
发育不良性髋关节脱位诊断、分型和手术
2013-09-12 13:20:00杨述华刘先哲
中华骨与关节外科杂志 2013年1期
杨述华 刘先哲
(华中科技大学同济医学院附属协和医院骨科,武汉 430022)
髋关节发育不良(developmental dysplasia of the hip,DDH)是年轻患者髋关节骨性关节炎的一个主要病因。在这些患者发展到终末期骨性关节炎之前,有几种非关节置换的手术方式可以考虑,包括股骨近端和髋臼周围截骨术。但是在DDH发展至终末期骨性关节炎,引起严重的疼痛和功能受限时,全髋关节置换术则是标准的治疗方式。与正常髋关节相比,发育不良的髋关节异常的接触应力容易诱发髋关节骨性关节炎。对于DDH患者行全髋关节置换术(THA)时需要考虑许多因素,包括患者的年龄,畸形的解剖结构,以及文献报道的高失败率和翻修率等。1
解剖特征
尽管每个DDH患者都有独特的解剖结构,但对于髋臼和股骨近端的解剖特征都有很好的描述。髋臼常见前侧和上方的缺损,而股骨近端常见前倾角增大,髓腔变细,直线轮廓,髋内翻或外翻。近来CT研究证明发育不良的股骨均表现为前倾角增大,股骨颈变短,髓腔变细,并且发育不良的程度越严重,股骨前倾角越大。减小的髓腔直径和更细的皮质厚度也使得发育异常的髋关节易于骨折。因此,在为DDH患者实施THA之前要特别注意每位患者的解剖特点。
对于DDH患者,软组织的因素也要考虑。严重的DDH患者常常合并外展肌群的肌力减退,导致跛行甚至trendelenburg步态。由于慢性关节脱位,髋关节内收肌群、屈肌群和伸肌群的肌肉萎缩。如果肢体延长大于3 cm,坐骨神经也很容易损伤。据文献报道,THA治疗髋关节发育不良时坐骨神经麻痹的发生率5.2%~13%。
2外展肌的平衡降低,降低步态效率,导致跛行。由于异常的生物力学包括髋臼缘负荷过重,常常继发骨性关节炎,最终导致疼痛和功能受限。放射学检查可以确认诊断,明确髋臼和股骨近端解剖异常的特点。
DDH患者的放射学检查对于手术方案的确定非常重要。标准的放射学检查包括骨盆的正位片和髋关节的侧位片,这可以在正侧位上反映髋臼对股骨头包容性情况。中心边缘角,即在骨盆正位片上,通过股骨头的中心垂直线和通过股骨头中心和髋臼侧缘连线之间的角度,通常>25°。垂直中心前角,即在髋关节侧位片上,通过股骨头的中心垂直线和通过股骨头中心和髋臼前缘连线之间的角度,通常>25°。通过骨盆正位片也可以评估股骨近端的颈干角。CT有助于评估髋臼的骨量情况和前倾角。
DDH的分型有助于手术方案的制定。其中,最常用的分型标准是Crowe等根据股骨头从髋臼脱位的严重程度分型。Ⅰ型:股骨头半脱位,脱位率<50%(图1);Ⅱ型:股骨头半脱位,脱位率50%~75%(图2);Ⅲ型:股骨头半脱位,脱位率75%~100%(图3);Ⅳ型:股骨头全脱位,脱位率>100%(图4)。这种分型标准可以用于指导THA术中髋臼重建。
Hartofilakidis分型将DDH分为三类:股骨头在真臼中;股骨头低脱位,在假臼中,假臼与真臼部分
2 DDDDHH的诊断和分型
DDH常见于年轻患者,起病隐袭,表现为腹股沟区的疼痛或髋关节痛。许多患者有下肢不等长,而跛行是最常见的功能障碍。髋关节高脱位的患者髋关联;股骨头高脱位,股骨头不在真臼及假臼中。许多外科医生认为这种分型更有助于指导手术。

图1 Ⅰ型:股骨头半脱位,脱位率<50%,股骨头仍在真臼中

