比较唑来膦酸与利塞膦酸在激素诱导的骨质疏松中的疗效
2013-03-04 00:39:02陈根强许慧娟马华鹰汪志明
重庆医学 2013年8期
陈根强,许慧娟,马华鹰,汪志明
(1.金华职业技术学院医学院,浙江金华321000;2.浙江省金华市中心医院 321000)
糖皮质激素广泛被用于治疗炎症及免疫调节紊乱性疾病[1-2]。然而,长期连续使用会导致如骨质疏松、增加骨折风险等不良反应[3]。研究发现,连续使用3个月的糖皮质激素会增加上述的风险[4-5]。双磷酸盐类为目前在防治糖皮质激素诱导的骨质疏松药物中疗效最为显著,能够增加骨密度及降低脊柱骨折的风险[6-7]。每天口服双磷酸盐类药物能够对糖皮质激素诱导的骨质疏松有预防与治疗的效果,但现今仍缺少此类药物的治疗周期用药规范。唑来膦酸与利塞膦酸为双磷酸盐类药物,现将本研究采用唑来膦酸联合利塞膦酸治疗糖皮质激素诱导的骨质疏松中的疗效报道如下。
1 资料与方法
1.1 一般资料 选取本院2007年1月至2010年1月糖皮质激素诱导的骨质疏松患者120例,随机双盲试验,分为唑来膦酸组60例,其中,男22例,女38例;平均年龄(53.3±21.7)岁。口服安慰剂及静脉滴注唑来膦酸5mg/d;风湿性关节炎26例,风湿性肌肉痛3例,系统性红斑狼疮9例,哮喘5例。利塞膦酸组60例,其中,男25例,女35例;平均年龄(52.6±28.1)岁。风湿性关节炎25例,风湿性肌肉痛3例,系统性红斑狼疮10例,哮喘4例,口服利塞膦酸5mg/d及每天静脉滴注安慰剂。疗程均为连续治疗12个月。纳入标准:最近一年中每天口服7.5mg泼尼松(或等量糖皮质激素)超过3个月。所有患者均签署知情同意书。排除标准:排除12个月内接受过双磷酸盐类药物或对骨骼有影响药物;血清维生素D浓度小于30nmol/L;恶心肿瘤或甲状旁腺疾病患者;肾功能不全患者(肌酐清除率小于30mL/min)。
1.2 指标检测 采用电化学发光免疫分析技术(electrochemiluminescence immunoassay,ECLIA)测定血清β-CTx及骨形成标志物P1NP浓度;骨密度仪检测腰椎L1~4及股骨颈骨密度。
1.3 统计学处理 应用SPSS11.0统计软件进行数据分析,计量资料以±s表示,组间比较采用ANOVA方差分析,以P<0.05为差异有统计学意义。
2 结 果
2.1 两组治疗后骨密度比较 治疗后3、6、9、12个月唑来膦酸组患者骨密度高于利塞膦酸组(P<0.05),见图1和表1。
2.2 治疗后的β-CTx及P1NP浓度变化比较 唑来膦酸组患者治疗后3、6、9、12个月血清β-CTx和P1NP浓度远低于利塞膦酸组患者血清浓度(P<0.05)。见图2和表2。
表1 两组患者治疗后骨密度变化比较(±s,%)

表1 两组患者治疗后骨密度变化比较(±s,%)
*:P<0.05,与利塞膦酸组比较。
组别 n 治疗前个月腰椎治疗后3个月 6个月 9个月 12个月股骨颈治疗后3个月 6个月 9个月 12*唑来膦酸组 60 0 1.9±0.7* 3.5±0.7* 3.8±0.8* 4.2±1.0* 0.6±0.3* 1.0±0.5* 1.2±0.4* 1.5±0.4利塞膦酸组 60 0 1.2±0.6 2.3±0.8 2.5±0.9 2.7±1.1 0.2±0.1 0.3±0.1 0.3±0.2 0.5±0.2
