Aortic valved stent designed without influence on coronary artery
2013-05-16 06:23:54,,,,
外科研究与新技术 2013年4期
,,,,
Deptartment of Cardiovascul Surgery,Tongji Hospital of Tongji university,Shanghai 200065,China
Aortic valved stent designed without influence on coronary artery
CAI Jian-zhi,ZHOU Yong-xin,SHAO Jie,MEI Yun-qing,WANG Yong-wu
Deptartment of Cardiovascul Surgery,Tongji Hospital of Tongji university,Shanghai200065,China
ObjectiveTo evaluated feasibility and safety of a new type of aortic valved stent in transcatheter aortic valve implantation(TAVI)using retrograde approach by testing and animal implantationin vitro.MethodsFirstly,a new type of aortic valve stent sutured with porcine pericardium valves was made.The fluid passing test,expanding and releasing tests,static and releasing tests in tube were peformedin vitrofor all stents.Then,the stents were implanted in six pigs using retrograde approach.These pigs were euthanized 12 h after implantation for anatomic evaluation.ResultsIn vitrothe tests showed that closure of new type of aortic valved stent leaflets were effective,and stents could be released through catheter,then expanded completely and could fix fast in tube.Left and right coronary artery flow rates did not change significantly when the stents were released above valve leaflets(P=0.7426,P=0.1487)after implantation.In vivoexperiments indicated that TAVI was successfully performed in six pigs using retrograde approach.However,one pig died 10h after implantation because stents were not expanded completely.The leaflets in stents opened well and no valvular regurgitation was observed in the rest five pigs.And no thrombosis was found.ConclusionThe new type of aortic valved stent designed in this study was characterised with good stability and could avoid the impact caused by valve leaflets on the coronary artery.
Aortic valved stent;Transcatheter aortic valve implantation;Retrograde
Introduction
Cardiovascular disease(CVD)is one of the most common diseases affecting health care systems and is considered to be the main cause of death worldwide,about 7.25 million deaths per year according to the report from World Health Organization[1,2].Meanwhile,it is very important to diagnose and treat the diseases of aortic valve for the aortic valve disease has a high incidence and serious threats to the health and life of people.Otherwise,untreated aortic valve disease may eventually result in heart failure,severe infection,and even a sudden death[3].
Currently,one of the prevalent cardiac operations and standard therapies for aortic valve disease is chestopened surgical aortic valve replacement which has mature procedures and good effects[4].However,surgical aortic valve replacement has some defects,such as severe trauma,extracorporeal circulation,long recovery time and long-term anticoagulation.Since symptomatic aortic valve stenosis usually occurs in the elderly,a high prevalence of comorbidities is present in these patients. What’s more, the common comorbidities including advanced age,previous cardiac surgery,leftventriculardysfunction,heartfailure,pulmonary disease and renal insufficiency are known to be related with a high periprocedural and postprocedural risk of mortality and morbidity of the patients[5,6].And almost one third of aortic valve stenosis patients with these comorbidities are not referred to or are rejected for surgery[7,8].Therefore,it is still a great challenge for medical technicians to treat the aortic valve patients with high risk effectively.
The technology oftranscatheteraortic valve implantation(TAVI)was first reported by Anderson et al.A new artificial aortic valve prosthesis prepared by mounting a porcine aortic valve into an expandable stent was developed for implantation by transluminal catheter technique without thoracotomy or extracorporal circulation indicates that artificial aortic valves can be implanted in closed chest animals by transluminal catheter technique[9].And Cribier et al reported the first human implantation performed in a 57-year-old man with calcific aortic stenosis and many noncardiac diseases concerned[10]. Percutaneously implanted heart valve was successfully implanted within the diseased native aortic valve,with accurate and stable positioning,without impairment of coronary artery blood flow or mitral valve function,and a mild paravalvular aortic regurgitation.
Though the success rate and curative effect for TAVI is gradually increasing,the mortality rate of high-risk patients may still account for approximately 20% within 30 days after the surgery[4,11,12].However,TAVI has a series of advantages,such as minimally invasion,less physical damage and rapid postoperative recovery.Therefore,TAVI has good development and applicable prospects especially in high-risk patiens who have contraindicationsfor surgical aortic valve replacement and it is increasingly being used to treat severe aortic stenosis in patients with high operative risk[13,14].Despite the fact that TAVIhasentered the mainstream asa viable treatment option for patients with symptomatic,severe aortic stenosis who are at prohibitively high surgical risk,there are still many problems associated with stent implantation including exact valve positioning,risk of coronary artery obstruction,disorder of mitral valve function and risk of paravalvular leak[15-17].Hence there is a definite need for continued development and refinementwith regardsto the application of TAVI.