图2 Ⅱ型:股骨头半脱位,脱位率50%~75%

图3 Ⅲ型:股骨头半脱位,脱位率75%~100%

图4 Ⅳ型:股骨头全脱位,脱位率>100%
3 不同方法全髋置换手术要点
标准的手术入路包括髋关节前侧入路、前外侧入路以及后侧入路。对于严重的髋关节发育不良,伴股骨头半脱位的患者,后侧入路更有利于股骨头和髋臼的充分暴露。此外,对于严重的髋关节发育不良,往往需要转子下短缩截骨术,以扩展股骨近端,充分暴露髋关节后侧。
3.1 髋臼重建
CroweⅠ型的髋关节,髋臼假体通常直接放置于真臼中。其臼杯可以与髋臼有充分的骨接触。Garvin等[13]指出髋臼外上方大约20%的不接触不会增加手术失败的风险。对于CroweⅠ型的髋关节,骨水泥型和压配型的臼杯假体都可以考虑,骨水泥型似乎有更高的机械失败率。
CroweⅡ型和Ⅲ型髋臼外上方的骨缺损造成了臼杯的不充分骨接触,影响臼杯假体的安放。这些是髋关节重建中最常见的问题。特殊的假体,小髋臼杯可以解决髋臼假体骨接触不足的问题。髋臼缺损可以通过下面的几种方法改善:①通过骨块在髋关节的解剖中心重建髋臼(图5);②在假臼外侧重建髋臼(图6);③结构性骨移植重建髋臼加网杯重建髋臼(图7)。通过骨块重建髋臼,臼杯有更多的解剖位置,在未来翻修手术中髋关节也有更多的骨量。
使用大块的股骨头自体移植是一种有效的方法,髋臼骨缺损的部位提供了一个良好的有血供的植骨床,而且股骨头的松质骨部分可以很好的塑形以匹配髋臼缺损,并由两枚或更多的螺钉固定在髂骨上。为了预防移植物的机械失败,Mulroy和Harris指出,宿主骨对髋臼杯的骨接触应大于70%。
CroweⅣ型髋关节,同样是髋臼发育不良,但是其髋臼上方的缺损并不比CroweⅡ~Ⅲ型髋关节更严重。因此,可以选择在髋关节解剖中心放置一个较小的非骨水泥型臼杯。通常并不需要骨块移植。
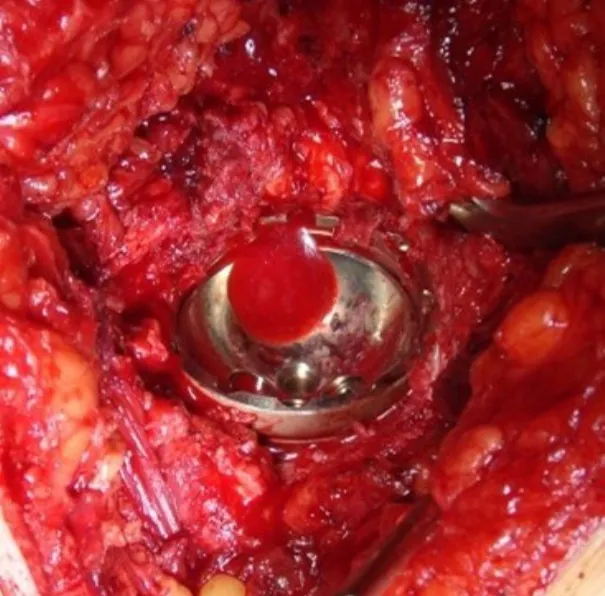
图5 自体股骨头髋关节解剖中心重建髋臼
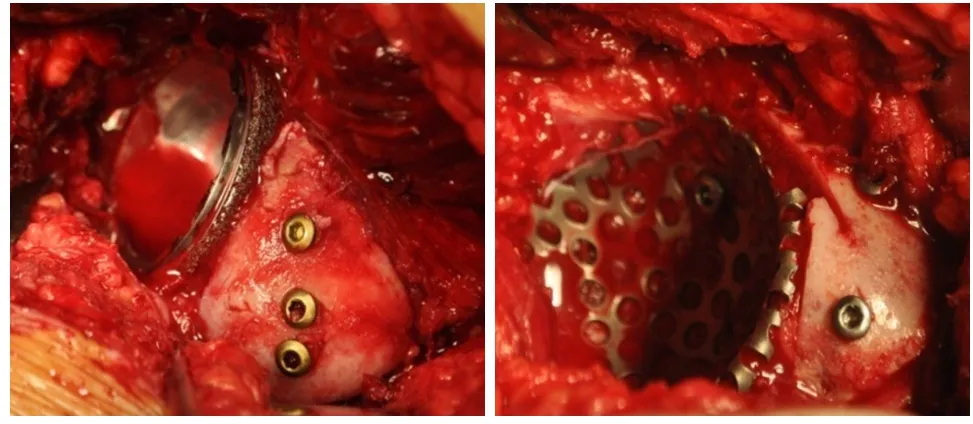
图6 在假臼外侧重建髋臼

图7 结构性骨移植重建髋臼加网杯重建髋臼
3.2 股骨重建
CroweⅠ~Ⅱ型髋关节,不需要股骨短缩截骨来将股骨端放置于髋关节解剖中心的安全位置。由于髓腔较窄以及股骨前倾角,可以使用DDH特殊的细柄,包括骨水泥型及非骨水泥型假体柄。细柄骨水泥型假体柄可以控制前倾角;如果选用非骨水泥型的压配型假体,术者必须注意避免前倾角过大,因为股骨本身存在一定的前倾角。
全髋关节置换术可以成功地治疗伴有关节疼痛和活动障碍的成人先天性髋关节高脱位患者。CroweⅢ型髋关节,股骨重建的原则与CroweⅠ~Ⅱ型髋关节相同。然而,这个技术要求高,且并发症发生率高。高脱位的股骨头必须被复位至真臼,髋关节的作用力降低,改善外展力臂,延长髋臼假体的使用寿命。当髋臼杯置入假臼中,由于外展肌群松弛Trendelenburg步态和肢体不等长不能得到纠正。当髋臼杯置入真髋臼,由于肌肉紧张和神经损伤的风险,髋关节复位几乎不可能。为克服这些困难,两种技术应运而生:①髂股牵引逐步延长肢体(图8),②股骨短缩截骨术(图9)。由于前者仅应用于少数或单侧病例,股骨短缩截骨术便成为治疗成人先天性髋关节高脱位的标准方法。
在某些情况下,如果重建髋关节解剖中心,也可能需要股骨短缩截骨。股骨短缩截骨在CroweⅣ型髋关节中的应用更为常见。
