peak signal power and signal magnitude were averaged across all stance phases of each participant and then across group. Group means for shock attenuation magnitude were also determ ined in this manner.A one-way analysis of variance was used to determ ine the difference between time and frequency domain acceleration variables between the RF and FF groups running w ith their habitual footfall pattern(α=0.05) using SPSS Statistics version 21.0(IBM,Amonk,NY,USA). Effect sizes(d)were also calculated to determ ine if the differences between groups were biologically meaningful(smalld≤0.3,moderated≤0.5,larged≤0.8).47
3.Results
3.1.Head and tibial acceleration in the time domain
Ankle joint angles measured during the treadm ill running confi rmed that the RF group ran w ith a dorsiflexion angle at touchdown whereas the FF group ran w ith a plantar flexion angle at touchdown(Fig.1).
Tibial and head acceleration in the time domain were plotted in Fig.2.There was no significantdifference in HP1 or HP2 between footfall patterns(p>0.05)(Table 2).However, RF running resulted in a greater PPA compared w ith FF running(p=0.009).
3.2.Head and tibialacceleration in the frequency domain
Tibial and head acceleration signals in the frequency domain were plotted in Fig.3A and B,respectively.HPFlowwas statistically greater during FF compared w ith RF running (p=0.001).TPFhighwas statistically greater during RF compared w ith FF running(p<0.001).No statistical difference was observed for HPFhighor TPFlow(p>0.05)(Table 2).
No statistical difference was detected between footfall patterns for HSMlowor HSMhigh(p>0.05)(Table 2).BothTSMlowand TSMhighwere statistically greater during RF running than FF running(p<0.001)(Table 2).
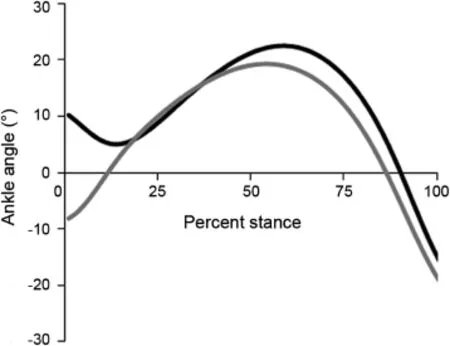
Fig.1.Mean time series of sagittalplane ankle jointmotion compared between the rearfoot(black)and forefoot(grey)groups performing their habitual footfall pattern during the treadm ill running.
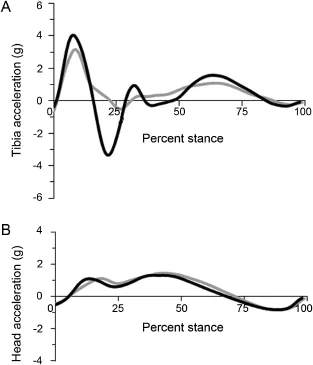
Fig.2.Mean tibial(A)and head(B)acceleration in the time domain compared between the rearfoot(black)and forefoot(grey)groups perform ing their habitual footfall pattern.
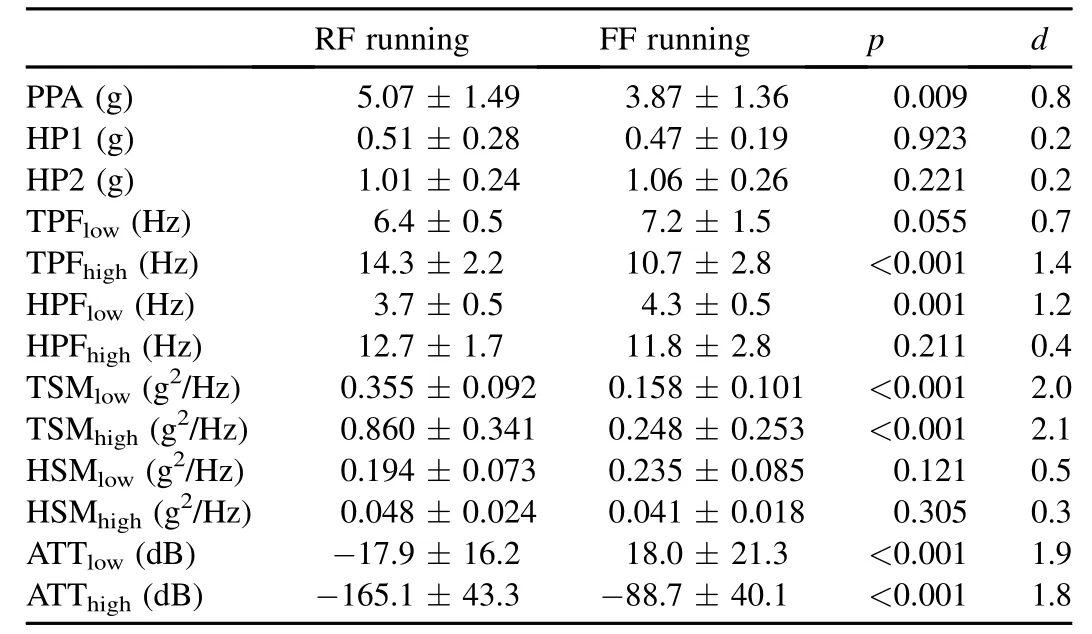
Table 2 Time domain and frequency domain characteristics of rearfoot(RF)and forefoot(FF)groups perform ing their habitual footfall pattern.Variables included:peak positive tibialacceleration(PPA);fi rst(HP1)and second(HP2) head acceleration peaks;frequency of peak power of the tibial(TPFlow,high) and head(HPFlow,high)acceleration signal w ithin the lower and higher frequency ranges;signal power magnitude of the tibial(TSMlow,high)and head (HSMlow,high)acceleration signal w ithin the lower and higher frequency ranges;and shock attenuation magnitude in the lower(ATTlow)and higher (ATThigh)frequency ranges.Positive values for ATTlow,highindicate a gain in signal power whereas negative values indicate attenuation of signal power (mean±SD).