In our study,a new type of aortic valve stent was made according to the anatomy parameters of porcine aortic rootand porcine pericardium valveswere sutured with the distal end of self-expandable stent.We evalute the feasibility,safety and efficacy of the new type ofaortic valve stentin TAVIusing retrograde implantation approach by testing and animal implantation studiesin vitro.
Materials and Methods
Animal preparation
A total of six healthy adult pigs(Fig.1A)of either gender weighing 15-21 kg were enrolled(Songjiang Experimental Animal Field,Shanghai,China).The study was performed after the pigs were allowed to acclimate for 1 week in the Animal Experiment Center of Tongji University.Anesthesia was initiated by intramuscular injection of ketamine(10mg/kg,JiangsuHengruiMedicalCo.Ltd,China),followed by intravenous injection of 10 ml of 2.5% pentobarbital sodium(Sinopharm Chemical Reagent Co.Ltd,China).Animal care and use was in accordance with the guidelines established by the Animal Ethics Committee of Tongji University.
Manufacture of the new type of aortic valved stent
The aortic inner diameter of experimental pig was shown in Fig.1B.The module of aortic valved stent(Fig.2A)was made with diameter of 20 -26 mm according to anatomy parameters and morphological characteristics of porcine aortic root.The self-expandable stent with diameter of 20-26mm was made by 0.2mm Ni-Ti shape memory alloy(Electric Titanium Factory of Jintai in Baoji City,Shaanxi,China)according to the method of sine curve.And the manufacture of self-expandable stent was accomplished(Fig.2B,C)after procedures of heat treatment,heat setting(400 -500℃,twice),acid pickling,cleaning,drying and inspection.
Freshporcine pericardium(Songjiang Experimental Animal Field,Shanghai,China)with uniform thickness and fiberwasselected and immersed in 0.6%glutaraldehyde for 36h(pH=7.4)after acellular disposalby 0.01% trypsin solution.Then,the decellularized pericardium was immersed in 2% L-glutamic acid solution for 24 h to remove toxicity of glutaraldehyde and sutured with the distal end of selfexpandable stent by 6-0 PROLENE(Shanghai Pudong Jinhuan Medical Products Co.Ltd,China).The stents were placed in the fixing solution for one day after the sinus of the valve were pressed with medical cotton balls.Then,the manufactured novel aortic valved stents(Figure 2D,E)were preserved in 70%ethanol and rinsed with physiological saline 3 times before use.
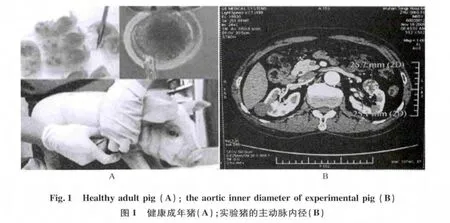
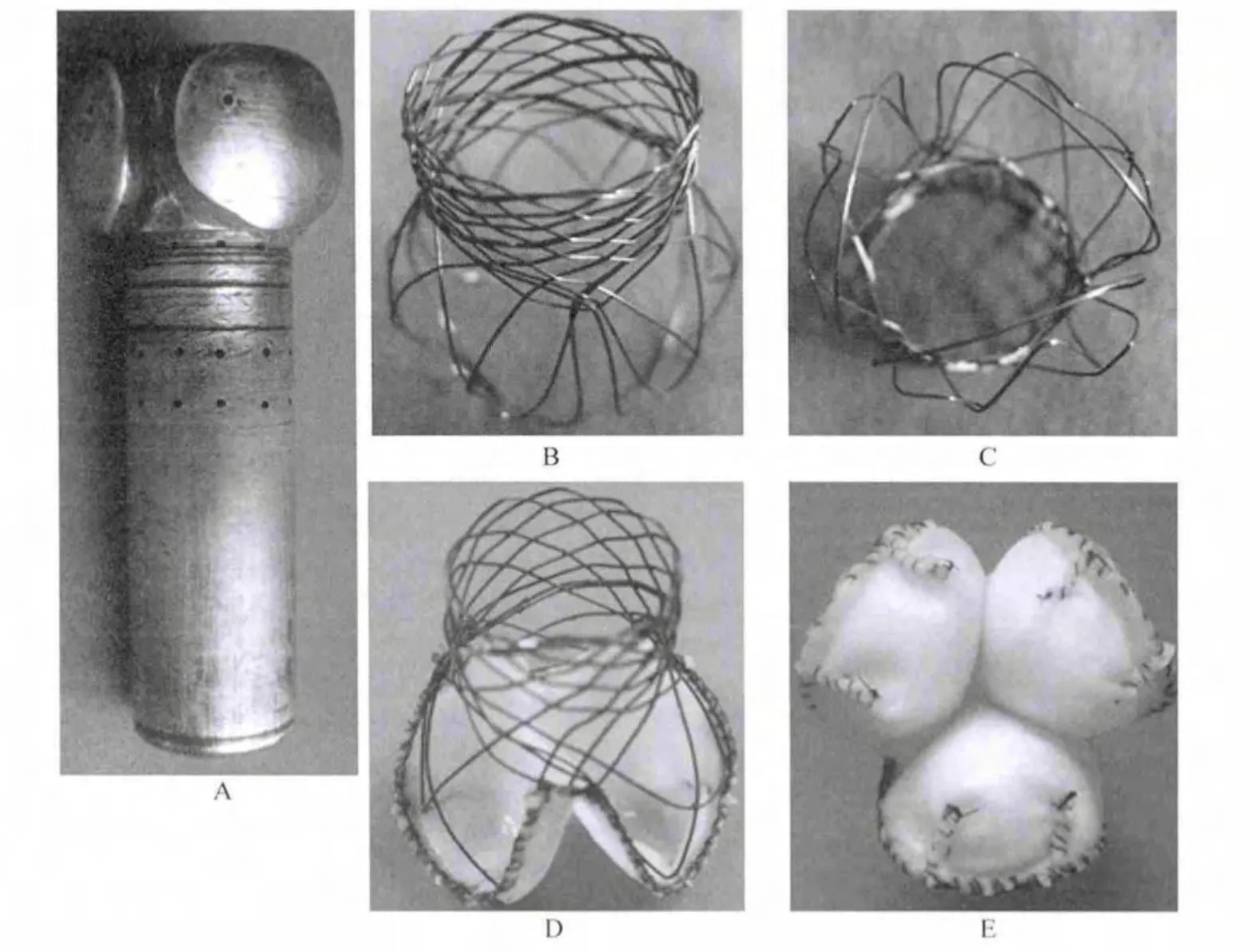
