复方甘草酸苷对过敏性紫癜患儿外周血T辅助细胞功能影响
2013-03-24 07:58:04刘娟娟张秋业
中国医药科学 2013年24期
刘娟娟 肖 静 张秋业
青岛大学医学院附属医院儿科,山东青岛 266003
Henoch-Schonlein purpura(HSP) is one kind of common allergia vasculitis in the pediatrics Department, the disease mostly strikes preschool children and school age children,its clinical manifestations are nonthrombocytopenic palpable purpura,arthralgia,stomachache and nephritis etc.The etiology and pathogenesis of HSP are still not thoroughly clear. At present,some studies have shown that obvious immunity disorder exists in the body of HSP sick children[1-3], mainly including humoral immun disorders, T cell subset dysfunction,abnormal cytokine expression etc.In recent years, the role of T helper cell dysfunction in HSP disease has attracted widely attention.There is no special clinical treatment for HSP currently,in recent years,some researches showed that compound glycyrrhizin was effective for treatment of HSP[4],but there are few reports about teatment mechanism.In this study,level variation of IFN-γ,IL-4 and IL-17 in peripheral blood plasma of children with HSP before and after treatment was detected,effect of compound glycyrrhizin on function of T helper cell in peripheral blood of HSP sick children was also discussed,thus its therapeutic mechanism for HSP was observed,which provides theoretical foundation for clinic treatment of HSP.
1 Materials and methods
1.1 Object of study
1.1.1 HSP group In this study we choose 39 cases of acute stage HSP sick childrens who hospitalized in Affiliated Hospital Qingdao University Medical College from October 2012 to June 2013, including 23 cases of boys,16 cases of girls, age range from 3years to 14 years,the average age was 7.4 years old. The patients were randomly divided into two groups(the differences of degree of the disease’s severity beteen the two groups had no statistical significance),20 cases in compound glycyrrhizin treatment group,19 cases in glucocorticoid treatment group. In compound glycyrrhizin treatment group,11 cases of them were boys,9 cases were girls,the average age was 8.1 years old,clinical features were as follows: 14 cases were suffered from single skin disease, 4 cases were suffered from skin disease and abdominal disease,2 cases were suffered from skin disease and arthropathy.In glucocorticoid treatment group,12 cases were boys,7 cases were girls, age range was 3-14 years old,average age was 6.8 years old,clinical features were as follows:12cases were suffered from single skin disease,4 cases were suffered from skin disease and abdominal disease,3cases were suffered from skin disease and arthropathy.
1.1.2 Control group 22 cases of children in same age who do medical examination in outpatient service were selected as the control group,14 cases were boys, 8 cases were girls,age range was 5-12 years old, average age was 8.2 years old. Filtering criteria:free from infection and hypersensitivity etc in recent years,without application history of immune agents.
1.2 Methods
1.2.1 Treatment method (1)Compound Glycyrrhizin treatment group:based on conventional therapy, corresponding dosage of compound glycyrrhizin were intravenously injected according to their age, dosage: 3-5 years old,80mg qd;5-8 years old, 120mg qd;>8years old, 160mg qd. course of treatment:7-10 days; (2)Glucocorticoid treatment group:based on conventional therapy(same as above),they were treated with methylprednisolone(1-2mg/kg/d,bid ),course of treatment:7-10 days.
1.2.2 Sample collection 2-3 ml of peripheral blood of HSP sick children on admission date and 7-10 days after treatment were sampled, put the sample into heparin anticoagulant tube, centrifugation was performed for 10min at a rate of 2000r/min at room temperature,1 ml of plasma was collected and stored at -80 ℃ for detection,plasma of normal childrens were sampled by the same method,stored for detection.