3.3.Impact shock attenuation
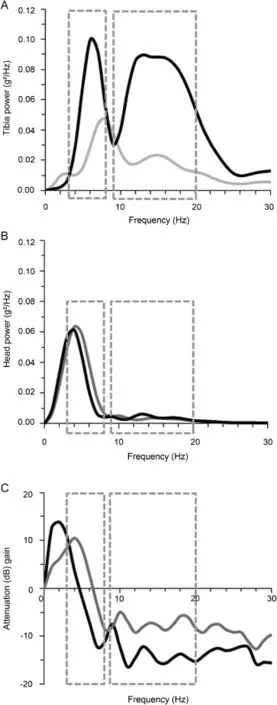
Fig.3.Mean power spectra of the tibia(A)and head(B)acceleration signals and(C)transfer function compared between the rearfoot(black)and forefoot (grey)groups perform ing their habitual footfall pattern.Boxes indicate the lower(3—8 Hz)and higher(9—20 Hz)frequency ranges investigated.
The lowest frequency thatwas attenuated was 5.1±0.5 Hz (mean±SD)in RF running and 6.9±0.9 Hz in FF running(p< 0.001,d=2.5)(Fig.3C).RF running resulted in attenuation of frequencies contained in ATTlowwhereas FF running resulted in a gain of these frequencies(p< 0.001) (Table 2).ATTlowwas positive in FF running because the gain of frequencies between 3 and 5 Hz was larger than the attenuation of frequencies between 6 and 8 Hz(Fig.3C).RF running resulted in significantly greater ATThighthan FF running as indicated by a larger negative value for ATThigh(p<0.001)(Table 2).
4.Discussion
The aim of this study was to determ ine if there were differences in the frequency content of impact shock and its subsequent attenuation between RF and FF running patterns. The fi rst hypothesis,that RF running would result in greater peak tibial acceleration and signal power in the higher frequency range(9—20 Hz)than FF running,was supported whereas tibialacceleration power in the lower frequency range (3—8 Hz)would be greater in FF than in RF running,was not supported.The higher frequency range is representative of the vertical impactpeak and the rapid deceleration of the footand leg follow ing initial ground contact.13,17RF running resulted in greater tibialacceleration power in the higher range because of the greater peak positive acceleration observed in the time domain w ith this pattern compared w ith FF running.Previous studies have indicated that jointkinematics at impact,such as greater heel vertical velocity,greater lower leg angle, decreased knee flexion angle,and a greater stride length result in greater tibial acceleration at impact.14,15,18,19,26,48,49Some of these kinematic features have been observed previously w ith RF compared w ith FF running.23Therefore,the joint geometry characteristics of RF running at foot-ground collision result in greater peak tibialacceleration magnitude in the time domain and greater tibialacceleration signalpower in the frequency domain compared w ith FF running.