Fig.2 Module of aortic valved stent(A);side view of the self-expandable stent(B);top view of the self-expandable stent(C);side view of the valved stent(D);top view of the valved stent(E)图2 主动脉瓣膜支架,A:侧面观(展开后);B:顶观(展开后);C:侧面观;D:顶观
Performance of aortic valved stents in vitro
The valved stents were delivered to left ventricle of the isolated heart from 3-4 months old miniature pig(Songjiang Experimental Animal Field,Shanghai,China)via ascending aorta and placed in the aortic valve.Then,the aortic valved stents were released and water was injected to observe the valvular competence and coronary flow rates.
The fluid passing test,expanding and releasing tests,static and releasing tests in tube were peformed for all valved stents by Sarns 5 200 extracorporeal circulation at 40 - 120 mmHg(Sarns,America).In the fluid passing test, the closure, open and regurgitation of all valved stents were observed when uniform flow rushed to the stents in the opposite or same direction.In the expanding and releasing tests,the valved stents were released into physiological saline at 37℃.Then,the expanding degree and rate were observed.For static and releasing tests,polyvinyl chloride(PVC)tube(Shanghai Xiangsheng Medical Instrument Co.Ltd,China)whose inner diameter was matched that of the valved stent was selected.The stents were implanted in the tube by simulating TAVI at 37℃ (thermostatic water tank,Sarns,America)via a catheter(Shanghai Pujiang Medical New Material Co.Ltd,China).The tube was filled with water continuously and filling stopped when the height of water surface was up to 150cm.The fixation,flow direction,leakage,degree of closure and open of valved stents were observed.
Implantion of aortic valved stents in vivo
The experimental pigs were placed on Model JL-1A operating table(Medical Equipment Factory of Shanghai Medical Instruments Co.Ltd,China)with supine position and hair was removed from the precordial region.After the skin of inguinal region was sterilized,a 5 cm incision was made through the right inguinal skin and subcutaneous tissue.Then,the right femoral artery was subsequently exposed and punctured with a 7-French(F)leak-proof sheath.Heparin(100 U/kg,Sinopharm Chemical Reagent Co.Ltd,China)was introduced via the sheath.A 6F pigtail catheter was introduced through the right femoral artery sheath,and imaging of the left ventricle was performed by using digital subtraction angiography(DSA)apparatus(GE,America).The radiography of valved stent in the ascending aorta was shown in Fig.4.