1.2.3 Cytokine detection IFN-γ,IL-4,IL-17 level in plasma of HSP sick children and normal children were detected by enzyme linked immunosorbent assay(ELISA) method, strictly operated according to kit instructions (The kits were purchased from Suzhou calvin Biotechnology company.Ltd. LOT: 20130602B). 1.2.4 Statistical method sample average T- test was performed by using SPSS17.0 statistical package for statistical treatment,data were presented as(±s),P<0.05 refers to the difference has statistical significance,P< 0.01 refers to the difference has significant statistical significance.
2 Results
2.1 The plasma cytokines levels of HSP group compare with normal control group
The level of IL-4 and IL-17 of HSP group was significantly higher than that of the control group(P<0.05, P<0.01),and there were no significant differences in the level of IFN-γ between the two groups(P> 0.05). There were no significant differences in the level of IFN-γ,IL-4 and IL-17 between two treatment groups before the treatment(P>0.05).Table 1.
2.2 The changes of plasma cytokine levels afer glycyrrhizin or glucocorticoid teatment
There was no significant difference in the level of IFN-γ of glycyrrhizin group between before and after the treatment (P> 0.05),while IL-4,IL-17 levels were significantly lower (P<0.01,P<0.05);The level of IFN-γ,IL-4 and IL-17 of glucocorticoid group were significantly decreased than that of before treatment (P<0.05,P<0.01,P<0.05) (Table 2).
2.3 The plasma cytokine changes amplitude of glycyrrhizin group and glucocorticoid group between before and after the treatment
In the glucocorticoid group the level of IFN-γ,IL - 4,IL -17 in the plasma decline were significantly greater than the glycyrrhizin group between before and after the treatment (P<0.05, P<0.01, P<0.05).Table 3.
Table2 The changes of plasma cytokine levels before and afer teatment(±s,pg/mL)

Table2 The changes of plasma cytokine levels before and afer teatment(±s,pg/mL)
△Compared with the same group before teatment t=3.24, P<0.05; ▲a ▲b ▲c Compared with the same group before treatment or t'=4.02,5.22,5.07,all P<0.01
Glucocorticoid group (n=19) Before teatment after teatment Before teatment after teatment IFN-γ 295.75±62.45 260.36±61.90 314.64±86.03 248.57±72.02 IL-4 16.90±4.18 11.89±3.67▲a 17.29±4.13 10.52±3.82▲b IL-17 21.31±4.10 16.85±4.56△ 22.02±4.48 14.93±4.11▲c Cytokines Glycyrrhizin group(n=20)
Table1 The plasma cytokines levels of HSP group before treatment and normal control group’s levels(±s,pg/mL)
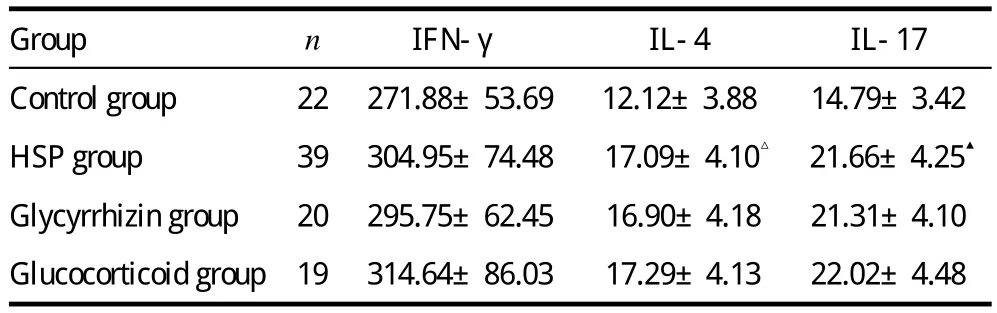
Table1 The plasma cytokines levels of HSP group before treatment and normal control group’s levels(±s,pg/mL)
△compare with normal control group t=4.62,P< 0.05;▲compare with normal control group, t=6.57,P<0.01
Group n IFN-γ IL-4 IL-17 Control group 22 271.88±53.69 12.12±3.88 14.79±3.42 HSP group 39 304.95±74.48 17.09±4.10△ 21.66±4.25▲Glycyrrhizin group 20 295.75±62.45 16.90±4.18 21.31±4.10 Glucocorticoid group 19 314.64±86.03 17.29±4.13 22.02±4.48
Table3 Before and afer teatment the plasma cytokine changes amplitude of the two treatment groups(±s,pg/mL)

Table3 Before and afer teatment the plasma cytokine changes amplitude of the two treatment groups(±s,pg/mL)
△a △b compare with glycyrrhizin group t or t'=2.14,3.05, P<0.05;▲compare with glycyrrhizin group, t=2.72, P<0.01