Anwar等报道通过股骨近端短缩截骨29%的患者骨不连,Trendelenburg步态的频率增加。因此,近来更推荐选择转子下截骨术,能够维持外展肌群的稳定并纠正旋转畸形。
短中期的随访研究表明,对于CroweⅣ型髋关节发育不良患者,通过转子下股骨短缩截骨术,并使用非骨水泥型股骨假体柄,髋关节解剖中心重建,术后骨愈合率较好。总的研究结果表明随访14年,生存率为75%,通过转子下截骨并股骨假体重建后,Harris髋关节评分较术前改善。而使用新一代的高交联聚乙烯内衬长期的随访结果尚待研究。

图8 髂股牵引逐步延长肢体

图9 转子下截骨及固定和股骨近端短缩截骨X线片
[1]Sanchez-Sotelo J,Trousdale RT,Berry DJ,et al.Surgical treatment of developmental dysplasia of the hip in adults:I.Nonarthroplasty options.J Am Acad Orthop Surg,2002,10(5):321-333.
[2]Sanchez-Sotelo J,Berry DJ,Trousdale RT,et al.Surgical treatment of developmental dysplasia of the hip in adults:II.Arthroplasty options.J Am Acad Orthop Surg,2002,10(5):334-344.
[3]Brand RA.Hip osteotomies:a biomechanical consideration.JAmAcad Orthop Surg,1997,5(5):282-291.
[4]Argenson JN,Flecher X,Parratte S,et al.Anatomy of the dysplastic hip and consequences for total hip arthroplasty.Clin Orthop Relat Res,2007,465:40-45.
[5]Engesaeter LB,Furnes O,Havelin LI.Developmental dysplasia of the hip--good results of later total hip arthroplasty:7135 primary total hip arthroplasties after developmental dysplasia of the hip compared with 59774 total hip arthroplasties in idiopathic coxarthrosis followed for 0 to 15 years in the Norwegian Arthroplasty Register.J Arthroplasty 2008,23:235-240.
[6]Noble PC,Kamaric E,Sugano N,et al.Three-dimensional shape of the dysplastic femur:implications for THR.Clin Orthop Relat Res,2003,417:27-40.