Then,the positions of aortic valve and coronary artery were identified according to the imaging results.After the inner diameter of ascending aorta was measured,the aortic valve was punctured.A balloon catheter(4.0 ×15 mm)was placed in the crevasse of the aortic valve via a steel guide wire(2.5 m).The balloon catheter was pushed out after the crevasse of the aortic valve was enlarged by compressing the balloon dilator.The ascending aortic angiography was performed to confirm the aortic valve incompetence and echocardiography was conducted to measure regurgitant volume.
New type of aortic valved stents with size of 2 cm larger than the measured ascending aorta were selected.The delivery route was established by introducing a steel guide wire into the left ventricle via pigtail catheter.After pigtail catheter was removed,a12 - 16F delivery sheath with an expandable stub was deployed into the ascending aorta at the top of the coronary artery via a guide wire.The expandable stub and steel guide wire were then removed and 14F sheath carrying the valve stent was connected with the delivery sheath.The stent was inserted into the delivery sheath positioned under DSA apparatus to the previously marked position of the ascending aorta.After it was confirmed that the stent had been delivered to the optimalposition,the delivery sheath was retracted to release the stent.The delivery sheath was subsequently removed and right femoral artery was sutured.
Then,echocardiography and ascending aortic angiography were performed to observe aortic valvular regurgitation by deploying a pigtail catheter via the left femoral artery.The catheter and right femoral artery sheath were removed.Allpigs received postoperative intramuscular injections ofpenicillin(80 000 000 U,North China Pharmaceutical Co.Ltd)and subcutaneous injections of heparin(2 500 IU).Statistical analysis
Statistical analysis was performed by the SPSS version 12.0 statistical software.The measurement data were expressed as mean±standard deviation and analyzed by T-test.There is significantly statistical difference whenP<0.05.
Results
Properties of aortic valved stents in vitro