Group n IFN-γ IFN-γ IL-17 Glycyrrhizin group 20 35.84±28.98 5.01±2.01 4.45±2.15 Glucocorticoid group 19 66.07±54.68△a 6.75±2.00▲ 7.18±3.33△b
3 Discussion
HSP pathogenesis is still not clearly up to the present. It has been clear that T lymphocyte subsets dysfunction was involved in the pathogenesis of HSP.It is probably one effective ways of cure HSP through regulating T cell subsets.As the significant immune cells in the human body,T helper cell,can assist the function of T and B lymphocyte response,and plays a critical role in organism immune response and regulate. T helper cells can be divided into Th0,Th1,Th2,Th3 and Th17. Th1 cell mainly secretes IL-2、IFN-γ and TNF-α, mainly participates in cellular immun process;Th2 cell secretes IL-4,IL-5 and IL-6 and mainly regulates the humoral immunity of organism[5].Normally,there exists interacting and regulating roles between Th1 and Th2 cells.Th1 and Th2 dysfunction may result into immune dysfunction of organism and induce autoimmune disease. Th17 is discovered in recent years refers to a kind of helper T lymphocyte subsets independents of Th1 and Th2 and mainly participates in the inflammatory reaction[6] through special secretion IL-17.At present,some studies found that the excessive expression of IL-17 by Th17 was closely related to many autoimmune diseases. For instance,many researchers such as Zhan-Ju Liu et al[7]have found that IL-17 in the body of patients with inflammatory bowel disease shows high-level expression; the research results such as Shahrara[8]et al showed that the level of IL-17 was increased in the body of patients with rheumatoid arthritis; additionally, other researches also showed that Th17 excessive activation may be participate in pathogenesis of Kawasaki disease[9]. Due to the lack of specific cell surface tag, the function of Th cell subsets are evaluated according to the expression degree of IFN-γ,IL-4 and IL-17 in blood plasma.Such as,Thl (IFN-γ),Th2 (IL-4) and Th17 (IL-17). IFN-γ and IL-4 play a role of antagonism during the occurrence and regulation of immune in organism. IFN-γ can refrain from Th2 cell differentiation,but IL-4 refrains from Th1 differentiation and plays the role of Th2 cell differentiation;IFN-γ can activate and enhance macrophage function while IL-4 can resist such function.In addition,IL-4 can facilitate B cell differentiation,maturity and proliferation and stimulate B cell differentiation to produce cell for antibody,but IFN-γ has no such function[10].IL-17, a kind of proinflammatory cytokine,can induce and facilitate the release of cell factors and participate in collection of neutrophile granulocyte,excitation of T cell and enhance the generation of antibody.Thus, it plays the role[11]of facilitating the occurrence and development of inflammation. IL-17 also can coordinate with many cell factors,thus it plays the role of magnifying the inflammatory reaction.The result in this paper shows that the IL-4 and 17 expression level of HSP patients at the acute phase is remarkably higher than that in the normal control group. There is no obvious changes in IFN-γ between treatment group and normal control group. It prompted that helper T cell dysfunction exists in the body of HSP patients and Th2 and Th17 showed relatively advantageous state of activation.