Joint and segment configurations at term inal sw ing w ill influence the velocity of the foot and leg just prior to impact and thus the force and rate of deceleration required to terminate foot and leg movement at initial contact.As a result, impact shock magnitude and the frequency that peak power occurs w ill also be affected.In the higher frequency range, peak powerof the tibialacceleration signaloccurred ata lower frequency during FF running compared w ith RF running.This finding may indicate that FF running results in a lower rate of tibial acceleration in the time domain at initial contact compared w ith RF running.Greater ankle compliance during FF running23,50may contribute to a lower rate of tibial deceleration after ground contact compared w ith RF running and may also delay the time that the vertical impactpeak GRF occurs in FF running.A delay in the tim ing of the impactpeak may explain why it is not visible in the time domain vertical GRF during FF running.51
Tibial acceleration signal power in the lower frequency range,representing the vertical GRF active peak and active movement of the leg and foot and whole body COM during stance,13,17was hypothesized to be greater during FF running than RF running because previous studies observed greater vertical GRF active peak magnitude in the time domain w ith FF running.23,24Contrary to this hypothesis,RF running resulted in greater tibial acceleration power magnitude in the lower range compared w ith FF running.Previous observations that RF running results in greater knee flexion excursion and velocity,23a greater stride length,and a greater contact time52may explain these results because these kinematics result in greater tibial signal power magnitude of frequencies below 10 Hz.14,17,22However,the frequency that peak tibial acceleration signal power occurred in the lower range was sim ilar between footfall patterns indicating a sim ilar rate of tibial acceleration during stance after initial contact.This result suggests that the dom inant frequency component contributing to the overall tibial acceleration waveform in the lower frequency range is sim ilarbetween footfallpatterns.Sim ilar rates of tibial acceleration may be a consequence of a greater tibial acceleration power magnitude occurring over a longer ground contact time in RF running compared w ith a lower rate of tibial acceleration magnitude occurring over a shorter ground contact time in FF running.
In support of the second hypothesis,the fi rst and second peaks of the head acceleration signal in the time domain and the head acceleration power in the lower and higher frequency ranges were not different between footfall patterns.Additionally,there was no difference in the frequency that peak head acceleration occurred w ithin the higher range.These results were expected because the body is able to respond to varying impact situations to maintain head stability14,17,22,26and suggest that the body is able to sufficiently attenuate the impact shock that occurred during both footfall patterns. However,peak power of the head acceleration signal within the lower frequency range was greater in FF running compared w ith RF running whereas there was no difference between patterns in the frequency of peak power in the higher range. This result indicates that the head and whole body COM oscillates at a greater dominate frequency in FF than in RF running,which reflects a greater rate of head acceleration in the time domain.The rate of acceleration of head may be greater w ith FF running because of the shorter contact time available to reverse the COM downward velocity after impact and may contribute to greater vertical GRF active peaks10,23,24,53than RF running.The rate of head and COM acceleration may be greater w ith FF running despite previous findings that this pattern m inim izes vertical COM excursion.23
Our third hypothesis was partially supported as there was greater impact attenuation through the body for RF running compared w ith FF running in both the lower and higher frequency ranges rather than just the higher frequency range.The present study supports previous findings that RF running increased impact shock attenuation measured in the time domain41and peak tibial acceleration compared w ith FF running.23,24Greater attenuation of the higher frequency components resulting from the foot-ground collision was likely a result of the body responding to greater tibial acceleration in the time and frequency domains compared w ith FF running.However,in the lower frequency domain,FF runningresulted in a gain of signalpower whereas RF running resulted in attenuation of these frequencies.The difference in the lowest frequency thatwas attenuated in RF compared w ith FF running may explain these results and why RF running resulted in greater attenuation of frequencies in the lower range compared with FF running.During RF running,the lowest frequency thatwas attenuated was between 4 and 6 Hz across participants whereas the lowest frequency that was attenuated during FF running was between 5 and 9 Hz (Fig.3C).A gain in signal power of the lower frequency components is typically a result of vertical oscillation of the COM and joint flexion occurring during stance that generate signal power of these lower frequency components.13,17This increase in signal power of low frequency components is reflected by the observation that FF running resulted in greater power of the head acceleration signal in this frequency range compared w ith RF running.