In vitrotests,the closure of the valved stent leaflets were effective,and all fluid flows were not restricted in the opposite direction.The valved stents could be rcleased through catheter,then expanded completely and could fix fast in the tube(Fig.3).
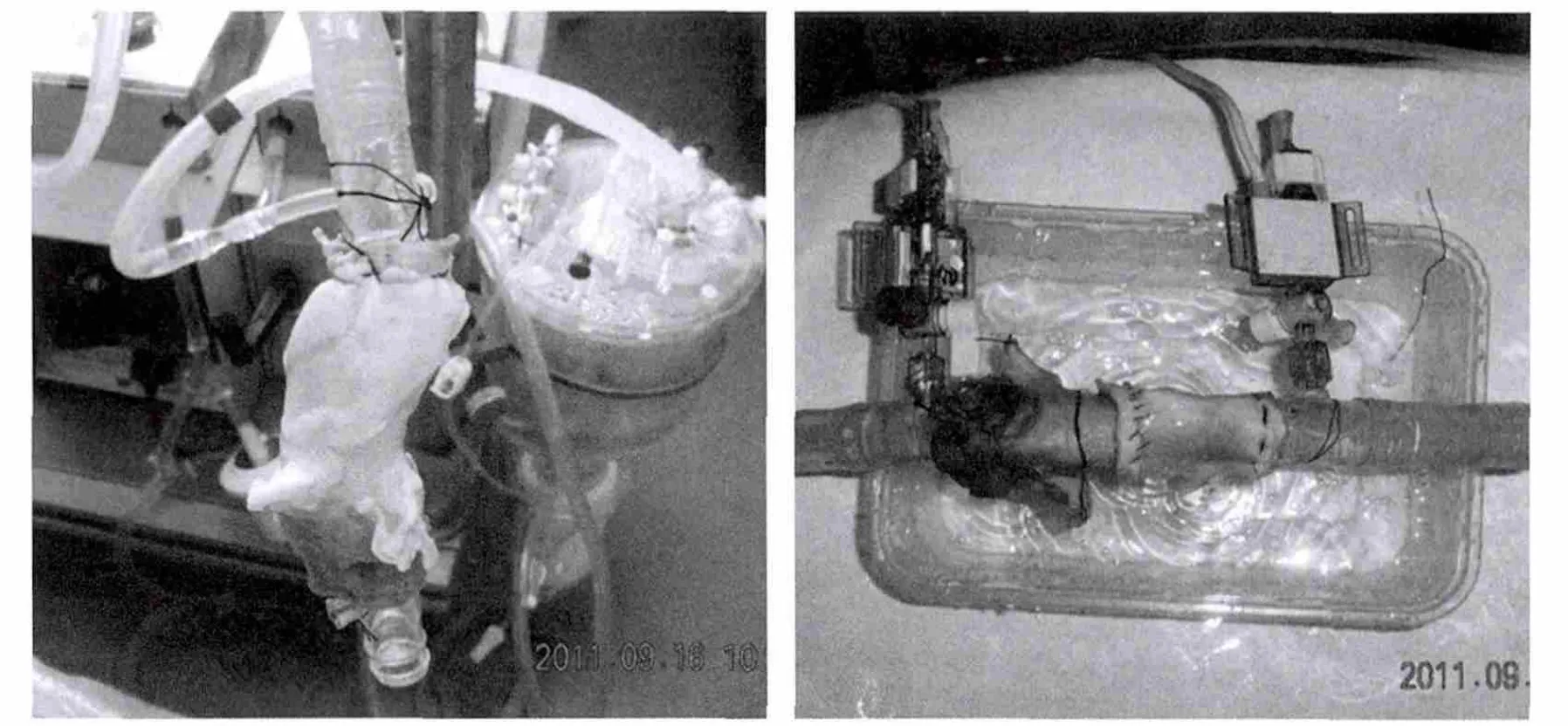
Fig 3 Static and releasing tests of aortic valved stent in PVC tube图3 主动脉瓣膜支架静态和释放试验

Fig.4 Radiography of aortic valved stent in the ascending aorta图4 主动脉瓣膜支架治疗图
The coronary flow rates pre-implantation and post-implantation were shown in Table 1.The left coronary artery flow rate decreased from 25.38 ±5.50 ml/s to 19.71 ± 4.80 ml/s(P=0.0000)and the right decreased from 21.30 ±5.41 ml/s to 17.74±4.10 ml/s(P=0.0001)when the new type of aortic valved stents were released in the middle of the valve leaflets.The left coronary arteryflow rate decreased from 27.71 ± 6.28 ml/s to 27.58 ± 6.16 ml/s(P=0.07426)and the right decreased from 22.37 ± 4.85 ml/s to 21.73 ± 4.77 ml/s(P=0.1487)with no significant difference when the new type of aortic valved stents were released above the valve leaflets.

Table 1 Coronary flow rates pre-implantation and post-implantation表1 植入前后冠脉流量
Implantation of aortic valved stent in vivo
The implantation ofaortic valved stentwas successfully performed in six pigs using retrograde implantation approach and no obviously adverse reaction was observed after implantation.However,one pig died 10 h after the implantation due to the stent was not expanded completely.The leaflets in stents were opening well and no valvular regurgitation was observed after successful deployment of the stents in the rest five pigs.Furthermore,there was no apparent change in the outflow tract pressure,systolic and diastolic function of left ventricle.
The rest 5 pigs were euthanized 24 h post implantation for anatomic evaluation.The morphological characteristics of aortic valved stent were shown in Fig.5.Most of the stent was covered with thin layer of endothelial cells.The post implantation anatomical features of three valve leaflets of aortic valved stent were shown in Figure 6.The aortic valved stents were fixed well in the ascending aorta.A small amount of fibroblast-like substances could be observed in the aortic valved stents and no thrombosis was found.