Compound glycyrrhizin,a kind of compound preparation, is mainly comprised of glycyrrhizic acid, cysteine, glycine and methionine,etc.Glycyrrhetinic acid is the metabolites of glycyrrhizic acid in the body. It plays the role of resisting inflammation and allergy and alleviating inflammatory response by stabilizing cell membrane, restraining mast cell from secreting histamine,inhibiting excitation of arachidonic acid metabolic enzymes and eliminating oxygen free radicals and reducing the harm of superoxide to partial blood vessels[12]. Compound glycyrrhizin also can increase the level of hydrocortisone in plasma,thus playing the role of enhancing the pharmacological action of hydrocortisone.Besides,glycyrrhizic acid can play the role of glucocorticoid without side effect of hormone by inhibiting the damage of adrenocortical hormone directly or indirectly after entering the human body. Meanwhile, glycyrrhizic acid has the role of immune regulation. It also can promote the thymus T cell differentiation, activate NK and T cells and also plays the role of inducingγ-interferon[13]. Compound glycyrrhizin has been used to cure HSP clinically with good curative effect in recent years.After many researchers including Tang Chunhui et al observed 72 HSP patients,they found that compound glycyrrhizin could rapidly alleviate the clinical symptoms and signs of HSP patients with apparently bettered prognosis and less adverse effect[14]during the therapeutic process.In the meantime, some researchers found compound glycyrrhizin had immunomodulatory effects on HSP after observing the changes in T cell subset and immune globulin before and after HSP patients used the drugs.This research found that periperal blood cell factors IL-4 and 17 are remarkably reduced compared to those before treatment after curing with compound glycyrrhizin. It indicated that compound glycyrrhizin had apparent inhibiting effect on excessive activation state of Th2 and Th17 at the acute phase of HSP, but its inhibiting strength was not better than that of glucocorticoid.
Glucocorticoid is one of immun supprressor which mostly widely used to cure HSP clinically. The research showed that glucocorticoid not only could reduce the arthralgia of HSP patients and also shortened the ache time[15].Additionally,it could rapidly mitigate acute gastrointestinal symptom of HSP patients, apparently reduced the abdominal pain and reduced the risks in occurrence of indigitation and intestinal hemorrhage[16]. The researchers such as Guan Fengjun et al found that the patients with rash and gastrointestinal symptoms could prevent the occurrence of renal damage or alleviated renal damage by applying glucocorticoid after analyzing the application of glucocorticoid into preventing renal damage meta for the children at the early stage of anaphylactoid purpura[17].This experimental result showed that glucocorticoid could lower the inflammatory factors IL-4 and IL-17 obviously and had remarkable regulating effect on Th2 and Th17. In addition, it also could reduce IFN-γ level and play the role of regulating Th1 cell. However, glucocorticoid has huge side effect,thus having impacts on each system of the body.For instance,it can result into disorder disturbance of internal secretion, metabolism, water and electrolyte and induce obesity,polytrichia,rise in blood glucose and water-sodium retention,etc.Additionally,it also can seduce gastrointestinal tract lesion, hypertension, arrhythmia, osteoporosis, and muscle atrophy, thus influencing the growth of children, and can give rise into adrenal cortex atrophy and dysfunction, etc.
To sum up,the curative effect of compound glucocorticoid on curing the HSP children is definite. Its mechanism of action is possibly related to regulating peripheral blood T cell subset, inhibiting excessive activation state of Th2 and Th17 and lowering the proinflammatory cytokines IL-4 and IL-17. However, due to its little side effect,it is the first choice for those who can not tolerate side effect of hormone or the patients whoose parents refuse to use glucocorticoid.
[1] Qian Yi,Feng Qihua.Research on immune state of children with Henoch-Schonlein acute in phase[J].Chinese Journal of Practical Pediatrics,2009,24(3):203-205.