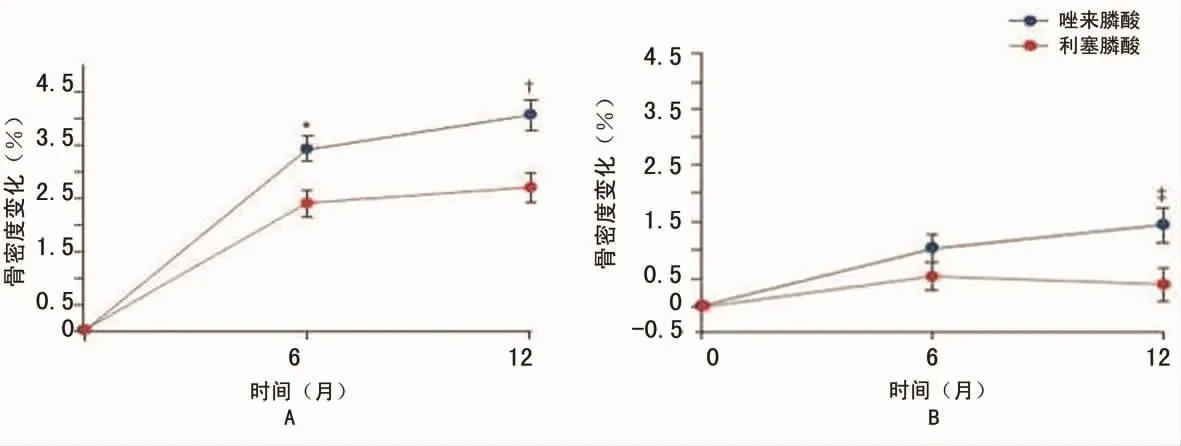
图1 两组患者治疗后骨密度变化
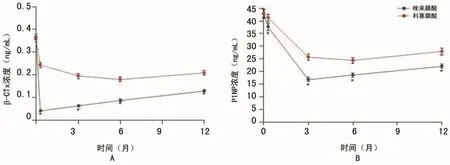
图2 两组患者治疗后β-CTx及P1NP浓度变化比较
表2 两组患者治疗后β-CTx及P1NP浓度变化比较(±s)
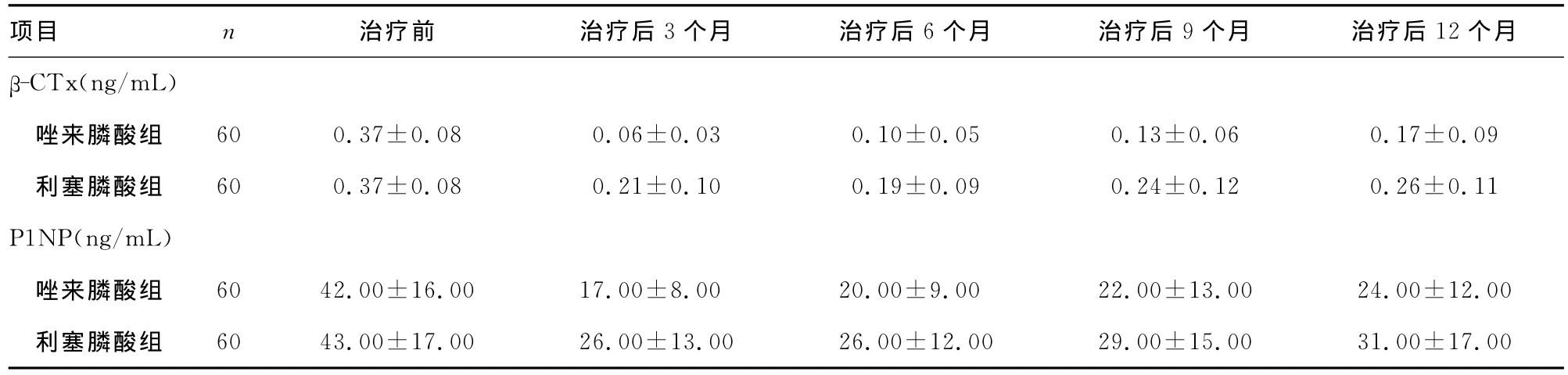
表2 两组患者治疗后β-CTx及P1NP浓度变化比较(±s)
个月β-CTx(ng/mL)项目 n 治疗前 治疗后3个月 治疗后6个月 治疗后9个月 治疗后12唑来膦酸组 60 0.37±0.08 0.06±0.03 0.10±0.05 0.13±0.06 0.17±0.09利塞膦酸组 60 0.37±0.08 0.21±0.10 0.19±0.09 0.24±0.12 0.26±0.11 P1NP(ng/mL)唑来膦酸组 60 42.00±16.00 17.00±8.00 20.00±9.00 22.00±13.00 24.00±12.00利塞膦酸组 60 43.00±17.00 26.00±13.00 26.00±12.00 29.00±15.00 31.00±17.00
3 讨 论
唑来膦酸属于含氮双膦酸化合物,主要作用于人体骨骼,通过对破骨细胞的抑制,从而抑制骨吸收。唑来膦酸静脉注射后可以迅速分布于骨骼当中,并像其他双膦酸化合物一样,优先聚集于高骨转化部位。注射唑来膦酸能够增加绝经后出现骨质疏松妇女的骨密度及降低骨折的风险[8-9]。在细胞水平,本品抑制破骨细胞。破骨细胞通常存在于骨表面上,但不具有明显的吸收活性[10-13]。
β胶原特殊序列(β-Crosslaps)是骨重吸收标志物,它是l型胶原蛋白的羧基端降解产物。总骨I型前胶原氨基端延长链(PINP)是骨形成标志物,反映了新合成的I型胶原蛋白的变化[14-15]。β-CTx及P1NP是国际骨质疏松症基金会(international osteoporosis foundation,IOF)推荐使用的3种骨标志物中的其中2种。本次同时对2个指标进行比较,发现唑来膦酸治疗后能快速降低β-CTx及P1NP血清浓度。利塞膦酸与唑来膦酸比较,治疗效果明显差于前者。
综上所述,本研究发现,唑来膦酸静脉滴注能够显著增加腰椎及股骨颈骨密度基值,降低β-CTx及P1NP血清浓度,治疗效果远优胜于利塞膦酸。同时从骨密度增长幅度及β-CTx及P1NP血清浓度降低的特点上发现,在使用唑来膦酸治疗时,采取短疗程已收到良好治疗效果,治疗疗程不建议超过6个月。
[1]van Staa TP,Leufkens HG,Abenhaim L,et al.Use of oral corticosteroids and risk of fractures[J].J Bone Miner Res,2009,15(12):993-1000.