Impactshock attenuation occurs by a combination of active and passive mechanisms.Passive mechanisms are responsible for attenuating higher frequency components and include deformation of the shoe,heel fat pad,ligaments,bone,articular cartilage,and oscillation of soft tissue compartments.28,29Frequencies greater than 40 Hz are also attenuated by preactivation of muscle in preparation for ground contact.32Active shock attenuation mechanisms specifically responding to the impactstimulus and those thatoccur later in stance may be responsible for attenuating lower frequency components29,33and include eccentric muscle contractions,increased muscle activation,changes in segment geometry,and adjustments in joint stiffness.14,34—37When greater shock attenuation is required as a result of greater input energy,it is typically accomplished by active mechanisms such as increasing energy absorption by the muscles crossing the joints of the lower extrem ity.14Eccentric muscle contractions may be the primary mechanisms that attenuate forces transm itted through the body.30However,different segment and joint positions can affect the transmissibility of the impact shock and the primary mechanisms responsible for attenuation.26,34For example,increasing knee flexion may shift the degree of shock attenuation from passive tissue to muscular contractions by increasing the amount of knee extensor eccentric activity.15Muscle activity w ill affect joint stiffness which has also been shown to adjust in response to greater impact loading.32Results from previous studies investigating lower extrem ity joint compliance suggest that a compliant ankle is responsible for active shock attenuation during FF running more so than the knee whereas a compliant knee is responsible for active shock attenuation during RF running than the ankle.23,50Relying more on the knee than the ankle for shock attenuation may partially explain the greater shock attenuation observed w ith RF rather than FF running in the present study.
The differences in impact loading have been at the centerof the footfall pattern debate.A recent retrospective study1and a recent survey study2found that those who use an MF or FF pattern have fewer injuries than those who use an RF pattern. These authors and others have suggested that MF and FF running may reduce the risk of developing running related injuries as a result of reduced impact loading compared w ith RF running.1,24,48These studies were excellent fi rst steps toward furthering our know ledge of injury rates between footfall types.However,more research is needed given the lim itations of survey studies and that statistical significance was only found in the retrospective study when male and female data were combined.Additionally,speculating that the findings were a result of differences in impact parameters between footfall patterns was a logical conclusion given that many studies have found a relationship between impact parameters and the development of running related injuries(e.g., Refs.3—5).However,many other studies have not found this relationship(e.g.,Refs.6—8).Running injuries,regardless of footfallpattern,are the resultof a complex interaction of many variables in addition to impact loading,such as excessive joint excursion and moments,greater verticalGRF active peak,and muscle weakness.11,54Results from the present study may assist w ith understanding why different types of injuries may be more common w ith one footfall pattern than another by providing insight on potential tissues and mechanisms responsible for attenuating shock w ith each footfall pattern. The capacity and reliance of different tissues and mechanisms to attenuate impact shock may be frequency dependent.21
The primary frequency content of acceleration due to impact shock and segment motion during stance of each footfall pattern may alter the reliance on the mechanisms used for shock attenuation and how specific tissues adapt or are injured w ith each footfall pattern.The present study indicates that RF running may result in a greater reliance on passive mechanisms because the power of higher frequency components of the tibial acceleration signal was greater compared w ith FF running.Bone deformation may be the primary passive shock attenuation mechanism during any activity.30Several studies have shown that impact forces sim ilar to those experienced during RF running result in beneficial adaptations to bone,tendon,and muscle.55—57Damage to bone, articular cartilage,vertebral discs,and other passive tissues may result if they are overloaded,30,40,58and thus may be more at risk for injury from RF running.However,overload and injury also occur from MF and FF running1,55,56,59,60despite generating less impactenergy than RF running.Given that FF running does not make heel contact,it cannot take advantage of passive mechanisms like the heel fatpad or shoe cushioning in the heel to attenuate impact forces resulting from the collision w ith the ground.Therefore,the proportion of shock thatwould otherw ise be attenuated by these mechanisms must be applied to other tissues thatmay nothave the same capacity for shock attenuation.As a result,FF running may have a greater reliance on kinematics and eccentric contractions of the plantar flexors to sufficiently attenuate impacts thus a greater risk of injury to the tissues involved.For example,the muscles of the triceps surae may not be as effective as the quadriceps at changing muscle activity to increase frequency damping due to the smaller mass of the triceps surae.32The potential differences in the reliance of impact attenuation mechanisms between footfall patterns may have implicationson not only the risk of injury,but the tissues or joints that are susceptible to injury.