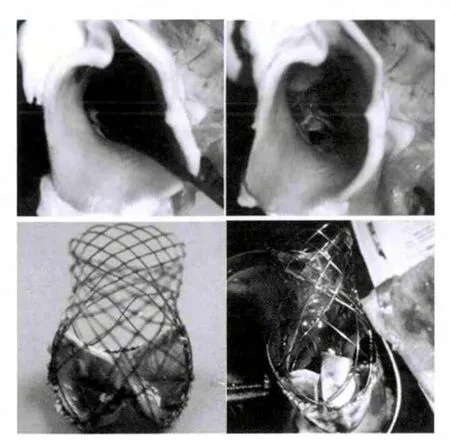
Fig.5 Post implantation morphological characteristics of aortic valved stent图5 主动脉瓣膜支架植入后形态学
Discussion
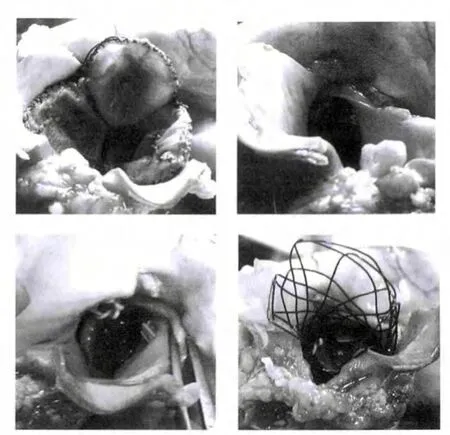
Fig.6 Post implantation anatomical features of three valve leaflets of aortic valved stent图6 三叶主动脉瓣膜支架植入后解剖特征
TAVI was first proposed in 1992 by Andersen and Cribier reported the firstclinicalcase of successful application of TAVI in 2002.Two typical representative aortic valved stents were Cribier-Edwards and CoreValve[18,19].The Cribier-Edwards valve is a trileaflet valve composed of three equal sectionsofequine pericardium integrated into a stainless steel balloon expandable stent frame[20,21].CoreValve is a self-expanding aortic valve prosthesis intended for retrograde delivery across the aortic valve[22,23].It has been reported that the coronary artery flow could be effective by aortic valved stents when TAVI was performed in animal experiments and clinical treatments,especially in the cases of aortic insufficiency[24,25]. Flecher et al reported that implantation of a percutaneous valved stent in the orthotopic position with native valve in place causes coronary ostial obstruction[26].This problem highlights the need for modified stents that are designed for implantation in patients with non-retracted,fibrotic,or calcified leaflets.
In our study,we designed a new type of aortic valve stent according to the anatomy parameters of porcine aortic root and porcine pericardium valves were sutured with the distal end of self-expandable stent.TAVI was performed in the isolated porcine heartin vitroand the coronary artery flow rates were measured.There was no significant difference in the left and right coronary artery flow rates between preimplantation and post-implantation when the new type of aortic valved stents were released above the valve leaflets(P=0.7426,P=0.1487).The left and right coronary artery flow rates decreased significantly after implantation when the new type of aortic valved stents were released in the middle of the valve leaflets(P=0.000,P=0.0001).The results indicated that the new type of aortic valve stent implanted above the valve leaflets could avoid the impacts caused by valve leaflets on the opening of coronary artery.Quaden,et al reported that operation of a high-pressure water stream to endovascularly resected human calcified aortic valves could easily lead to thromboembolism for it is hardly to capture all the tissue fragments of disordered valves[27]. Bonhoeffer, et al[28]has developed an innovative system for percutaneous stent implantation combined with valve replacement but the operation is very complicated and not easy to be popularized.No obvious shifting was observed when the new type of aortic valved stent was released in the middle of the valve leaflets suggesting that the special shape of our aortic valved stent increased the stability at the aortic root.Therefore,a better stability of stent could be obtained when the aortic valve stent was implanted above the valve leaflets.
TAVI is usually performe dusing antegrade or retrograde implantation approach. Currently, the antegrade transseptal approach has been adopted in most cases.Cribier et al successfully performed TAVI in patients with end-stage calcific aortic stenosis using antegrade transseptal approach[10,29].Boudjemline et al performed retrograde replacement on the carotid artery oflamb which resulted in many complications including obstruction of coronary sinus,mitral insufficiency and stent shifting[30].However,Hanzel et al reported a retrograde implantation of TAVI in an 84-year-old man with critical aortic stenosis and refractory congestive heart failure after difficulties encountered with an initialantegrade approach;Utilizing a retrograde approach,TAV was successfully conducted in a stable position below coronary ostia and well above the mitral valve leaflets[31].Webb et al reported that the aortic valve area was significantly increased,no intraproceduraldeaths,16 patients(89%)remain alive after follow-up of 75±55 days since TAVI was performed in 18 high risk patients(aged 81±6 years)byusingtheretrograde implantation approach[32].Therefore,the retrograde approach may be considerably safer by avoiding potential guidewire injury to the mitral valve though this approach may be associated with greater risk of vascular access site complications.In our study,implantion of aortic valved stentsin vivofurther proved that the new type of aortic valved stent could be implanted in the ascending aorta by retrograde method via delivery catheter and successfully released.However,the stentdid notexpanded completely in one pig.Hence,the development of shape memory functional stents which are related to the manufacture of the Ni-Ti alloy stent,suture of valves,size of stents and delivery catheter,need to be emphasized.