[2]Boonen S,Lorenc RS,Orwoll ES,et al.Evidence for safety and efficacy of risedronate in men with osteoporosis over 4years of treatment:results from the 2-year,open-label,extension study of a 2-year,randomized,double-blind,placebo-controlled study[J].Bone,2012,51(3):383-388.
[3]van Staa TP,Leufkens HG,Abenhaim L,et al.Oral corticosteroids and fracture risk:relationship to daily and cumulative doses[J].Rheumatology(Oxford),2000,39(12):1383-1389.
[4]Dissette V,Bozzi B,Pasti L,et al.Particulate adducts based on sodium risedronate and titanium dioxide for the bioavailability enhancement of oral administered bisphosphonates[J].Eur J Pharm Sci,2010,41(2):328-336.
[5]The digitalis investigation group.American college of rheumatology Ad Hoc committee on glucocorticoid-induced osteoporosis.Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis:2001 update[J].Arthritis Rheum,2001,44(16):1496-1503.
[6]Watts NB,Brown JP,Cline G.Risedronate on 2consecutive days a month reduced vertebral fracture risk at 1year compared with historical placebo[J].J Clin Densitom,2010,13(1):56-62.
[7]Devogelaer JP,Goemaere S,Boonen S,et al.Evidence-based guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis:a consensus document of the Belgian Bone Club[J].Osteoporos Int,2006,17(1):8-19.
[8]van Staa TP.The pathogenesis,epidemiology and management of glucocorticoid-induced osteoporosis[J].Calcif Tissue Int,2006,79(2):129-137.
[9]Carbonell-Abella C,Guañabens-Gay N,Marín-Rives JA,et al.Analysis of therapeutic compliance in women with osteoporosis[J].Reumatol Clin,2011,7(5):299-304.
[10]Cohen S,Levy RM,Keller M,et al.Risedronate therapy prevents corticosteroid-induced bone loss:a twelvemonth,multicenter,randomized,double-blind,placebocontrolled,parallel-group study[J].Arthritis Rheum,1999,42(11):2309-2318.
[11]Gaines JM,Marx KA.Older men′s knowledge about osteoporosis and educational interventions to increase osteoporosis knowledge in older men:a systematic review[J].Maturitas,2011,68(1):5-12.
[12]Reid DM,Hughes RA,Laan RF,et al.Efficacy and safety of daily risedronate in the treatment of corticosteroid-induced osteoporosis in men and women:a randomized trial.European Corticosteroid-Induced Osteoporosis Treatment Study[J].J Bone Miner Res,2000,15(6):1006-1013.
[13]Majumdar SR,McAlister FA,Johnson JA,et al.Interventions to increase osteoporosis treatment in patients with′incidentally′detected vertebral fractures[J].Am J Med,2012,125(9):929-936.
[14]Saag KG,Emkey R,Schnitzer TJ,et al.Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis.Glucocorticoid-Induced Osteoporosis Intervention Study Group[J].N Engl J Med,1998,339(24):292-299.
[15]Hamilton B,McCoy K,Taggart H.Tolerability and compliance with risedronate in clinical practice[J].Osteoporos Int,2003,14(3):259-262.
猜你喜欢
中老年保健(2022年3期)2022-08-24 03:00:58
保健医苑(2021年7期)2021-08-13 08:48:02
现代临床医学(2021年1期)2021-01-26 00:56:28
中华养生保健(2020年8期)2021-01-14 01:13:10
中国生殖健康(2019年2期)2019-08-23 08:12:02
中华老年多器官疾病杂志(2016年9期)2016-04-28 08:52:44
中国医学装备(2015年10期)2015-12-29 12:00:32
云南中医学院学报(2015年5期)2015-07-31 17:45:28
医学研究杂志(2015年7期)2015-06-22 11:01:10
现代检验医学杂志(2015年6期)2015-02-06 01:44:22