5.Conclusion
RF running resulted in greater impact loads and impact shock attenuation compared w ith FF running.Varying amounts of shock attenuation between footfallpatterns suggest that the body has the capacity to manage a range of impulsive loads in order to protect the head from excessive acceleration. The difference in impact shock frequency content between footfall patterns suggests that the primary mechanisms for attenuation may also differ.Although RF running may elicitan increased requirement of the body tissues to attenuate greater impulsive loads which may be detrimental,it is also possible that the tissues adapt to greater impulsive loads in a beneficial manner.However,the threshold between injury and adaptation is currently unknown.
1.Daoud AI,Geissler GJ,Wang F,Saretsky J,Daoud YA,Lieberman DE. Foot strike and injury rates in endurance runners:a retrospective study.Med Sci Sports Exerc2012;44:1325—34.
2.Goss DL,Gross MT.Relationships among self-reported shoe type,footstrike pattern,and injury incidence.US Army Med Dep J2012:25—30.
3.Hreljac A,Marshall RN,Hume PA.Evaluation of lowerextremity overuse injury potential in runners.Med Sci Sports Exerc2000;32:1635—41.
4.M ilner CE,Ferber R,Pollard CD,Hamill J,Davis IS.Biomechanical factors associated w ith tibial stress fracture in female runners.Med Sci Sports Exerc2006;38:323—8.
5.Zifchock RA,Davis IS,Ham ill J.Kinetic asymmetry in female runners w ith and w ithout retrospective tibial stress fractures.JBiomech2006;39:2792—7.
6.Azevedo LB,Lambert M I,Vaughan CL,O’Connor CM,Schwellnus MP. Biomechanicalvariables associated w ith achilles tendinopathy in runners.Br J Sports Med2009;43:288—92.
7.Bennell K,Crossley K,Jayarajan J,Walton E,Warden S,Kiss ZS,et al. Ground reaction forces and bone parameters in females w ith tibial stress fracture.Med Sci Sports Exerc2004;36:397—404.
8.Bredeweg S.No relationship between running related injuries and kinetic variables.Br J Sports Med2011;45:328.
9.Nigg BM,Cole GK,Bruggemann GP.Impact forces during heel toe running.J Appl Biomech1995;11:407—32.
10.Dickinson JA,Cook SD,Leinhardt TM.The measurementof shock waves follow ing heel strike while running.J Biomech1985;18:415—22.
11.Messier SP,Davis SE,Curl WW,Lowery RB,Pack RJ.Etiologic factors associated w ith patellofemoral pain in runners.Med Sci Sports Exerc1991;23:1008—15.
12.Radin EL.The physiology and degeneration of joints.Semin Arthritis Rheum1972;2:245—57.
13.Bobbert MF,Schamhardt HC,Nigg BM.Calculation of vertical ground reaction force estimates during running from positional data.J Biomech1991;24:1095—105.
14.Derrick TR,Ham ill J,Caldwell GE.Energy absorption of impacts during running at various stride lengths.Med Sci Sports Exerc1998;30:128—35.
15.Edwards WB,Derrick TR,Hamill J.Musculoskeletal attenuation of impact shock in response to knee angle manipulation.J Appl Biomech2012;28:502—10.
16.Hennig EM,Lafortune MA.Relationships between ground reaction force and tibial bone acceleration parameters.Int JSportsBiomech1991;7:303—9.
17.Shorten MR,W inslow DS.Spectral analysis of impact shock during running.Int J Sports Biomech1992;8:288—304.
18.Clarke TE,Cooper LB,Ham ill CL,Clark DE.The effectof varied stride rate upon shank deceleration in running.J Sports Sci1985;3:41—9.
19.Mercer JA,Vance J,Hreljac A,Ham ill J.Relationship between shock attenuation and stride length during running at different velocities.Eur J Appl Physiol2002;87:403—8.
20.Whittle MW.Generation and attenuation of transient impulsive forces beneath the foot:a review.Gait Posture1999;10:264—75.