[2] Yang Jun,Li Chengrong,Zu Ying,et al.Role of regulatory T cells in pathogenesis of Henoch-Schonlein purpura in children[J].Chin J Pediatr,2006,44(6):411-414.
[3] BAI Cui,ZONG Jinbao,ZHANG Qiuye.Functional changes of immune cells in children with Henoch-Schonlein purpura in acute stage[J].Med J Qilu,2010,25(2):137-139.
[4] Zhang Li. Effection of compound Glycyrrhizin on immunoloregulation children with Henoch-Schonlein purpura[J].Chin J Postgrad Med, 2012,35(3):50-51.
[5] Mckenzie AN.Regulation of T helper type2 cell immunity by interleukin–4 and interleukin-13[J]. Phrmacolyher, 2000,88(2):143-151.
[6] Bettelli E,Korn T.Kuchroo VK.Thl7:The third member of the effector T cell trilogy[J].Curr,Opin lmmunol,2007,19(6):652-657.
[7] Zhan-Ju Liu,Praveen K Yadav,Jing-Ling Su,et al.Potential role of Th17 cells in the pathogenesis of inflammatory bowel disease[J]. World J Gastroenterol,2009,15(46):5784-5788.
[8] Shahrara S,Huang Q,Mandelin AM,et al.Th17 cells in rheumatoid arthritis[J].Arthritis Res Ther,2008,10(4):533-541.
[9] Wang Guobing,Li Chengrong,Yang Jun,et al,Investigation of the change of Th17 cells during acute phase of Kawasaki disease[J].Chin J Microbiol Immunol, 2009,29(10):939-943.
[10] Paludan SR.Interleukin-4 and interferon-gamma:the quintessence of a mutual antagonistic relationship[J].Scand J Immunol,1998,48(5):459-468.
[11] Moseiey TA,Haudenschild DR, Rose L,et al.Interleukin-17 family and IL-17 receptor[J].Cytokine Growth factor Rev,2003,14(2):155-174.
[12] Zhang Jinxia.The pharmacology,clinical uses and side Affects of compound Glycyrrhizin[J].Guide of China Medicine,2011,9(27):198-200.
[13] Narges B,Mohammad HK,Zahra A,et al.The effect of glycyrrhizin on maturation and T cell stimulating activity of dendritic cells[J].Cellular Immunology,2012,280:44-49.
[14] Tang Chunhui,Huangpu Chunrong.Clinic observation on compound Glycyrrhizin injection treatment for children with Henoch-Schonlein purpura[J].Journal of Pediatric Pharmacy, 2011,17(3):25-27.
[15] Sunderkotter C,Bonsmann G,Sindrilaru A,et al.Management of leukocytoclastic vasculitis.J Dermatol Treat,2005,16:193-206.
[16] Ronkainen J,Koskimies O,Ala-Houhala M,et a1.Early prednisone therapy in Henoch-Schonlein purpura: a randomized,double-blind,placebocontrolled trial[J].J Pediatr,2006,149:241-247.
[17] Guan Fengjun,YI Zhunwen,Dang Xiqiang,et al.Corticosteroid preventing renal involvement of Henoch-Schonlein purpura in early stage:a metaanalysis[J].Chin J Evid Based Pediatr, 2006,1(4):258-263.
猜你喜欢
国家教育行政学院学报(2022年7期)2022-08-18 14:51:46
校园英语·上旬(2020年5期)2020-08-02 10:50:43
家庭医学(下半月)(2020年4期)2020-05-30 12:42:42
校园英语·下旬(2019年2期)2019-04-08 07:18:12
商周刊(2018年25期)2019-01-08 03:31:10
中国民族医药杂志(2016年4期)2016-05-09 07:41:00
中国卫生标准管理(2015年4期)2016-01-14 05:16:45
西南医科大学学报(2016年4期)2016-01-03 01:26:29
西藏科技(2015年11期)2015-09-26 12:11:36
中国当代医药(2015年33期)2015-03-01 02:09:17