[7]Perka C,Fischer U,Taylor WR,et al.Developmental hip dysplasia treated with total hip arthroplasty with a straight stem and a threaded cup.J Bone Joint Surg Am,2004,86-A:312-319.
[8]Lewallen DG.Neurovascular injury associated with hip arthroplasty.Instr Course Lect,1998,47:275-283.
[9]Nunley RM,Prather H,Hunt D,et al.Clinical presentation of symptomatic acetabular dysplasia in skeletally mature patients.J Bone Joint SurgAm,2011,93 Suppl 2:17-21.
[10]Delaunay S,Dussault RG,Kaplan PA,et al.Radiographic measurements of dysplastic adult hips.SkeletalRadiol,1997,26:75-81.
[11]Crowe JF,Mani VJ,Ranawat CS.Total hip replacement in congenital dislocation and dysplasia of the hip.J Bone Joint SurgAm,1979,61:15-23.
[12]Hartofilakidis G,Stamos K,Karachalios T,et al.Congenital hip disease in adults.Classification of acetabular deficiencies and operative treatment with acetabuloplasty combined with total hip arthroplasty.J Bone Joint Surg Am,1996,78:683-692.
[13]Garvin KL,Bowen MK,Salvati EA,et al.Long-term results of total hip arthroplasty in congenital dislocation and dysplasia of the hip.A follow-up note.J Bone Joint Surg Am,1991,73:1348-1354.
[14]Mulroy RD,Harris WH.Failure of acetabular autogenous grafts in total hip arthroplasty.Increasing incidence:a follow-up note.J Bone Joint SurgAm,1990,72:1536-1540.
[15]Morsi E,Garbuz D,Gross AE.Total hip arthroplasty with shelf grafts using uncemented cups.A long-term follow-upstudy.JArthroplasty,1996,11:81-85.
[16]Gross AE,Catre MG.The use of femoral head autograft shelf reconstruction and cemented acetabular components in the dysplastic hip.Clin Orthop Relat Res,1994,298:60-66.
[17]Gerber SD,Harris WH.Femoral head autografting to augment acetabular deficiency in patients requiring total hip replacement.A minimum five-year and an average seven-year follow-up study.J Bone Joint Surg Am,1986,68:1241-1248.
[18]Kim M,Kadowaki T.High long-term survival of bulk femoral head autograft for acetabular reconstruction in cementless THA for developmental hip dysplasia.Clin Orthop Relat Res,2010,468:1611-1620.
[19]Rodriguez JA,Huk OL,Pellicci PM,et al.Autogenous bone grafts from the femoral head for the treatment of acetabular deficiency in primary total hip arthroplasty with cement.Long-term results.J Bone Joint Surg Am,1995,77:1227-1233.
[20]Dorr LD,Tawakkol S,Moorthy M,et al.Medial protrusio technique for placement of a porous-coated,hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia.J Bone Joint SurgAm,1999,81:83-92.
[21]Linde F,Jensen J.Socket loosening in arthroplasty for congenital dislocation of the hip.Acta Orthop Scand,1988,59:254-257.
[22]Stans AA,Pagnano MW,Shaughnessy WJ,et al.Resultsof total hip arthroplasty for Crowe Type III developmental hip dysplasia.Clin Orthop Relat Res,1998,348:149-157.
[23]Delp SL,Wixson RL,KomattuAV,et al.How superior placement of the joint center in hip arthroplasty affects the abductor muscles.Clin Orthop Relat Res,1996,328:137-146.
[24]Kaneuji A,Sugimori T,Ichiseki T,et al.Minimum ten-year results of a porous acetabular component for Crowe I to III hip dysplasia using an elevated hip center.J Arthroplasty,2009,24:187-194.
[25]Krych AJ,Howard JL,Trousdale RT,et al.Total hip arthroplasty with shortening subtrochanteric osteotomy in Crowe type-IV developmental dysplasia:surgical technique.J Bone Joint SurgAm,2010,92 Suppl 1 Pt 2:176-187.
[26]Thillemann TM,Pedersen AB,Johnsen SP,et al.Implant survival after primary total hip arthroplasty due to childhood hip disorders:results from the Danish Hip Arthroplas-ty Registry.Acta Orthop,2008,79:769-776.
[27]Charnley J,Feagin JA.Low-friction arthroplasty in congenital subluxation of the hip.Clin Orthop Relat Res,1973,91:98-113.