In conclusion,the new type of aortic valved stent designed in this study is characterised with good stability and can avoid the impact caused by valve leaflets on the coronary artery.In our study,the ascending aorta of miniature pig was used as animal model.However,the state of the valves in the isolated heartin vitromodel was different from that in the heart of a live animal.And there certainly be some differences of cardiac system between human and pigs though the cardiac structure of pig was similar to that of human being.Therefore,the application of aortic valved stent in human need to be further studied.
[1] Altowaijri A,Phillips CJ,Fitzsimmons D.A systematic review of the clinical and economic effectiveness of clinical pharmacist intervention in secondary prevention of cardiovascular disease[J].J Manag Care Pharm,2013,19(5):408 -416.
[2] Davis EM,Knezevich JT,Teply RM.Advances in antiplatelet technologies to improve cardiovascular disease morbidity and mortality[J].Clin Pharmacol,2013,5(1):67 -83.
[3] Nishimura RA.Cardiology patient pages.Aortic valve disease[J].Circulation,2002,106(7):770 -772.
[4] Baan J.Percutaneous implantation of the CoreValve aortic valve prosthesis in patients at high risk or rejected for surgical valve replacement:Clinical evaluation and feasibility of the procedure in the first 30 patients in the AMC-UvA[J].Neth Heart J,2010,18(1):18-24.
[5] Varadarajan P.Clinicalprofileand naturalhistory of 453 nonsurgically managed patients with severe aortic stenosis[J].Ann Thorac Surg,2006,82(6):2111 -2115.
[6] Goodney PP,Wennberg DE.Do hospitals with low mortality rates in coronary artery bypass also perform well in valve replacement[J].The Annals of thoracic surgery,2003,82(7):2111-2115.
[7] Bouma BJ.To operate or not on elderly patients with aortic stenosis:the decision and its consequences[J].Heart,1999,82(2):143-148.
[8] Iung B.A prospective survey of patients with valvular heart disease in Europe:The Euro Heart Survey on Valvular Heart Disease[J].Eur Heart J,2003,24(13):1231 -1243.
[9] Andersen HR,Knudsen LL,Hasenkam JM.Transluminal implantation of artificial heart valves.Description of a new expandable aortic valve and initial results with implantation by catheter technique in closed chest pigs[J].Eur Heart J,1992,13(5):704-708.
[10] Cribier A.Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis:first human case description[J].Circulation,2002,106(24):3006 -3008.
[11] Ye J.Transapical transcatheter aortic valve implantation:1-year outcome in 26 patients[J].J Thorac Cardiovasc Surg,2009,137(1):167-173.
[12] Grube ESG,Buellesfeld L,Gerckens U,et al.Percutaneous aortic valve replacement for severe aortic stenosis in high-risk patients using the second and current third generation selfexpanding CoreValve prosthesis:device success and 30 day outcome[J].J Am Coll Cardiol,2007,50(1):69 -76.
[13] Descoutures F. Contemporary surgical or percutaneous management of severe aortic stenosis in the elderly[J].Eur Heart J,2008,29(11):1410 -1417.
[14] Khawaja MZ.Transcatheter aortic valve implantation for stenosed and regurgitant aortic valve bioprostheses CoreValve for failed bioprosthetic aortic valve replacements[J].J Am Coll Cardiol,2010,55(2):97 - 101.
[15] Flecher EM.Coronary flow obstruction in percutaneous aortic valve replacement.An in vitro study[J].Eur J Cardiothorac Surg,2007,32(2):291 -294.
[16] Antunes M J.Percutaneous aortic valve implantation.The demise of classical aortic valve replacement[J].Eur Heart J,2008,29(11):1339-1341.
[17] BAI Yuan,ZG-j,WANG Yan-yan,et al.Percutaneous aortic valve replacement using a W-model valved stent:a preliminary feasibility study in sheep[J].Hinese Medical Journal,2009,122(6):655-658.
[18] Webb J,CribierA.Percutaneous transarterialaortic valve implantation:what do we know?[J].Eur Heart J,2011,32(2):140-147.
[19] Cribier A.Development of transcatheter aortic valve implantation(TAVI):a 20-year odyssey[J].Arch Cardiovasc Dis,2012,105(3):146-152.
[20] Eltchaninoff H.Transcatheter aortic valve implantation:technical aspects,results and indications[J].Arch Cardiovasc Dis,2008,101(2):126-132.