21.Smeathers JE.Transient vibrations caused by heel strike.Proc Inst Mech Eng H1989;203:181—6.
22.Ham ill J,Derrick TR,Holt KG.Shock attenuation and stride frequency during running.Hum Mov Sci1995;14:45—60.
23.Laughton CA,Davis IS,Hamill J.Effectof strike pattern and orthotic intervention on tibialshock during running.J Appl Biomech2003;19:153—68.
24.Oakley T,Pratt DJ.Skeletal transients during heel and toe strike running and the effectiveness of some materials in their attenuation.Clin Biomech (Bristol,Avon)1988;3:159—65.
25.Pozzo T,Berthoz A,Lefort L,Vitte E.Head stabilization during various locomotor tasks in humans.Ii.Patients with bilateralperipheralvestibular defi cits.Exp Brain Res1991;85:208—17.
26.Lafortune MA,Lake M J,Hennig EM.Differential shock transm ission response of the human body to impact severity and lower limb posture.J Biomech1996;29:1531—7.
27.Cavanagh PR,Valiant GA,M iserich KW.Biological aspects of modelling shoe/footinteractions during running.In:Frederick EC,editor.Sports shoes and playing surfaces.Champaign,Illinois:Human Kinetics;1984.p.24—46.
28.Chu ML,Yazdani-Ardakani S,Gradisar IA,Askew MJ.Anin vitrosimulation study of impulsive force transm ission along the lower skeletal extremity.J Biomech1986;19:979—87.
29.Paul IL,Munro MB,Abernethy PJ,Simon SR,Radin EL,Rose RM. Musculo-skeletal shock absorption:relative contribution of bone and soft tissues at various frequencies.J Biomech1978;11:237—9.
30.Radin EL,Paul IL.Does cartilage compliance reduce skeletal impact loads?the relative force attenuating properties of articular cartilage,synovial fl uid,periarticular soft tissues and bone.Arthritis Rheum1970;13:139—44.
31.Simon SR,Radin EL,Paul IL,Rose RM.The response of joints to impact loading.II.invitrobehavior of subchondral bone.JBiomech1972;5:267—72.
32.Boyer KA,Nigg BM.Changes in muscle activity in response to different impact forces affect soft tissue compartment mechanical properties.J Biomech Eng2007;129:594—602.
33.Simon SR,Paul IL,Mansour J,Munro M,Abernethy PJ,Radin EL.Peak dynam ic force in human gait.J Biomech1981;14:817—22.
34.Cole GK,Nigg BM,van Den Bogert AJ,Gerritsen KG.The clinical biomechanics award paper 1995:lower extrem ity joint loading during impact in running.Clin Biomech(Bristol,Avon)1996;11:181—93.
35.M cMahon TA,Valiant G,Frederick EC.Groucho running.J Appl Physiol1987;62:2326—37.
36.Perry J.Kinesiology of lower extremity bracing.Clin Orthop Relat Res1974:18—31.
37.Perry SD,Lafortune MA.Influences of inversion/eversion of the footupon impact loading during locomotion.ClinBiomech(Bristol,Avon)1995;10:253—7.
38.Wakeling JM,Von Tscharner V,Nigg BM,Stergiou P.Muscle activity in the leg is tuned in response to ground reaction forces.J Appl Physiol2001;91:1307—17.
39.Voloshin A,Wosk J.Anin vivostudy of low back pain and shock absorption in the human locomotor system.J Biomech1982;15:21—7.
40.Voloshin A,Wosk J,BrullM.Force wave transm ission through the human locomotor system.J Biomech Eng1981;103:48—50.
41.Delgado TL,Kubera-Shelton E,Robb RR,Hickman R,Wallmann HW, Dufek JS.Effects of foot strike on low back posture,shock attenuation, and com fort in running.Med Sci Sports Exerc2013;45:490—6.
42.Gruber AH,Boyer K,Silvernail JF,Ham ill J.Comparison of classification methods to determ ine footfall pattern.Footwear Sci2013;5:S103—4.
43.Maclean CL,Davis IS,Ham ill J.Influence of running shoe m idsole composition and custom foot orthotic intervention on lower extremity dynam ics during running.J Appl Biomech2009;25:54—63.
44.Wosk J,Voloshin A.Wave attenuation in skeletons of young healthy persons.J Biomech1981;14:261—7.