[28]Boyle MJ,Frampton CM,Crawford HA.Early results of total hip arthroplasty in patients with developmental dysplasia of the hip compared with patients with osteoarthritis.J Arthroplasty,2012,27:386-390.
[29]MacKenzie JR,Kelley SS,Johnston RC.Total hip replacement for coxarthrosis secondary to congenital dysplasia anddislocation of the hip.Long-term results.J Bone Joint SurgAm,1996,78:55-61.
[30]Sochart DH,Porter ML.The long-term results of Charnley low-friction arthroplasty in young patients who have congenital dislocation,degenerative osteoarthrosis,or rheumatoid arthritis.J Bone Joint SurgAm,1997,79:1599-1617.
[31]Numair J,Joshi AB,Murphy JC,et al.Total hip arthroplasty for congenital dysplasia or dislocation of the hip.Survivorship analysis and long-term results.J Bone Joint Surg Am,1997,79:1352-1360.
[32]Silber DA,Engh CA.Cementless total hip arthroplasty with femoral head bone grafting for hip dysplasia.J Arthroplasty,1990,5:231-240.
[33]Lee BP,Cabanela ME,Wallrichs SL,et al.Bone-graft augmentation for acetabular deficiencies in total hip arthroplasty.Results of long-term follow-up evaluation.J Arthroplasty,1997,12:503-510.
[34]Schutzer SF,Harris WH.High placement of porous-coated acetabular components in complex total hip arthroplasty.J Arthroplasty,1994,9:359-367.
[35]Russotti GM,Harris WH.Proximal placement of the acetabular component in total hip arthroplasty.A long-term follow-up study.J Bone Joint SurgAm,1991,73:587-592.
[36]KlapachAS,Callaghan JJ,Miller KA,et al.Total hip arthroplasty with cement and without acetabular bone graft for severe hip dysplasia.A concise follow-up,at a minimum of twenty years,of a previous report.J Bone Joint Surg Am,2005,87:280-285.
[37]Kim YH.The results of a proximally-coated cementless femoral component in total hip replacement:a five-to 12-year follow-up.J Bone Joint Surg Br,2008,90:299-305.
[38]Hallan G,Lie SA,Furnes O,et al.Medium-and long-term performance of 11,516 uncemented primary femoral stems from the Norwegian arthroplasty register.J Bone Joint Surg Br,2007,89:1574-1580.
[39]Mortazavi SM,Restrepo C,Kim PJ,et al.Cementless femoral reconstruction in patients with proximal femoral deformity.JArthroplasty,2011,26:354-359.
[40]Anwar MM,Sugano N,Masuhara K,et al.Total hip arthroplasty in the neglected congenital dislocation of the hip.A five-to 14-year follow-up study.Clin Orthop Relat Res,1993,295:127-134.
[41]Krych AJ,Howard JL,Trousdale RT,et al.Total hip arthroplasty with shortening subtrochanteric osteotomy in Crowe type-IV developmental dysplasia.J Bone Joint Surg Am,2009,91:2213-2221.
[42]Bernasek TL,Haidukewych GJ,Gustke KA,et al.Total hip arthroplasty requiring subtrochanteric osteotomy for developmental hip dysplasia:5-to 14-year results.J Arthroplasty,2007,22:145-150.
[43]Biant LC,Bruce WJ,Assini JB,et al.Primary total hip arthroplasty in severe developmental dysplasia of the hip.Ten-year results using a cementless modular stem.J Arthroplasty,2009,24:27-32.
猜你喜欢
疯狂英语·新读写(2023年5期)2023-06-02 02:05:02
疯狂英语·新读写(2023年1期)2023-04-06 01:26:32
中华骨与关节外科杂志(2022年1期)2022-08-31 09:18:48
基层中医药(2022年1期)2022-07-22 07:22:16
基层中医药(2018年3期)2018-05-31 08:52:11
中华骨与关节外科杂志(2017年1期)2017-05-17 06:11:24
中华骨与关节外科杂志(2016年6期)2016-05-17 06:11:13
中华骨与关节外科杂志(2016年6期)2016-05-17 06:11:09
中华骨与关节外科杂志(2016年5期)2016-05-17 06:11:01
中华骨与关节外科杂志(2016年5期)2016-05-17 06:10:53