[21] Cheung AW.Transcathetertransapicalmitralvalve-in-valve implantations for a failed bioprosthesis:a case series[J].J Thorac Cardiovasc Surg,2011,141(3):711 -715.
[22] Grube E.Percutaneous implantation ofthe CoreValve selfexpanding valve prosthesis in high-risk patients with aortic valve disease:the Siegburg first-in-man study[J].Circulation,2006,114(15):1616-1624.
[23] Jilaihawi HA.Asgar,R.Bonan.Good outcomeandvalve function despite Medtronic-corevalve underexpansion[J].Catheter Cardiovasc Interv,2010,76(7):1022 -1025.
[24] Wilhelmi MH.Role of inflammation and ischemia after implantation of xenogeneic pulmonary valve conduits:histological evaluation after 6 to 12 months in sheep[J].Int J Artif Organs,2003,26(5):411 -420.
[25] Shinoka T.Tissue engineering heartvalves:valve leaflet replacement study in a lamb model[J].Ann Thorac Surg,1995,60(6 Suppl):S513-S516.
[26] Said SA.Surgical treatment of bilateral aneurysmal coronary to pulmonary artery fistulas associated with severe atherosclerosis[J].Ann Thorac Surg,2007,83(1):291 -293.
[27] Quaden R.Percutaneousaorticvalvereplacement:resection before implantation[J].Eur J Cardiothorac Surg,2005,27(5):836-40.
[28] Bonhoeffer P.Percutaneous replacement of pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction[J].Lancet,2000,356(9239):1403 -1405.
[29] Cribier A.Early experience with percutaneoustranscatheter implantation of heart valve prosthesis for the treatment of endstage inoperable patients with calcific aortic stenosis[J].J Am Coll Cardiol,2004,43(4):698 - 703.
[30] Boudjemline Y,Bonhoeffer P.Steps toward percutaneous aortic valve replacement[J].Circulation,2002,105(6):775 -778.
[31] Hanzel GS.Retrograde percutaneous aortic valve implantation for critical aortic stenosis[J].Catheter Cardiovasc Interv,2005,64(3):322-326.
[32] Webb JG.Percutaneous aortic valve implantation retrograde from the femoral artery.[J].Circulation,2006,113(6):842 - 850.
一种新型的对冠脉无影响的主动脉瓣膜支架
蔡建志,周永新,邵 杰,梅运清,王永武
同济大学附属同济医院心胸外科,上海 200065
目的 通过体外测试和动物实验,采用经导管逆行主动脉瓣植入的方法,评价一种新型主动脉瓣膜支架的可行性和安全性。方法 采用猪的心包制作一种新型主动脉瓣膜支架。所有支架在体外均进行流体力学、扩张和释放实验。将这些支架采用逆行经导管的方法植入6头猪体内。这些猪在植入12 h后进行分析。结果 离体实验显示这种新型主动脉瓣膜支架的瓣叶的闭合是有效的,支架可以通过导管释放,然后完全开展并迅速固定。左右冠状动脉血流量在瓣膜支架植入后没有显著的变化。在体内试验中,逆行经导管植入主动脉瓣膜支架于6头猪体内。然后,有一头猪在植入10 h候因为支架没有完全打开导致死亡。在其余5头猪中,瓣膜支架打开良好,无主动脉瓣逆流,也没有血栓形成。结论 该新型主动脉瓣膜支架稳定性好,可以避免瓣叶对冠状动脉的影响。
主动脉瓣膜支架;经导管主动脉瓣植入;逆转
R654.2
A
2095-378x(2013)04-0232-08
国家自然科学基金资助项目(81370334)
蔡建志(1970-),男,博士,主治医师,从事胸外科。
王永武,E-mail:wangyongwu993@sohu.com
猜你喜欢
云南医药(2021年3期)2021-07-21 05:40:52
心肺血管病杂志(2020年5期)2021-01-14 00:43:30
心肺血管病杂志(2019年6期)2019-07-12 09:04:34
心肺血管病杂志(2019年4期)2019-06-27 07:36:10
中华胸部外科电子杂志(2019年2期)2019-06-25 11:31:00
中华胸部外科电子杂志(2019年1期)2019-04-02 07:47:00
中国循证心血管医学杂志(2019年1期)2019-01-04 21:53:34
心血管病学进展(2016年4期)2016-02-21 00:19:58
中国卫生标准管理(2015年17期)2016-01-20 09:26:51
厦门大学学报(自然科学版)(2015年2期)2015-10-13 01:24:38