45.Gillespie KA,Dickey JP.Determ ination of the effectiveness of materials in attenuating high frequency shock during gait using fi lterbank analysis.Clin Biomech(Bristol,Avon)2003;18:50—9.
46.Lafortune MA,Hennig EM.Cushioning properties of footwear during walking:accelerometer and force platform measurements.Clin Biomech (Bristol,Avon)1992;7:181—4.
47.Cohen J.A power primer.Psychol Bull1992;112:155—9.
48.Lieberman DE,Venkadesan M,Werbel WA,Daoud AI,D’Andrea S, Davis IS,et al.Foot strike patterns and collision forces in habitually barefoot versus shod runners.Nature2010;463:531—5.
49.Potthast W,Bruggemann GP,Lundberg A,Arndt A.The influences of impact interface,muscle activity,and knee angle on impact forces and tibial and femoral accelerations occurring after external impacts.J Appl Biomech2010;26:1—9.
50.Ham ill J,Gruber AH,Derrick TR.Lower extrem ity stiffness characteristics during running w ith different footfall patterns.Eur J Sports Sci2014;14:130—6.
51.Gruber AH,Davis IS,Ham ill J.Frequency contentof the vertical ground reaction force component during rearfoot and forefoot running patterns.Med Sci Sports Exerc(Suppl.)2011;43:S42.
52.Gruber AH,Umberger BR,Braun B,Hamill J.Economy and rate of carbohydrate oxidation during running w ith rearfoot and forefoot strike patterns.J Appl Physiol2013;115:194—201.
53.Ardigo LP,Lafortuna C,M inetti AE,Mognoni P,Saibene F.Metabolic and mechanical aspects of foot landing type,forefoot and rearfoot strike, in human running.Acta Physiol Scand1995;155:17—22.
54.Nicola TL,Jew ison DJ.The anatomy and biomechanics of running.Clin Sports Med2012;31:187—201.
55.Rosager S,Aagaard P,Dyhre-Poulsen P,Neergaard K,K jaer M, Magnusson SP.Load displacement properties of the human triceps surae aponeurosis and tendon in runners and nonrunners.Scand J Med Sci Sports2002;12:90—8.
56.Grimston SK,Willows ND,Hanley DA.Mechanical loading regime and its relationship to bone m ineraldensity in children.Med Sci Sports Exerc1993;25:1203—10.
57.Stone J,Brannon T,Haddad F,Qin A,Baldw in KM.Adaptive responses of hypertrophying skeletal muscle to endurance training.J Appl Physiol1996;81:665—72.
58.Burr DB,M ilgrom C,Fyhrie D,Forwood M,Nyska M,Finestone A,etal.In vivomeasurementof human tibialstrains during vigorous activity.Bone1996;18:405—10.
59.Ridge ST,Johnson AW,M itchell UH,Hunter I,Robinson E,Rich BS, et al.Foot bone marrow edema after a 10-wk transition to m inimalist running shoes.Med Sci Sports Exerc2013;45:1363—8.
60.Salzler MJ,Bluman EM,Noonan S,Chiodo CP,de Asla RJ.Injuries observed in m inimalist runners.Foot Ankle Int2012;33:262—6.
Received 10 September 2013;revised 2 February 2014;accepted 10 March 2014
*Corresponding author.
E-mail address:jhamill@kin.umass.edu(J.Hamill)
Peer review under responsibility of Shanghai University of Sport.
2095-2546/$-see front matter CopyrightⒸ2014,Shanghai University of Sport.Production and hosting by Elsevier B.V.A ll rights reserved. http://dx.doi.org/10.1016/j.jshs.2014.03.004
 Journal of Sport and Health Science2014年2期
Journal of Sport and Health Science2014年2期
- Journal of Sport and Health Science的其它文章
- Can m inimal running shoes im itate barefoot heel-toe running patterns? A comparison of lower leg kinematics
- The effect of m inimal shoes on arch structure and intrinsic foot muscle strength
- Strike type variation among Tarahumara Indians in m inimal sandals versus conventional running shoes
- Foot strike patterns and hind limb joint angles during running in Hadza hunter-gatherers
- Muscle activity and kinematics of forefoot and rearfoot strike runners
- The effectof shoe type on gait in forefootstrike runners during a 50-km run